

Recomendados
Más contenido relacionado
La actualidad más candente
La actualidad más candente (20)
Similar a Glaucoma
Similar a Glaucoma (20)
Último
Último (20)
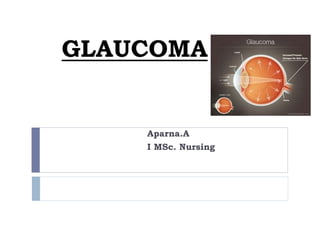
Glaucoma
- 2. What is glaucoma? Classified as a group of diseases. Damages the optic nerve. Can cause permanent vision loss if left untreated.
- 3. Magnitude Second major cause of blindness Often asymptomatic in early stage. Damage is irreversible. More prevalent among men than women Incidence increase with age
- 4. DEFINITION It is a heterogeneous group of diseases in which damage to the optic nerve(optic neuropathy) is usually caused by raised ocular pressure IOP: Depends on the balance between production and removal of aqueous humour
- 5. NORMAL IOP = between 10 and 21mmHg IOP > 21.7 is abnormal.
- 7. Eye Anatomy The optic nerve is a bundle of nerve fibers. It carries visual information from the retina to the brain.
- 8. Acqeous flow
- 9. Aqueous Humour Dynamics Produced by non-pigmented epithelia of pars plicata Aqueous production rate - 2µL/min Facility of outflow – 0.22µL/min/mm of Hg
- 10. Fluid Circulation The eye has an internal fluid circulation system. Fluid is produced at the base of the iris.
- 11. Fluid Circulation The fluid flows through the pupil to the front of the iris.
- 12. Fluid Circulation The fluid exits the eye at the angle between the iris and the cornea where it drains through a spongy meshwork.
- 13. Angle of the Anterior Chamber of Eye The aqueous humor outflow occurs by two routes Trabecular: Trabeculum is the site for pressure dependent aqueous outflow functioning as a one way valve that allows aqueous to leave the eye but does not allow the flow inside it. Uveoscleral: Pressure independent outflow. The aqueous passes across the cilliary muscles into the supracilliary and suprachoroidal spaces and drain into the venous circulation.
- 14. Unimpeded outflow of aqueous fluid depends on an intact drainage system and an open angle (about 45 degrees) between the iris and the cornea. A narrower angle places the iris closer to the trabecular meshwork, diminishing the angle.
- 15. IOP IOP is determined by the rate of aqueous production, the resistance encountered by the aqueous humour as it flows out of the passages, and the venous pressure of the episcleral veins that drain into the anterior ciliary vein.
- 16. *Age *Sex *Race *Heredity *Diurnal & Seasonal variation *Blood pressure *Obesity *Drugs *Posture *Exercise Factor affect IOP *Hormone *Refractive error *Eye movement *Eyelid closure *Inflammation *Surgery
- 17. Cause of glaucoma Slow fluid drainage. Pressure builds up and damages the optic nerve. Optic nerve damage can occur at different pressure levels for different people.
- 18. Higher risk people Family history of glaucoma African American race Older age Diabetes Cardiovascular disease Migraine syndromes Nearsightedness (myopia) Eye trauma Prolonged use of topical or systemic corticosteroids
- 19. Pathophysiology
- 20. Theories of damage 1. Mechanical theory • Compression of axons leads to axonal death 2. Vascular theory • Ischemia causes axonal necrosis Direct damage due to pressure Capillary Occlusion Interference to Axoplasmic flow
- 21. Stages 1. Initiating events: precipitating factors include illness, emotional stress, congenital narrow angles, long-term use of corticosteroids, and mydriatics (ie, medications causing pupillary dilation).
- 22. Stages 2. Structural alterations in the aqueous outflow system: Tissue and cellular changes caused by factors that affect aqueous humour dynamics lead to structural alterations.
