

Recomendados
Recomendados
Más contenido relacionado
La actualidad más candente
La actualidad más candente (16)
Destacado
Destacado (16)
Similar a Ssc guidelines2013
Similar a Ssc guidelines2013 (20)
Ssc guidelines2013
- 1. Special Articles Surviving Sepsis Campaign: International Guidelines for Management of Severe Sepsis and Septic Shock: 2012 R. Phillip Dellinger, MD1; Mitchell M. Levy, MD2; Andrew Rhodes, MB BS3; Djillali Annane, MD4; Herwig Gerlach, MD, PhD5; Steven M. Opal, MD6; Jonathan E. Sevransky, MD7; Charles L. Sprung, MD8; Ivor S. Douglas, MD9; Roman Jaeschke, MD10; Tiffany M. Osborn, MD, MPH11; Mark E. Nunnally, MD12; Sean R. Townsend, MD13; Konrad Reinhart, MD14; Ruth M. Kleinpell, PhD, RN-CS15; Derek C. Angus, MD, MPH16; Clifford S. Deutschman, MD, MS17; Flavia R. Machado, MD, PhD18; Gordon D. Rubenfeld, MD19; Steven A. Webb, MB BS, PhD20; Richard J. Beale, MB BS21; Jean-Louis Vincent, MD, PhD22; Rui Moreno, MD, PhD23; and the Surviving Sepsis Campaign Guidelines Committee including the Pediatric Subgroup* Objective: To provide an update to the “Surviving Sepsis Cam- Methods: The authors were advised to follow the principles of the paign Guidelines for Management of Severe Sepsis and Septic Grading of Recommendations Assessment, Development and Shock,” last published in 2008. Evaluation (GRADE) system to guide assessment of quality of evi- Design: A consensus committee of 68 international experts rep- dence from high (A) to very low (D) and to determine the strength resenting 30 international organizations was convened. Nominal of recom endations as strong (1) or weak (2). The potential draw- m groups were assembled at key international meetings (for those backs of making strong recommendations in the presence of low- committee members attending the conference). A formal con- quality evidence were emphasized. Some recommendations were flict of interest policy was developed at the onset of the process ungraded (UG). Recommendations were classified into three and enforced throughout. The entire guidelines process was groups: 1) those directly targeting severe sepsis; 2) those targeting conducted independent of any industry funding. A stand-alone general care of the critically ill patient and considered high priority in meeting was held for all subgroup heads, co- and vice-chairs, severe sepsis; and 3) pediatric considerations. and selected individuals. Teleconferences and electronic-based Results: Key recommendations and suggestions, listed by cat- discussion among subgroups and among the entire committee egory, include: early quantitative resuscitation of the septic served as an integral part of the development. patient during the first 6 hrs after recognition (1C); blood ultures c 1 Cooper University Hospital, Camden, New Jersey. 20 Royal Perth Hospital, Perth, Western Australia. 2 Warren Alpert Medical School of Brown University, Providence, Rhode 21 Guy’s and St. Thomas’ Hospital Trust, London, United Kingdom. Island. 22 Erasme University Hospital, Brussels, Belgium. 3 St. George’s Hospital, London, United Kingdom. 23 UCINC, Hospital de São José, Centro Hospitalar de Lisboa Central, 4 Hôpital Raymond Poincaré, Garches, France. E.P.E., Lisbon, Portugal. 5 Vivantes-Klinikum Neukölln, Berlin, Germany. * embers of the 2012 SSC Guidelines Committee and Pediatric Sub- M 6 Memorial Hospital of Rhode Island, Pawtucket, Rhode Island. group are listed in Appendix A at the end of this article. 7 Emory University Hospital, Atlanta, Georgia. Supplemental digital content is available for this article. Direct URL cita- 8 Hadassah Hebrew University Medical Center, Jerusalem, Israel. tions appear in the printed text and are provided in the HTML and PDF ver- 9 Denver Health Medical Center, Denver, Colorado. sions of this on the journal’s Web site (http://journals.lww.com/ccmjournal). 10 McMaster University, Hamilton, Ontario, Canada. 11 Barnes-Jewish Hospital, St. Louis, Missouri. Complete author and committee disclosures are listed in Supplemental 12 University of Chicago Medical Center, Chicago, Illinois. Digital Content 1 (http://links.lww.com/CCM/A615). 13 California Pacific Medical Center, San Francisco, California. This article is being simultaneously published in Critical Care Medicine 14 Friedrich Schiller University Jena, Jena, Germany. and Intensive Care Medicine. 15 Rush University Medical Center, Chicago, Illinois. For additional information regarding this article, contact R.P. Dellinger 16 University of Pittsburgh, Pittsburgh, Pennsylvania. (Dellinger-Phil@CooperHealth.edu). 17 Perelman School of Medicine at the University of Pennsylvania, Philadelphia, Pennsylvania. Copyright © 2013 by the Society of Critical Care Medicine and the Euro- 18 Federal University of Sao Paulo, Sao Paulo, Brazil. pean Society of Intensive Care Medicine 19 Sunnybrook Health Sciences Center, Toronto, Ontario, Canada. DOI: 10.1097/CCM.0b013e31827e83af 580 www.ccmjournal.org February 2013 • Volume 41 • Number 2
- 2. Special Article before antibiotic therapy (1C); imaging studies performed unless contraindicated (1B); a conservative fluid strategy for promptly to confirm a potential source of infection (UG); admin- patients with established ARDS who do not have evidence of istration of broad-spectrum antimicrobials therapy within 1 hr of tissue hypoperfusion (1C); protocols for weaning and seda- recognition of septic shock (1B) and severe sepsis without sep- tion (1A); minimizing use of either intermittent bolus sedation tic shock (1C) as the goal of therapy; reassessment of antimi- or continuous infusion sedation targeting specific titration crobial therapy daily for de-escalation, when appropriate (1B); endpoints (1B); avoidance of neuromuscular blockers if pos- infection source control with attention to the balance of risks and sible in the septic patient without ARDS (1C); a short course benefits of the chosen method within 12 hrs of diagnosis (1C); of neuromuscular blocker (no longer than 48 hrs) for patients initial fluid resuscitation with crystalloid (1B) and consideration with early ARDS and a Pao2/Fio2 150 mm Hg (2C); a proto- of the addition of albumin in patients who continue to require colized approach to blood glucose management commencing substantial amounts of crystalloid to maintain adequate mean insulin dosing when two consecutive blood glucose levels are arterial pressure (2C) and the avoidance of hetastarch formula- 180 mg/dL, targeting an upper blood glucose ≤ 180 mg/dL tions (1C); initial fluid challenge in patients with sepsis-induced (1A); equivalency of continuous veno-venous hemofiltration or tissue hypoperfusion and suspicion of hypovolemia to achieve a intermittent hemodialysis (2B); prophylaxis for deep vein throm- minimum of 30 mL/kg of crystalloids (more rapid administration bosis (1B); use of stress ulcer prophylaxis to prevent upper and greater amounts of fluid may be needed in some patients) gastrointestinal bleeding in patients with bleeding risk factors (1C); fluid challenge technique continued as long as hemody- (1B); oral or enteral (if necessary) feedings, as tolerated, rather namic improvement, as based on either dynamic or static vari- than either complete fasting or provision of only intravenous ables (UG); norepinephrine as the first-choice vasopressor to glucose within the first 48 hrs after a diagnosis of severe sep- maintain mean arterial pressure ≥ 65 mm Hg (1B); epinephrine sis/septic shock (2C); and addressing goals of care, including when an additional agent is needed to maintain adequate blood treatment plans and end-of-life planning (as appropriate) (1B), pressure (2B); vasopressin (0.03 U/min) can be added to nor- as early as feasible, but within 72 hrs of intensive care unit epinephrine to either raise mean arterial pressure to target or admission (2C). Recommendations specific to pediatric severe to decrease norepinephrine dose but should not be used as sepsis include: therapy with face mask oxygen, high flow nasal the initial vasopressor (UG); dopamine is not recommended cannula oxygen, or nasopharyngeal continuous PEEP in the except in highly selected circumstances (2C); dobutamine presence of respiratory distress and hypoxemia (2C), use of infusion administered or added to vasopressor in the presence physical examination therapeutic endpoints such as capillary of a) myocardial dysfunction as suggested by elevated cardiac refill (2C); for septic shock associated with hypovolemia, the filling pressures and low cardiac output, or b) ongoing signs use of crystalloids or albumin to deliver a bolus of 20 mL/kg of hypoperfusion despite achieving adequate intravascular vol- of crystalloids (or albumin equivalent) over 5 to 10 mins (2C); ume and adequate mean arterial pressure (1C); avoiding use more common use of inotropes and vasodilators for low cardiac of intravenous hydrocortisone in adult septic shock patients if output septic shock associated with elevated systemic vascular adequate fluid resuscitation and vasopressor therapy are able resistance (2C); and use of hydrocortisone only in children with to restore hemodynamic stability (2C); hemoglobin target of suspected or proven “absolute”‘ adrenal insufficiency (2C). 7–9 g/dL in the absence of tissue hypoperfusion, ischemic Conclusions: Strong agreement existed among a large cohort coronary artery disease, or acute hemorrhage (1B); low tidal of international experts regarding many level 1 recommenda- volume (1A) and limitation of inspiratory plateau pressure (1B) tions for the best care of patients with severe sepsis. Although for acute respiratory distress syndrome (ARDS); application of a significant number of aspects of care have relatively weak at least a minimal amount of positive end-expiratory pressure support, evidence-based recommendations regarding the (PEEP) in ARDS (1B); higher rather than lower level of PEEP acute management of sepsis and septic shock are the founda- for patients with sepsis-induced moderate or severe ARDS tion of improved outcomes for this important group of critically (2C); recruitment maneuvers in sepsis patients with severe ill patients. (Crit Care Med 2013; 41:580–637) refractory hypoxemia due to ARDS (2C); prone positioning in Key Words: evidence-based medicine; Grading of Recommendations sepsis-induced ARDS patients with a Pao2/Fio2 ratio of ≤ 100 Assessment, Development and Evaluation criteria; guidelines; mm Hg in facilities that have experience with such practices infection; sepsis; sepsis bundles; sepsis syndrome; septic shock; (2C); head-of-bed elevation in mechanically ventilated patients severe sepsis; Surviving Sepsis Campaign Sponsoring organizations: American Association of Critical-Care America, Indian Society of Critical Care Medicine, International Pan Nurses, American College of Chest Physicians, American College Arabian Critical Care Medicine Society, Japanese Association for Acute of Emergency Physicians, American Thoracic Society, Asia Pacific Medicine, Japanese Society of Intensive Care Medicine, Pediatric Acute Association of Critical Care Medicine, Australian and New Zealand Lung Injury and Sepsis Investigators, Society for Academic Emergency Intensive Care Society, Brazilian Society of Critical Care, Canadian Medicine, Society of Critical Care Medicine, Society of Hospital Critical Care Society, Chinese Society of Critical Care Medicine, Medicine, Surgical Infection Society, World Federation of Critical Chinese Society of Critical Care Medicine−China Medical Association, Emirates Intensive Care Society, European Respiratory Society, Care Nurses, World Federation of Pediatric Intensive and Critical Care European Society of Clinical Microbiology and Infectious Diseases, Societies; World Federation of Societies of Intensive and Critical Care European Society of Intensive Care Medicine, European Society of Medicine. Participation and endorsement: The German Sepsis Society Pediatric and Neonatal Intensive Care, Infectious Diseases Society of and the Latin American Sepsis Institute. Critical Care Medicine www.ccmjournal.org 581
- 3. Dellinger et al Dr. Dellinger consulted for Biotest (immunoglobulin concentrate available in Dr. Douglas received grants paid to his institution from Eli Lilly (PROWESS Europe for potential use in sepsis) and AstraZeneca (anti-TNF compound Shock site), Eisai (study site), National Institutes of Health (ARDS Network), unsuccessful in recently completed sepsis clinical trial); his institution received Accelr8 (VAP diagnostics), CCCTG (Oscillate Study), and Hospira (Dexme- consulting income from IKARIA for new product development (IKARIA has detomidine in Alcohol Withdrawal RCT). His institution received an honorar- inhaled nitric oxide available for off-label use in ARDS) and grant support from ium from the Society of Critical Care Medicine (Paragon ICU Improvement); Spectral Diagnostics Inc (current endotoxin removal clinical trial), Ferring (vaso- he consulted for Eli Lilly (PROWESS Shock SC and Sepsis Genomics pressin analog clinical trial-ongoing); as well as serving on speakers bureau for Study) in accordance with institutional policy; he received payment for pro- Eisai (anti-endotoxin compound that failed to show benefit in clinical trial). viding expert testimony (Smith Moore Leatherwood LLP); travel/accommo- dations reimbursed by Eli Lilly and Company (PROWESS Shock Steering Dr. Levy received grant support from Eisai (Ocean State Clinical Coordi- Committee) and the Society of Critical Care Medicine (Hospital Quality Alli- nating Center to fund clinical trial [$500K]), he received honoraria from Eli ance, Washington DC, four times per year 2009−2011); he received hono- Lilly (lectures in India $8,000), and he has been involved with the Surviving raria from Covidien (non-CME lecture 2010, US$500) and the University Sepsis Campaign guideline from its beginning. of Minnesota Center for Excellence in Critical Care CME program (2009, Dr. Rhodes consulted for Eli Lilly with monetary compensation paid to him- 2010); he has a pending patent for a bed backrest elevation monitor. self as well as his institution (Steering Committee for the PROWESS Shock Dr. Jaeschke has disclosed that he has no potential conflicts of interest. trial) and LiDCO; travel/accommodation reimbursement was received from Eli Lilly and LiDCO; he received income for participation in review activities Dr. Osborn consulted for Sui Generis Health ($200). Her institution such as data monitoring boards, statistical analysis from Orion, and for Eli receives grant support from the National Institutes of Health Research, Lilly; he is an author on manuscripts describing early goal-directed therapy, Health Technology Assessment Programme-United Kingdom (trial doc- and believes in the concept of minimally invasive hemodynamic monitoring. tor for sepsis-related RCT). Salary paid through the NIHR government funded (nonindustry) grant. Grant awarded to chief investigator from Dr. Annane participated on the Fresenius Kabi International Advisory Board ICNARC. She is a trial clinician for ProMISe. (honorarium 2000€). His nonfinancial disclosures include being the princi- pal investigator of a completed investigator-led multicenter randomized con- Dr. Nunnally received a stipend for a chapter on diabetes mellitus; he is an trolled trial assessing the early guided benefit to risk of NIRS tissue oxygen author of editorials contesting classic tight glucose control. saturation; he was the principal investigator of an investigator-led randomized Dr. Townsend is an advocate for healthcare quality improvement. controlled trial of epinephrine vs norepinephrine (CATS study)–Lancet 2007; Dr. Reinhart consulted for EISAI (Steering Committee member−less then he also is the principle investigator of an ongoing investigator-led multina- US $10,000); BRAHMS Diagnostics (less than US $10,000); and SIRS- tional randomized controlled trial of crystalloids vs colloids (Crystal Study). Lab Jena (founding member, less than US $10,000). He received hono- Dr. Gerlach has disclosed that he has no potential conflicts of interest; raria for lectures including service on the speakers’ bureau from Biosyn he is an author of a review on the use of activated protein C in surgical Germany (less than €10,000) and Braun Melsungen (less than €10,000). patients (published in the New England Journal of Medicine, 2009). He received royalties from Edwards Life Sciences for sales of central venous oxygen catheters (~$100,000). Dr. Opal consulted for Genzyme Transgenics (consultant on trans- genic antithrombin $1,000), Pfizer (consultant on TLR4 inhibitor project Dr. Kleinpell received monetary compensation for providing expert testimony $3,000), British Therapeutics (consultant on polyclonal antibody project (four depositions and one trial in the past year). Her institution receives $1,000), and Biotest A (consultant on immunoglobul project $2,000). grants from the Agency for Healthcare Research and Quality and the Prince His institution received grant support from Novartis (Clinical Coordinat- Foundation (4-year R01 grant, PI and 3-year foundation grant, Co-l). She ing Center to assist in patient enrollment in a phase III trial with the use received honoraria from the Cleveland Clinic and the American Association of Tissue Factor Pathway Inhibitor [TFPI] in severe community acquired of Critical Care Nurses for keynote speeches at conferences; she received pneumonia [SCAP] $30,000 for 2 years), Eisai ($30,000 for 3 years), royalties from McGraw Hill (co-editor of critical care review book); travel/ Astra Zeneca ($30,000 for 1 year), Aggenix ($30,000 for 1 year), Inimex accommodations reimbursed from the American Academy of Nurse Prac- ($10,000), Eisai ($10,000), Atoxbio ($10,000), Wyeth ($20,000), Sirtris titioners, Society of Critical Care Medicine, and American Association of (preclinical research $50,000), and Cellular Bioengineering Inc. ($500). Critical Care Nurses (one night hotel coverage at national conference). He received honoraria from Novartis (clinical evaluation committee TFPI Dr. Angus consulted for Eli Lilly (member of the Data Safety Monitoring study for SCAP $20,000) and Eisai ($25,000). He received travel/accom- Board, Multicenter trial of a PC for septic shock), Eisai Inc (Anti-TLR4 modations reimbursed from Sangart (data and safety monitoring $2,000), therapy for severe sepsis), and Idaho Technology (sepsis biomarkers); he Spectral Diagnostics (data and safety monitoring $2,000), Takeda (data received grant support (investigator, long-term follow-up of phase III trial and safety monitoring $2,000) and Canadian trials group ROS II oseltami- of an anti-TLR4 agent in severe sepsis), a consulting income (anti-TRL4 vir study (data and safety monitoring board (no money). He is also on the therapy for severe sepsis), and travel/accommodation expense reimburse- Data Safety Monitoring Board for Tetraphase (received US $600 in 2012). ment from Eisai, Inc; he is the primary investigator for an ongoing National Institutes of Health-funded study comparing early resuscitation strategies Dr. Sevransky received grant support to his institution from Sirius Genom- for sepsis-induced tissue hypoperfusion. ics Inc; he consulted for Idaho Technology ($1,500); he is the co-principal investigator of a multicenter study evaluating the association between Dr. Deutschman has nonfinancial involvement as a coauthor of the Society intensive care unit organizational and structural factors, including proto- of Critical Care Medicine’s Glycemic Control guidelines. cols and in-patient mortality. He maintains that protocols serve as useful Dr. Machado reports unrestricted grant support paid to her institution for reminders to busy clinicians to consider certain therapies in patients with Surviving Sepsis Campaign implementation in Brazil (Eli Lilly do Brasil); sepsis or other life-threatening illness. she is the primary investigator for an ongoing study involving vasopressin. Dr. Sprung received grants paid to his institution from Artisan Pharma Dr. Rubenfeld received grant support from nonprofit agencies or foundations ($25,000–$50,000), Eisai, Corp ($1,000–$5,000 ACCESS), Ferring including National Institutes of Health ($10 million), Robert Wood Johnson Pharmaceuticals A/S ($5,000–$10,000), Hutchinson Technology Incorpo- Foundation ($500,000), and CIHR ($200,000). His institution received grants rated ($1,000–$5,000), Novartis Corp (less than $1,000). His institution from for-profit companies including Advanced Lifeline System ($150,000), receives grant support for patients enrolled in clinical studies from Eisai Cor- Siemens ($50,000), Bayer ($10,000), Byk Gulden ($15,000), AstraZen- poration (PI. Patients enrolled in the ACCESS study $50,000–$100,000), eca ($10,000), Faron Pharmaceuticals ($5,000), and Cerus Corporation Takeda (PI. Study terminated before patients enrolled). He received grants ($11,000). He received honoraria, consulting fees, editorship, royalties, and paid to his institution and consulting income from Artisan Pharma/Asahi Data and Safety Monitoring Board membership fees paid to him from Bayer Kasei Pharma America Corp ($25,000–$50,000). He consulted for Eli ($500), DHD ($1,000), Eli Lilly ($5,000), Oxford University Press ($10,000), Lilly (Sabbatical Consulting fee $10,000–$25,000) and received honoraria Hospira ($15,000), Cerner ($5,000), Pfizer ($1,000), KCI ($7,500), Ameri- from Eli Lilly (lecture $1,000–$5,000). He is a member of the Australia and can Association for Respiratory Care ($10,000), American Thoracic Society New Zealand Intensive Care Society Clinical Trials Group for the NICE- ($7,500), BioMed Central ($1,000), National Institutes of Health ($1,500), SUGAR Study (no money received); he is a council member of the Inter- and the Alberta Heritage Foundation for Medical Research ($250). He has national Sepsis Forum (as of Oct. 2010); he has held long time research database access or other intellectual (non financial) support from Cerner. interests in steroids in sepsis, PI of Corticus study, end-of-life decision mak- Dr. Webb consulted for AstraZeneca (anti-infectives $1,000−$5,000) and ing and PI of Ethicus, Ethicatt, and Welpicus studies. Jansen-Cilag (anti-infectives $1,000-$5,000). He received grant support 582 www.ccmjournal.org February 2013 • Volume 41 • Number 2
- 4. Special Article from a NHMRC project grant (ARISE RECT of EGDT); NHMRC proj- Eli Lilly and Company (development of educational presentations including ect grant and Fresinius-unrestricted grant (CHEST RCT of voluven vs. service on speaker’ bureaus (intensive care school hosted in department); saline); RCT of steroid vs. placebo for septic shock); NHMRC project travel/accommodations were reimbursed from bioMerieux (GeneXpert Focus grant (BLISS study of bacteria detection by PRC in septic shock) Intensive Group, France) and LiDCO (Winter Anaesthetic and Critical Care Review Care Foundation-ANZ (BLING pilot RCT of beta-lactam administration Conference), Surviving Sepsis Campaign (Publications Meeting, New York; by infusion); Hospira (SPICE programme of sedation delirium research); Care Bundles Conference, Manchester), SSC Publication Committee Meet- NHMRC Centres for Research Excellent Grant (critical illness microbi- ing and SSC Executive Committee Meeting, Nashville; SSC Meeting, Man- ology observational studies); Hospira-unrestricted grant (DAHlia RCT of chester), Novartis (Advisory Board Meeting, Zurich), Institute of Biomedical dexmedetomidine for agitated delirium). Travel/accommodations reim- Engineering (Hospital of the Future Grand Challenge Kick-Off Meeting, bursed by Jansen-Cilag ($5,000–$10,000) and AstraZeneca ($1,000- Hospital of the Future Grand Challenge Interviews EPSRC Headquarters, $5,000); he has a patent for a meningococcal vaccine. He is chair of the Swindon, Philips (Kick-Off Meeting, Boeblingen, Germany; MET Conference, ANZICS Clinical Trials Group and is an investigator in trials of EGDT, PCR Cohenhagen), Covidien (Adult Monitoring Advisory Board Meeting, Frank- for determining bacterial load and a steroid in the septic shock trial. furt), Eisai (ACCESS Investigators Meeting, Barcelona). His nonfinancial dis- closures include authorship of the position statement on fluid resuscitation Dr. Beale received compensation for his participation as board member for from the ESICM task force on colloids (yet to be finalized). Eisai, Inc, Applied Physiology, bioMérieux, Covidien, SIRS-Lab, and Novartis; consulting income was paid to his institution from PriceSpective Ltd, Easton Dr. Vincent reports consulting income paid to his institution from Astellas, Associates (soluble guanylate cyclase activator in acute respiratory distress AstraZeneca, Curacyte, Eli Lilly, Eisai, Ferring, GlaxoSmithKline, Merck, and syndrome/acute lung injury adjunct therapy to supportive care and ventila- Pfizer. His institution received honoraria on his behalf from Astellas, Astra- tion strategies), Eisai (eritoran), and Phillips (Respironics); he provided expert Zeneca, Curacyte, Eli Lilly, Eisai, Ferring, Merck, and Pfizer. His institution testimony for Eli Lilly and Company (paid to his institution); honoraria received received grant support from Astellas, Curacyte, Eli Lilly, Eisai, Ferring, and (paid to his institution) from Applied Physiology (Applied Physiology PL SAB, Pfizer. His institution received payment for educational presentations from Applied Physiology SAB, Brussels, Satellite Symposium at the ISICEM, Astellas, AstraZeneca, Curacyte, Eli Lilly, Eisai, Ferring, Merck, and Pfizer. Brussels), bioMérieux (GeneXpert Focus Group, France), SIRS-Lab (SIRS- Dr. Moreno consulted for bioMerieux (expert meeting). He is a coauthor of LAB SAB Forum, Brussels and SIRS-LAB SAB, Lisbon), Eli Lilly (CHMP a paper on corticosteroids in patients with septic shock. He is the author Hearing), Eisai (eritoran through leader touch plan in Brussels), Eli Lilly of several manuscripts defining sepsis and stratification of the patient with (Lunchtime Symposium, Vienna), Covidien (adult monitoring advisory board sepsis. He is also the author of several manuscripts contesting the utility meeting, Frankfurt), Covidien (Global Advisory Board CNIBP Boulder USA), of sepsis bundles. S METHODOLOGY epsis is a systemic, deleterious host response to infection leading to severe sepsis (acute organ dysfunction second- ary to documented or suspected infection) and septic Definitions shock (severe sepsis plus hypotension not reversed with fluid Sepsis is defined as the presence (probable or documented) of resuscitation). Severe sepsis and septic shock are major health- infection together with systemic manifestations of infection. care problems, affecting millions of people around the world Severe sepsis is defined as sepsis plus sepsis-induced organ each year, killing one in four (and often more), and increasing dysfunction or tissue hypoperfusion (Tables 1 and 2) (6). in incidence (1–5). Similar to polytrauma, acute myocardial Throughout this manuscript and the performance improve- infarction, or stroke, the speed and appropriateness of therapy ment bundles, which are included, a distinction is made administered in the initial hours after severe sepsis develops between definitions and therapeutic targets or thresholds. Sep- are likely to influence outcome. sis-induced hypotension is defined as a systolic blood pressure The recommendations in this document are intended to (SBP) 90 mm Hg or mean arterial pressure (MAP) 70 mm provide guidance for the clinician caring for a patient with Hg or a SBP decrease 40 mm Hg or less than two standard severe sepsis or septic shock. Recommendations from these deviations below normal for age in the absence of other causes guidelines cannot replace the clinician’s decision-making capa- of hypotension. An example of a therapeutic target or typical bility when he or she is presented with a patient’s unique set of threshold for the reversal of hypotension is seen in the sepsis clinical variables. Most of these recommendations are appro- bundles for the use of vasopressors. In the bundles, the MAP priate for the severe sepsis patient in the ICU and non-ICU set- threshold is ≥ 65 mm Hg. The use of definition vs. threshold will tings. In fact, the committee believes that the greatest outcome be evident throughout this article. Septic shock is defined as improvement can be made through education and process sepsis-induced hypotension persisting despite adequate fluid change for those caring for severe sepsis patients in the non- resuscitation. Sepsis-induced tissue hypoperfusion is defined ICU setting and across the spectrum of acute care. Resource as infection-induced hypotension, elevated lactate, or oliguria. limitations in some institutions and countries may prevent physicians from accomplishing particular recommendations. History of the Guidelines Thus, these recommendations are intended to be best practice These clinical practice guidelines are a revision of the 2008 (the committee considers this a goal for clinical practice) and SSC guidelines for the management of severe sepsis and septic not created to represent standard of care. The Surviving Sepsis shock (7). The initial SSC guidelines were published in 2004 Campaign (SSC) Guidelines Committee hopes that over time, (8) and incorporated the evidence available through the end particularly through education programs and formal audit of 2003. The 2008 publication analyzed evidence available and feedback performance improvement initiatives, the guide- through the end of 2007. The most current iteration is based lines will influence bedside healthcare practitioner behavior on updated literature search incorporated into the evolving that will reduce the burden of sepsis worldwide. manuscript through fall 2012. Critical Care Medicine www.ccmjournal.org 583