- 23. 3. Functional alterations: conditions such as increased IOP or impaired blood flow create functional changes Stages
- 24. 4. Optic nerve damage: Atrophy of the optic nerve is characterized by loss of nerve fibers and blood supply, and this stage inevitably progresses to the fifth stage. Stages
- 25. 5. Visual loss: progressive loss of vision is characterized by visual field defects. Stages
- 26. Glaucomatous Damage Axonal necrosis leading to cupping Loss of supporting glial tissue Normally leads to disc pallor Histology of Normal and Glaucomatous Optic nerve
- 28. GLAUCOMA Optic nerve signs of glaucoma progression Development of disk pallor Disc hemorrhage (60% will show progression of VF damage) Vessel displacement Increased visibility of lamina cribosa
- 29. Pallor and cupping Cupping and pallor correspond Pallor - maximal area of colour contrast Cupping is greater than pallor Cupping - bending of small blood vessels crossing disc
- 30. CLASSIFICATION ACORDING TO AETIOLOGY *Primary *Secondary ACCORDING TO APPERANCE OF THE ANGLE MECHANISMS CAUSE IMPAIRED AQUEOUS OUTFLOW *Open angle glaucoma. *Closed angle glaucoma. *Combined mechanism glaucoma *Developmental- Congenital, manifest at birth Infantile, present in first year of life. Juvenile, present in late childhood.
- 33. Congenital Features Buphthalmos corneal diameter 12 mm < 1 yr characterized by dysgenesis of the angle of the anterior chamber, raised IOP, corneal opacities and enlargement of the globe Optic disc cupping
- 35. Etiology: 10% show autosomal recessive inheritance with variable penetration Chromosomal abnormalities at 1p6 and 2p21 The disease is caused by the maldevelopment of the angle of the anterior chamber (angle dysgenesis). The characteristic gonioscopic appearance of an eye with congenital glaucoma is marked by the presence of open angle, Barkan’s membrane, abnormally high insertion of the iris, poorly developed and posteriorly placed sclera spur and collapsed Schlemm’s canal.
- 36. MANAGEMENT OF CONGENITAL GLAUCOMA GONIOTOMY TRABECULOTOMY
- 37. GLAUCOMA CLASSIFICATION PRIMARY VERSUS SECONDRY *PRIMARY No detectable ocular or systemic abnormality. Often bilateral. Often familial *SECONDARY Predisposing ocular or systemic abnormality. Often unilateral. Often sporadic
- 38. Primary Glaucoma Is the iris: Covering the Trabecular meshwork NOT covering the Trabecular meshwork OPEN angle glaucoma CLOSED angle glaucoma With high pressure With normal pressure
- 39. Signs & symptoms 1. “Silent thief of sight” 2. Frequent change of presbyopic glasses Open Angle Glaucoma Risk Factors Age Race Family History Diabetes Myopia Hypertension Smoking
- 40. Primary OPEN angle glaucoma It is the most common type of glaucoma It is the 2nd cause of blindness in the India It is also called chronic open angle glaucoma. It causes SLOW damage to the optic nerve, causing gradual loss of vision.
- 41. Definition of POAG POAG is defined as a chronic progressive optic neuropathy associated with elevated IOP and visual field defects
- 42. Primary Open Angle Glaucoma (POAG) POAG is the most common form of glaucoma It occurs when the fluid drainage is poor and fluid builds up in the eye and the internal eye pressure goes up. This increased pressure can cause damage to the optic nerve and vision loss. The exact mechanism of damage is still unknown.
- 43. Risk Factors for POAG High Intraocular (Eye) Pressure Over the age of 40 Family history of glaucoma African or Caribbean descent Thin cornea High myopia (Nearsightedness) Diabetes High blood pressure
- 44. Primary OPEN angle glaucoma Pathogenesis: Resistance of drainage of aqueous through the Trabecular meshwok, due to: Thickening of Trabecular lamellae (reduces pore size). Reduction in number of lining Trabecular cells. Increased extracellular material in the Trabecular meshwork spaces.
- 45. Interference with aqueous outflow degenerative changes in the trabeculum, schlemm’s canal and exit channels vascular insufficiency optic nerve damage (cupping).
- 46. Normal -tension Glaucoma IOP<21 Mostly elderly people Vasospastic disease – Migraine, Raynaud’s phenomena, Autoimmune disease
- 47. Ocular Hypertension Some people can have high eye pressure but the optic nerve does not get damaged. This condition is called ocular hypertension. These patients must be closely followed because of the risk of developing glaucoma.
- 48. Occular Hypertension It is defined as one who has an elevated IOP in the absence of identifiable optic neuropathy and visual field defects. It is benign rise of IOP usually found in about 6-10% of population above 40yrs of age and is more common than open angle glaucoma.
- 49. Symptoms of Primary Open Angle Glaucoma POAG develops gradually and painlessly and has no initial symptoms Vision is normal in the early stages
- 50. Symptoms of Primary Open Angle Glaucoma If untreated, peripheral or side vision is slowly lost Tunnel vision
- 51. Symptoms of Primary Open Angle Glaucoma Eventually, all vision may be lost
- 52. Angle Closure Glaucoma This type of glaucoma is an emergency situation. It occurs when the iris itself blocks the drainage angle and results in a sudden increase in pressure. Symptoms include severe eye pain, nausea, eye redness and very blurred vision. Immediate treatment is required.
- 53. Primary Angle Closure Glaucoma(PACG) Risk factors include race (varies in different race), age (increases with age), gender (2-4 times frequently in females), family history (first degree relatives) personality (anxious).
- 54. PRIMARY ANGLE CLOSURE GLAUCOMAS PRIMARY ANGLE- CLOSURE GLAUCOMA ANATOMIC FEATURES: • SMALL CORNEAL DIAMETER • SHALLOW ANTERIOR CHAMBER • THICKER LENS • SMALL RADIUS OF THE ANTERIOR LENS CURVATURE • ANTERIOR LENS POSITION • SHORT AXIAL LENGTH • HYPEROPIC EYES
- 55. PRIMARY ANGLE CLOSURE GLAUCOMAS STAGES A. PRIMARY ANGLE-CLOSURE GLAUCOMA SUSPECT B. SUBACUTE ANGLE-CLOSURE GLAUCOMA C. ACUTE ANGLE-CLOSURE GLAUCOMA D. CHRONIC ANGLE-CLOSURE GLAUCOMA E. ABSOLUTE GLAUCOMA
- 56. CLINICAL COURSE Primary angle closure glaucoma suspect Small hyperopic eyes with small anterior chamber associated with an occludable angle are usually prone to develop primary angle closure glaucoma The patient is usually symptom free. Treatment is laser iridotomy.
- 57. CLINICAL COURSE…. Subacute or intermittent primary angle closure glaucoma Transient attacks of unilateral head ache, blurring of vision, coloured halos, associated with sudden and sharp rise of IOP in an eye with a shallow anterior chamber and an occludable angle characterize the subacute primary angle closure glaucoma. The attack is precipitated by several factors like dim illumination, emotional stress and drugs. The attack is usually subsides without any medication, probably by spontaneous resolution of the pupillary block due to miosis during sleep.
- 58. CLINICAL COURSE…. Acute primary angle closure glaucoma An acute congestive attack is characterized by a sudden neuralgic pain, profound diminution of vision, intense cilliary congestion, corneal edema, very shallow anterior chamber, complete closure of the angle of anterior chamber, vertically dilated non reacting pupil and markedly raised IOP. An acute congestive attack occurs always with the closure of the angle by peripheral anterior synechiae and edematous and congested root of the iris and ciliary processes. The changes in the iris are secondary to the vascular strangulation which results from the raised IOP.
- 59. CLINICAL COURSE…. Chronic primary angle closure glaucoma It develops either after recurrent attacks of subacute or acute primary angle closure glaucoma or when the angle closes gradually and IOP rises slowly. A gradual asymptomatic angle closure is known as creeping angle closure glaucoma
- 60. CLINICAL COURSE…. Absolute primary angle closure glaucoma The terminal stage of primary angle closure glaucoma is marked by the complete loss of vision and stony hard eye. Etiology is untreated acute primary angle closure glaucoma or chronic primary angle closure glaucoma which ends up in absolute glaucoma.
- 61. Features of Absolute primary angle closure glaucoma The eyes are painful and blind. A chronic congestion is seen in circumcorneal region and often the anterior ciliary vessels are dilated. The cornea is edematous and has bullous or filamentary keratopathy; it is hazy and insensitive. The anterior chamber is shallow. The iris may show atropic patches. The pupil is dilated and does not react to light and accommodation. Ectropion of uveal pigment is frequent at the papillary boarder. IOP is very high and the eyeball is stony hard. The optic nerve head is deeply cupped.