- 5. Dellinger et al Selection and Organization of Committee Members Grading of Recommendations The selection of committee members was based on inter- We advised the authors to follow the principles of the Grading est and expertise in specific aspects of sepsis. Co-chairs and of Recommendations Assessment, Development and Evalua- executive committee members were appointed by the Society tion (GRADE) system to guide assessment of quality of evi- of Critical Care Medicine and European Society of Intensive dence from high (A) to very low (D) and to determine the Care Medicine governing bodies. Each sponsoring organiza- strength of recommendations (Tables 3 and 4). (9–11). The tion appointed a representative who had sepsis expertise. Addi- SSC Steering Committee and individual authors collaborated tional committee members were appointed by the co-chairs with GRADE representatives to apply the system during the and executive committee to create continuity with the previous SSC guidelines revision process. The members of the GRADE committees’ membership as well as to address content needs group were directly involved, either in person or via e-mail, in for the development process. Four clinicians with experience all discussions and deliberations among the guidelines com- in the GRADE process application (referred to in this docu- mittee members as to grading decisions. ment as GRADE group or Evidence-Based Medicine [EBM] The GRADE system is based on a sequential assessment of group) took part in the guidelines development. the quality of evidence, followed by assessment of the balance The guidelines development process began with appoint- between the benefits and risks, burden, and cost, leading to ment of group heads and assignment of committee members development and grading of a management recommendation. to groups according to their specific expertise. Each group was Keeping the rating of quality of evidence and strength of responsible for drafting the initial update to the 2008 edition recommendation explicitly separate constitutes a crucial and in their assigned area (with major additional elements of infor- defining feature of the GRADE approach. This system classifies mation incorporated into the evolving manuscript through quality of evidence as high (grade A), moderate (grade B), low year-end 2011 and early 2012). (grade C), or very low (grade D). Randomized trials begin With input from the EBM group, an initial group meet- as high-quality evidence but may be downgraded due to ing was held to establish procedures for literature review and limitations in implementation, inconsistency, or imprecision of development of tables for evidence analysis. Committees and the results, indirectness of the evidence, and possible reporting their subgroups continued work via phone and the Internet. bias (Table 3). Examples of indirectness of the evidence Several subsequent meetings of subgroups and key indi- include population studied, interventions used, outcomes viduals occurred at major international meetings (nominal measured, and how these relate to the question of interest. groups), with work continuing via teleconferences and elec- Well-done observational (nonrandomized) studies begin as tronic-based discussions among subgroups and members low-quality evidence, but the quality level may be upgraded on of the entire committee. Ultimately, a meeting of all group the basis of a large magnitude of effect. An example of this is heads, executive committee members, and other key commit- the quality of evidence for early administration of antibiotics. tee members was held to finalize the draft document for sub- References to supplemental digital content appendices of mission to reviewers. GRADEpro Summary of Evidence Tables appear throughout this document. Search Techniques The GRADE system classifies recommendations as strong A separate literature search was performed for each clearly (grade 1) or weak (grade 2). The factors influencing this deter- defined question. The committee chairs worked with subgroup mination are presented in Table 4. The assignment of strong heads to identify pertinent search terms that were to include, or weak is considered of greater clinical importance than a at a minimum, sepsis, severe sepsis, septic shock, and sepsis syn- difference in letter level of quality of evidence. The commit- drome crossed against the subgroup’s general topic area, as well tee assessed whether the desirable effects of adherence would as appropriate key words of the specific question posed. All outweigh the undesirable effects, and the strength of a rec- questions used in the previous guidelines publications were ommendation reflects the group’s degree of confidence in searched, as were pertinent new questions generated by gen- that assessment. Thus, a strong recommendation in favor of eral topic-related searches or recent trials. The authors were an intervention reflects the panel’s opinion that the desirable specifically asked to look for existing meta-analyses related to effects of adherence to a recommendation (beneficial health their question and search a minimum of one general database outcomes; lesser burden on staff and patients; and cost sav- (ie, MEDLINE, EMBASE) and the Cochrane Library (both ings) will clearly outweigh the undesirable effects (harm to The Cochrane Database of Systematic Reviews [CDSR] and health; more burden on staff and patients; and greater costs). Database of Abstracts of Reviews of Effectiveness [DARE]). The potential drawbacks of making strong recommenda- Other databases were optional (ACP Journal Club, Evidence- tions in the presence of low-quality evidence were taken into Based Medicine Journal, Cochrane Registry of Controlled account. A weak recommendation in favor of an intervention Clinical Trials, International Standard Randomized Controlled indicates the judgment that the desirable effects of adherence Trial Registry [http://www.controlled-trials.com/isrctn/] or to a recommendation probably will outweigh the undesirable metaRegister of Controlled Trials [http://www.controlled- effects, but the panel is not confident about these tradeoffs— trials.com/mrct/]. Where appropriate, available evidence was either because some of the evidence is low quality (and thus summarized in the form of evidence tables. uncertainty remains regarding the benefits and risks) or the 584 www.ccmjournal.org February 2013 • Volume 41 • Number 2