- 62. Treatment of Absolute primary angle closure glaucoma cyclodestructive surgeries to reduce IOP and enucleation in case of painful eyes
- 63. Secondary Glaucoma Glaucoma can develop as a complication from other conditions including: Eye injuries Uveitis (internal eye inflammation) Pigment dispersion Diabetes (Neovascular glaucoma) Steroid use
- 64. Pseudoexfoliation Glaucoma Elderly white women Fibrillar material deposited on trabecular meshwork Moth-eaten iris transillumination defects Pigment on trabecular meshwork
- 65. STEROID INDUCED GLAUCOMA Risk Factors POAG Diabetes Myopia Stronger the steroid more the elevation
- 66. Malignant Glaucoma Aqueous misdirected posteriorly behind vitreous Vitreous moves forward, collapses iris & lens into AC Typically after intraocular surgery particularly cataract & glaucoma
- 67. Lens related Glaucoma Intumescence Dislocation and Subluxation Phacolytic Lens particle
- 68. Symptoms At first, there are none. As glaucoma progresses, side vision fails. Field of vision narrows as glaucoma worsens.
- 69. What does vision with glaucoma look like? Normal Vision Vision with Glaucoma
- 70. Glaucoma detection Regular eye examinations by an optometrist or ophthalmologist are vital to detecting glaucoma. A number of tests are performed.
- 71. Glaucoma can be detected through a comprehensive dilated eye exam.
- 72. STEPWISE DIAGNOSIS IOP with Applanation tonometry with Corneal Pachymetry Good S/L examination & Stereoscopic Dialated Ophtalmoscopic examination Gonioscopy Formal visual-field testing(WWP) Imaging
- 73. How is glaucoma detected?
- 74. Glaucoma Tests: History A patient’s medical history, family history and background are important to determine the presence of risk factors.
- 75. Glaucoma Tests: Visual Acuity A refraction is done to determine best corrected vision. This shows central vision function.
- 76. Glaucoma Tests: Slit Lamp & Gonioscopy A special microscope called a slit lamp is used to examine the structures of the eye. A gonioscopy lens may be used to view the drainage angle.
- 77. Glaucoma Tests: Tonometry Eye pressure is measured with an instrument called a tonometer. Three types that are commonly used are: Goldmann (Perkins) Non-contact (air puff) Tonopen
- 78. Tonometers Goldmann Contact applanation Perkins Portable contact applanation Pulsair 2000 (Keeler)Air-puff Schiotz Portable non-contact applanationNon-contact indentation Contact indentation Tono-Pen portable contact applanation
- 79. Glaucoma Tests: Ophthalmoscopy Eye drops may be placed in the eyes to dilate the pupils. Special magnifying lenses are used to examine the retina and optic nerve for damage. Normal Optic Nerve Suspicious Optic Nerve
- 80. Glaucoma Tests: Ophthalmoscopy Advances are being made in digital imaging of the retina.
- 81. Glaucoma Tests: Visual Field Test Peripheral (side) vision is tested with a perimeter. The patient responds to flashes of light in different locations
- 82. Optic Nerve
- 83. Field Test
- 85. Normal Disc
- 86. Cupped Disc
- 88. Glaucoma treatment Medications Surgery ◦ Laser ◦ Conventional
- 89. MANAGEMENT OF CONGENITAL GLAUCOMA GONIOTOMY TRABECULOTOMY
- 90. Treatment
- 91. Treatment Medical Beta blockers (Timolol) Carbonic anhydraze inhibitors Azopt and Trusopt Sympathomimetics Propine and Apraclonidine Parasympathomimetics (pilocarpine) Prostaglandin Derivatives (Xalatan)
- 92. Glaucoma Medications Medications are usually the first type of treatment used Eyedrops or pills are used to either decrease the fluid production or to increase the fluid drainage
- 93. Glaucoma Medications There are several different types of medication available. The right choice will depend on what other medications are being taken, other medical conditions and the effectiveness in decreasing the eye pressure. Often, combinations of eyedrops are used.