- 6. Special Article Table 1. Diagnostic Criteria for Sepsis Infection, documented or suspected, and some of the following: General variables Fever ( 38.3°C) Hypothermia (core temperature 36°C) Heart rate 90/min–1 or more than two sd above the normal value for age Tachypnea Altered mental status Significant edema or positive fluid balance ( 20 mL/kg over 24 hr) Hyperglycemia (plasma glucose 140 mg/dL or 7.7 mmol/L) in the absence of diabetes Inflammatory variables Leukocytosis (WBC count 12,000 µL–1) Leukopenia (WBC count 4000 µL–1) Normal WBC count with greater than 10% immature forms Plasma C-reactive protein more than two sd above the normal value Plasma procalcitonin more than two sd above the normal value Hemodynamic variables Arterial hypotension (SBP 90 mm Hg, MAP 70 mm Hg, or an SBP decrease 40 mm Hg in adults or less than two sd below normal for age) Organ dysfunction variables Arterial hypoxemia (Pao2/Fio2 300) Acute oliguria (urine output 0.5 mL/kg/hr for at least 2 hrs despite adequate fluid resuscitation) Creatinine increase 0.5 mg/dL or 44.2 µmol/L Coagulation abnormalities (INR 1.5 or aPTT 60 s) Ileus (absent bowel sounds) Thrombocytopenia (platelet count 100,000 µL–1) Hyperbilirubinemia (plasma total bilirubin 4 mg/dL or 70 µmol/L) Tissue perfusion variables Hyperlactatemia ( 1 mmol/L) Decreased capillary refill or mottling WBC = white blood cell; SBP = systolic blood pressure; MAP = mean arterial pressure; INR = international normalized ratio; aPTT = activated partial thromboplastin time. Diagnostic criteria for sepsis in the pediatric population are signs and symptoms of inflammation plus infection with hyper- or hypothermia (rectal temperature 38.5° or 35°C), tachycardia (may be absent in hypothermic patients), and at least one of the following indications of altered organ function: altered mental status, hypoxemia, increased serum lactate level, or bounding pulses. Adapted from Levy MM, Fink MP, Marshall JC, et al: 2001 SCCM/ESICM/ACCP/ATS/SIS International Sepsis Definitions Conference. Crit Care Med 2003; 31: 1250–1256. benefits and downsides are closely balanced. A strong recom- The implications of calling a recommendation strong mendation is worded as “we recommend” and a weak recom- are that most well-informed patients would accept that mendation as “we suggest.” intervention and that most clinicians should use it in most Throughout the document are a number of statements situations. Circumstances may exist in which a strong rec- that either follow graded recommendations or are listed as ommendation cannot or should not be followed for an stand-alone numbered statements followed by “ungraded” individual because of that patient’s preferences or clinical in parentheses (UG). In the opinion of the committee, characteristics that make the recommendation less applica- these recommendations were not conducive for the GRADE ble. A strong recommendation does not automatically imply process. standard of care. For example, the strong recommendation Critical Care Medicine www.ccmjournal.org 585
- 7. Dellinger et al Table 2. Severe Sepsis Severe sepsis definition = sepsis-induced tissue hypoperfusion or organ dysfunction (any of the following thought to be due to the infection) Sepsis-induced hypotension Lactate above upper limits laboratory normal Urine output 0.5 mL/kg/hr for more than 2 hrs despite adequate fluid resuscitation Acute lung injury with Pao2/Fio2 250 in the absence of pneumonia as infection source Acute lung injury with Pao2/Fio2 200 in the presence of pneumonia as infection source Creatinine 2.0 mg/dL (176.8 µmol/L) Bilirubin 2 mg/dL (34.2 µmol/L) Platelet count 100,000 µL Coagulopathy (international normalized ratio 1.5) Adapted from Levy MM, Fink MP, Marshall JC, et al: 2001 SCCM/ESICM/ACCP/ATS/SIS International Sepsis Definitions Conference. Crit Care Med 2003; 31: 1250–1256. for administering antibiotics within 1 hr of the diagnosis were available for advice throughout the process. Subgroups of severe sepsis, as well as the recommendation for achiev- agreed electronically on draft proposals that were then ing a central venous pressure (CVP) of 8 mm Hg and a cen- presented for general discussion among subgroup heads, the tral venous oxygen saturation (Scvo2) of 70% in the first 6 SSC Steering Committee (two co-chairs, two co-vice chairs, hrs of resuscitation of sepsis-induced tissue hypoperfusion, and an at-large committee member), and several selected key although deemed desirable, are not yet standards of care as committee members who met in July 2011 in Chicago. The verified by practice data. results of that discussion were incorporated into the next Significant education of committee members on the version of recommendations and again discussed with the GRADE approach built on the process conducted during 2008 whole group using electronic mail. Draft recommendations efforts. Several members of the committee were trained in were distributed to the entire committee and finalized during the use of GRADEpro software, allowing more formal use of an additional nominal group meeting in Berlin in October the GRADE system (12). Rules were distributed concerning 2011. Deliberations and decisions were then recirculated to the assessing the body of evidence, and GRADE representatives entire committee for approval. At the discretion of the chairs Table 3. Determination of the Quality of Evidence Underlying methodology A (high) RCTs B (moderate) Downgraded RCTs or upgraded observational studies C (low) Well-done observational studies with control RCTs D (very low) Downgraded controlled studies or expert opinion based on other evidence Factors that may decrease the strength of evidence 1. Poor quality of planning and implementation of available RCTs, suggesting high likelihood of bias 2. Inconsistency of results, including problems with subgroup analyses 3. Indirectness of evidence (differing population, intervention, control, outcomes, comparison) 4. Imprecision of results 5. High likelihood of reporting bias Main factors that may increase the strength of evidence 1. Large magnitude of effect (direct evidence, relative risk 2 with no plausible confounders) 2. Very large magnitude of effect with relative risk 5 and no threats to validity (by two levels) 3. Dose-response gradient RCT = randomized controlled trial. 586 www.ccmjournal.org February 2013 • Volume 41 • Number 2
- 8. Special Article Table 4. Factors Determining Strong vs. Weak Recommendation What Should be Considered Recommended Process High or moderate evidence The higher the quality of evidence, the more likely a strong recommendation. (Is there high or moderate quality evidence?) Certainty about the balance of benefits vs. The larger the difference between the desirable and undesirable consequences and harms and burdens (Is there certainty?) the certainty around that difference, the more likely a strong recommendation. The smaller the net benefit and the lower the certainty for that benefit, the more likely a weak recommendation. Certainty in or similar values The more certainty or similarity in values and preferences, the more likely a strong (Is there certainty or similarity?) recommendation. Resource implications The lower the cost of an intervention compared to the alternative and other costs related to (Are resources worth expected benefits?) the decision–ie, fewer resources consumed–the more likely a strong recommendation. and following discussion, competing proposals for wording they had the least COI. They were required to work within of recommendations or assigning strength of evidence were their group with full disclosure when a topic for which they resolved by formal voting within subgroups and at nominal had relevant COI was discussed, and they were not allowed group meetings. The manuscript was edited for style and form to serve as group head. At the time of final approval of the by the writing committee with final approval by subgroup document, an update of the COI statement was required. No heads and then by the entire committee. To satisfy peer review additional COI issues were reported that required further during the final stages of manuscript approval for publication, adjudication. several recommendations were edited with approval of the SSC executive committee group head for that recommendation and MANAGEMENT OF SEVERE SEPSIS the EBM lead. Initial Resuscitation and Infection Issues (Table 5) Conflict of Interest Policy A. Initial Resuscitation Since the inception of the SSC guidelines in 2004, no members 1. We recommend the protocolized, quantitative resuscitation of of the committee represented industry; there was no industry patients with sepsis- induced tissue hypoperfusion (defined in input into guidelines development; and no industry represen- this document as hypotension persisting after initial fluid chal- tatives were present at any of the meetings. Industry awareness lenge or blood lactate concentration ≥ 4 mmol/L). This proto- or comment on the recommendations was not allowed. No col should be initiated as soon as hypoperfusion is recognized member of the guidelines committee received honoraria for and should not be delayed pending ICU admission. During the any role in the 2004, 2008, or 2012 guidelines process. first 6 hrs of resuscitation, the goals of initial resuscitation of A detailed description of the disclosure process and all sepsis-induced hypoperfusion should include all of the follow- author disclosures appear in Supplemental Digital Content 1 ing as a part of a treatment protocol (grade 1C): in the supplemental materials to this document. Appendix B a) CVP 8–12 mm Hg shows a flowchart of the COI disclosure process. Committee b) MAP ≥ 65 mm Hg members who were judged to have either financial or nonfi- c) Urine output ≥ 0.5 mL·kg·hr nancial/academic competing interests were recused during the d) uperior vena cava oxygenation saturation (Scvo2) or S closed discussion session and voting session on that topic. Full mixed venous oxygen saturation (Svo2) 70% or 65%, disclosure and transparency of all committee members’ poten- respectively. tial conflicts were sought. 2. We suggest targeting resuscitation to normalize lactate in On initial review, 68 financial conflict of interest (COI) patients with elevated lactate levels as a marker of tissue disclosures and 54 nonfinancial disclosures were submitted hypoperfusion (grade 2C). by committee members. Declared COI disclosures from 19 members were determined by the COI subcommittee to be Rationale. In a randomized, controlled, single-center study, not relevant to the guidelines content process. Nine who early quantitative resuscitation improved survival for emer- were determined to have COI (financial and nonfinancial) gency department patients presenting with septic shock (13). were adjudicated by group reassignment and requirement Resuscitation targeting the physiologic goals expressed in rec- to adhere to SSC COI policy regarding discussion or voting ommendation 1 (above) for the initial 6-hr period was associ- at any committee meetings where content germane to their ated with a 15.9% absolute reduction in 28-day mortality rate. COI was discussed. Nine were judged as having conflicts This strategy, termed early goal-directed therapy, was evalu- that could not be resolved solely by reassignment. One of ated in a multicenter trial of 314 patients with severe sepsis in these individuals was asked to step down from the commit- eight Chinese centers (14). This trial reported a 17.7% absolute tee. The other eight were assigned to the groups in which reduction in 28-day mortality (survival rates, 75.2% vs. 57.5%, Critical Care Medicine www.ccmjournal.org 587
- 9. Dellinger et al p = 0.001). A large number of other observational studies using generally can be relied upon as supporting positive response to similar forms of early quantitative resuscitation in comparable fluid loading. Either intermittent or continuous measurements patient populations have shown significant mortality reduction of oxygen saturation were judged to be acceptable. During compared to the institutions’ historical controls (Supplemental the first 6 hrs of resuscitation, if Scvo2 less than 70% or Svo2 Digital Content 2, http://links.lww.com/CCM/A615). Phase III equivalent of less than 65% persists with what is judged to be of the SSC activities, the international performance improve- adequate intravascular volume repletion in the presence of ment program, showed that the mortality of septic patients persisting tissue hypoperfusion, then dobutamine infusion (to a presenting with both hypotension and lactate ≥ 4 mmol/L was maximum of 20 μg/kg/min) or transfusion of packed red blood 46.1%, similar to the 46.6% mortality found in the first trial cited cells to achieve a hematocrit of greater than or equal to 30% in above (15). As part of performance improvement programs, attempts to achieve the Scvo2 or Svo2 goal are options. The strong some hospitals have lowered the lactate threshold for triggering recommendation for achieving a CVP of 8 mm Hg and an Scvo2 quantitative resuscitation in the patient with severe sepsis, but of 70% in the first 6 hrs of resuscitation of sepsis-induced tissue these thresholds have not been subjected to randomized trials. hypoperfusion, although deemed desirable, are not yet the The consensus panel judged use of CVP and Svo2 targets standard of care as verified by practice data. The publication to be recommended physiologic targets for resuscitation. of the initial results of the international SSC performance Although there are limitations to CVP as a marker of improvement program demonstrated that adherence to CVP intravascular volume status and response to fluids, a low CVP and Scvo2 targets for initial resuscitation was low (15). Table 5. Recommendations: Initial Resuscitation and Infection Issues A. Initial Resuscitation 1. rotocolized, quantitative resuscitation of patients with sepsis- induced tissue hypoperfusion (defined in this document as hypotension P persisting after initial fluid challenge or blood lactate concentration ≥ 4 mmol/L). Goals during the first 6 hrs of resuscitation: a) Central venous pressure 8–12 mm Hg b) Mean arterial pressure (MAP) ≥ 65 mm Hg c) Urine output ≥ 0.5 mL/kg/hr d) Central venous (superior vena cava) or mixed venous oxygen saturation 70% or 65%, respectively (grade 1C). 2. In patients with elevated lactate levels targeting resuscitation to normalize lactate (grade 2C). B. Screening for Sepsis and Performance Improvement 1. outine screening of potentially infected seriously ill patients for severe sepsis to allow earlier implementation of therapy (grade 1C). R 2. Hospital–based performance improvement efforts in severe sepsis (UG). C. Diagnosis 1. ultures as clinically appropriate before antimicrobial therapy if no significant delay ( 45 mins) in the start of antimicrobial(s) (grade C 1C). At least 2 sets of blood cultures (both aerobic and anaerobic bottles) be obtained before antimicrobial therapy with at least 1 drawn percutaneously and 1 drawn through each vascular access device, unless the device was recently (48 hrs) inserted (grade 1C). 2. se of the 1,3 beta-D-glucan assay (grade 2B), mannan and anti-mannan antibody assays (2C), if available and invasive U candidiasis is in differential diagnosis of cause of infection. 3. Imaging studies performed promptly to confirm a potential source of infection (UG). D. Antimicrobial Therapy 1. dministration of effective intravenous antimicrobials within the first hour of recognition of septic shock (grade 1B) and severe A sepsis without septic shock (grade 1C) as the goal of therapy. 