- 94. Treatment Laser Trabeculoplasty Sclerostomy Cycloablation
- 95. Laser Trabeculoplasty This laser treatment helps to increase the fluid drainage The surgeon uses a laser to burn the spongy meshwork that is located in the drainage angle
- 96. Treatment Surgical Goniotomy for congenital Trabeculotomy for congenital glaucoma's Trabeculectomy for adult glaucoma's Implants for difficult non responsive
- 100. Conventional Surgery With this treatment, the surgeon creates a new opening in the eye for the fluid to drain out from If the new opening becomes plugged or narrowed, further surgery may be required
- 101. Coping with Vision Loss Many patients with sight loss due to glaucoma can benefit from low vision aids Optometrists can perform low vision assessments and prescribe magnifying devices to enhance both distance and reading vision
- 102. Coping with Vision Loss These aids will not restore sight to normal levels but they allow people to maximize the amount of vision remaining
- 103. Early Detection & Treatment Regular eye health examinations are important to detect glaucoma early so that treatment can be started and vision loss can be prevented.
- 104. NURSING MANAGEMENT
- 105. Acute angle closure glaucoma Nursing Assessment Establishing demographic data Family history of glaucoma or other eye problems OTC drugs History of allergy to drugs/ dye Evaluate patient for severe pain, nausea and vomiting, signs of increased IOP. Assess visual symptoms. Establish history of onset of attack and previous attacks. Assess patient's level of anxiety and knowledge base.
- 106. Nursing Diagnoses Acute Pain related to increased IOP Goal: Relieving Pain Nursing Interventions: Notify health care provider immediately of patient's condition. Administer opioids and other medications as directed. Medications that may cause nausea and vomiting are avoided. Patient may be medicated with antiemetic if nausea occurs.
- 107. Acute Pain related to increased IOP Explain to patient that the goal of treatment is to reduce IOP as quickly as possible. Explain procedures to patient. Reassure patient that, with reduction in IOP, pain and other signs and symptoms should subside.
- 108. Acute Pain related to increased IOP Explain adverse effects of medications: Mannitol (Osmitrol) (I.V.) for transient blurred vision, rhinitis, thirst, nausea, transient circulatory overload, and headache Acetazolamide (Diamox) or methazolamide (Neptazane) (oral) - drowsiness, anorexia, paresthesia, stomach upset, tinnitus, fluid and electrolyte imbalance, rare kidney or liver dysfunction Pilocarpine (Pilocar, Isopto carpine, Ocupress) (topical) - burning and redness of eye, headache, constricted pupil, poor vision in dim light, retinal detachment, rare lens opacity
- 109. Fear related to pain and potential loss of vision Goal: Relieving Fear Intervention: Provide reassurance and calm presence to reduce anxiety and fear. Prepare patient for surgery, if necessary.
- 110. Fear related to pain and potential loss of vision Describe procedure to patient; surgery will likely be done on outpatient basis. Patch will be worn for several hours, and sunglasses may help with photophobia. Vision will be blurred for first few days after the procedure. Frequent initial follow-up will be necessary for tonometry to make sure control of IOP.
- 111. Fear related to pain and potential loss of vision Recommend the following: Continuous daily use of eye medications as prescribed Moderate use of the eyes Exercise in moderation to maintain general well-being Unrestricted fluid intake: alcohol and coffee may be permitted unless they are noted to cause increased IOP in the particular patient Maintenance of regular bowel habits to decrease straining Wearing a medical identification tag indicating the patient has glaucoma
- 112. Evaluation: Expected Outcomes Verbalizes understanding of glaucoma as a chronic disease; demonstrates proper instillation of ophthalmic medication.
- 113. Key points to patients: Know intraocular pressure (IOP) measurement and the desired range. Be informed about the extent of vision loss and optic nerve damage. Keep a record of eye pressure measurements and visual field test results to monitor progress.
- 114. Key points to patients: Review all medications (including over-the- counter and herbal medications) with ophthalmologist, and mention any side effects each visit. Ask about potential side effects and drug interactions of eye medications. Ask whether generic or less costly forms of eye medications are available.
- 115. Key points to patients: Review the dosing schedule with ophthalmologist and inform him or her if you have trouble complying with the schedule. Participate in the decision-making process. Let the doctor know what dosing schedule works for you and other preferences regarding eye care. Have the nurse observe instilling eye medication to determine whether you are administering it properly.
- 116. Key points to patients: Be aware that glaucoma medications can cause adverse effects if used inappropriately. Eyedrops are to be administered as prescribed, not when eyes feel irritated. Ask your ophthalmologist to send a report to primary care physician after each appointment. Keep all follow-up appointments.
- 117. CONTINUING GLAUCOMA CARE AT HOME referral to services that assist the patient in performing customary activities may be needed. The loss of peripheral vision impairs mobility the most. These patients need to be referred to low vision and rehabilitation services. Patients who meet the criteria for legal blindness should be offered referrals to agencies that assist in obtaining federal assistance.
- 118. Reassurance and emotional support are important aspects of care. The family must be integrated into the plan of care, and because the disease has a familial tendency, family members should be encouraged to undergo examinations at least once every 2 years to detect glaucoma early.
- 119. Patient Education and Health Maintenance Instruct patient in use of medications. Do not rub the eyes Stress the importance of long-term medication use to control this chronic disease. Remind patient to keep follow-up appointments.
- 120. Patient Education and Health Maintenance Instruct patient to seek immediate medical attention if signs and symptoms of increased IOP return, severe eye pain, photophobia, and excessive lacrimation. Advise patient to notify all health care providers of condition and medications and to avoid use of medications that may increase IOP, such as corticosteroids and anticholinergics (such as antihistamines), unless the benefit outweighs the risk.
- 121. Patient Education and Health Maintenance Evaluation: Expected Outcomes Pain is decreased Describes treatment regimen and verbalizes reduced fear
- 122. Chronic open angle glaucoma Nursing Assessment Assess frequency, duration, and severity of visual symptoms. Assess patient's knowledge of disease process and anxiety about the diagnosis. Assess patient's motivation to participate in long-term treatment.
- 123. Nursing Diagnoses Deficient Knowledge about glaucoma and surgical procedure Goal: Providing Information about Glaucoma Nursing Interventions : Review the normal anatomy and physiology of the eye as well as the changes that occur in the drainage of aqueous humour with glaucoma. Make sure that the patient understands that, although he may be asymptomatic, IOP could still be elevated, and damage to the eye could be occurring. Therefore, ongoing use of medication and follow-up are essential.
- 124. Teach patient the action, dosage, and adverse effects of all medications. Make sure adequate administration of eyedrops by watching return demonstration. Timolol (Timoptic) and betaxolol (Betoptic) and adverse effects include headache, eye irritation, decreased corneal sensitivity, blurred vision, bradycardia, palpitations, bronchospasm, hypotension, and heart failure Pilocarpine (Pilocar, Isopto Carpine) - adverse effects include eye irritation, blurring, and redness; headache; pupil constriction; poor vision in dim light; possible hypertension and tachycardia; and rare retinal detachment and lens opacity Acetazolamide (Diamox) and methazolamide (Neptazane)- adverse effects include drowsiness, anorexia, paresthesia, stomach upset, tinnitus, fluid and electrolyte imbalance, and rare kidney and liver dysfunction
- 125. Discuss visual defects with patient and ways to compensate. Vision loss is permanent, and treatment is aimed at stopping the process. Inform patient that surgery is done on outpatient basis and recovery is quick. Prolonged restrictions are not required. After surgery, elevation of head 30 degrees will promote aqueous humour drainage after a trabeculectomy. Additional medications after surgery will include topical steroids and cycloplegics to decrease inflammation and to dilate the pupil.
- 126. Patient Education and Health Maintenance Patient must remember that glaucoma cannot be cured, but it can be controlled. Remind patient that periodic eye checkups are essential because pressure changes may occur. Alert patient to avoid, if possible, circumstances that may increase IOP: Upper respiratory infections Emotional upsets - worry, fear, anger Exertion, such as snow shoveling, pushing, heavy lifting