2a. nitial empiric anti-infective therapy of one or more drugs that have activity against all likely pathogens (bacterial and/or fungal or I viral) and that penetrate in adequate concentrations into tissues presumed to be the source of sepsis (grade 1B). 2b. Antimicrobial regimen should be reassessed daily for potential deescalation (grade 1B). 3. se of low procalcitonin levels or similar biomarkers to assist the clinician in the discontinuation of empiric antibiotics in patients U who initially appeared septic, but have no subsequent evidence of infection (grade 2C). 4a. Combination empirical therapy for neutropenic patients with severe sepsis (grade 2B) and for patients with difficult-to-treat, multidrug- resistant bacterial pathogens such as Acinetobacter and Pseudomonas spp. (grade 2B). For patients with severe infections associated with respiratory failure and septic shock, combination therapy with an extended spectrum beta-lactam and either an aminoglycoside or a fluoroquinolone is for P. aeruginosa bacteremia (grade 2B). A combination of beta-lactam and macrolide for patients with septic shock from bacteremic Streptococcus pneumoniae infections (grade 2B). (Continued) 588 www.ccmjournal.org February 2013 • Volume 41 • Number 2
- 10. Special Article Table 5. (Continued) Recommendations: Initial Resuscitation and Infection Issues 4b. mpiric combination therapy should not be administered for more than 3–5 days. De-escalation to the most appropriate single E therapy should be performed as soon as the susceptibility profile is known (grade 2B). 5. Duration of therapy typically 7–10 days; longer courses may be appropriate in patients who have a slow clinical response, undrainable foci of infection, bacteremia with S. aureus; some fungal and viral infections or immunologic deficiencies, including neutropenia (grade 2C). 6. Antiviral therapy initiated as early as possible in patients with severe sepsis or septic shock of viral origin (grade 2C). 7. Antimicrobial agents should not be used in patients with severe inflammatory states determined to be of noninfectious cause (UG). E. Source Control 1. A specific anatomical diagnosis of infection requiring consideration for emergent source control be sought and diagnosed or excluded as rapidly as possible, and intervention be undertaken for source control within the first 12 hr after the diagnosis is made, if feasible (grade 1C). 2. When infected peripancreatic necrosis is identified as a potential source of infection, definitive intervention is best delayed until adequate demarcation of viable and nonviable tissues has occurred (grade 2B). 3. When source control in a severely septic patient is required, the effective intervention associated with the least physiologic insult should be used (eg, percutaneous rather than surgical drainage of an abscess) (UG). 4. f intravascular access devices are a possible source of severe sepsis or septic shock, they should be removed promptly after I other vascular access has been established (UG). F. Infection Prevention 1a. elective oral decontamination and selective digestive decontamination should be introduced and investigated as a method to S reduce the incidence of ventilator-associated pneumonia; This infection control measure can then be instituted in health care settings and regions where this methodology is found to be effective (grade 2B). 1b. ral chlorhexidine gluconate be used as a form of oropharyngeal decontamination to reduce the risk of ventilator-associated O pneumonia in ICU patients with severe sepsis (grade 2B). In mechanically ventilated patients or those with known fluid responsiveness during resuscitation, including flow and preexisting decreased ventricular compliance, a higher target possibly volumetric indices and microcirculatory changes, CVP of 12 to 15 mm Hg should be achieved to account for may have advantages (29–32). Available technologies allow the impediment in filling (16). Similar consideration may be measurement of flow at the bedside (33, 34); however, the effi- warranted in circumstances of increased abdominal pressure cacy of these monitoring techniques to influence clinical out- (17). Elevated CVP may also be seen with preexisting clini- comes from early sepsis resuscitation remains incomplete and cally significant pulmonary artery hypertension, making use requires further study before endorsement. of this variable untenable for judging intravascular volume The global prevalence of severe sepsis patients initially pre- status. Although the cause of tachycardia in septic patients senting with either hypotension with lactate ≥ 4 mmol//L, hypo- may be multifactorial, a decrease in elevated pulse rate with tension alone, or lactate ≥ 4 mmol/L alone, is reported as 16.6%, fluid resuscitation is often a useful marker of improving intra- 49.5%, and 5.4%, respectively (15). The mortality rate is high in vascular filling. Published observational studies have dem- septic patients with both hypotension and lactate ≥ 4 mmol/L onstrated an association between good clinical outcome in (46.1%) (15), and is also increased in severely septic patients septic shock and MAP ≥ 65 mm Hg as well as Scvo2 ≥ 70% with hypotension alone (36.7%) and lactate ≥ 4 mmol/L alone (measured in the superior vena cava, either intermittently or (30%) (15). If Scvo2 is not available, lactate normalization may continuously [18]). Many studies support the value of early be a feasible option in the patient with severe sepsis-induced protocolized resuscitation in severe sepsis and sepsis-induced tissue hypoperfusion. Scvo2 and lactate normalization may also tissue hypoperfusion (19–24). Studies of patients with shock be used as a combined endpoint when both are available. Two indicate that Svo2 runs 5% to 7% lower than Scvo2 (25). While multicenter randomized trials evaluated a resuscitation strat- the committee recognized the controversy surrounding egy that included lactate reduction as a single target or a tar- resuscitation targets, an early quantitative resuscitation pro- get combined with Scvo2 normalization (35, 36). The first trial tocol using CVP and venous blood gases can be readily estab- reported that early quantitative resuscitation based on lactate lished in both emergency department and ICU settings (26). clearance (decrease by at least 10%) was noninferior to early Recognized limitations to static ventricular filling pressure quantitative resuscitation based on achieving Scvo2 of 70% or estimates exist as surrogates for fluid resuscitation (27, 28), but more (35). The intention-to-treat group contained 300, but the measurement of CVP is currently the most readily obtainable number of patients actually requiring either Scvo2 normalization target for fluid resuscitation. Targeting dynamic measures of or lactate clearance was small (n = 30). The second trial included Critical Care Medicine www.ccmjournal.org 589
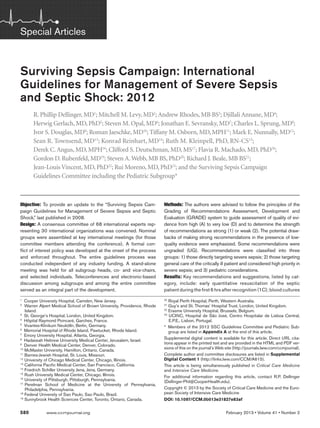
- 11. Dellinger et al 348 patients with lactate levels ≥ 3 mmol/L (36). The strategy in 32,000 patient charts gathered from 239 hospitals in 17 countries this trial was based on a greater than or equal to 20% decrease through September 2011 as part of phase III of the campaign in lactate levels per 2 hrs of the first 8 hrs in addition to Scvo2 informed the revision of the bundles in conjunction with the target achievement, and was associated with a 9.6% absolute 2012 guidelines. As a result, for the 2012 version, the management reduction in mortality (p = 0.067; adjusted hazard ratio, 0.61; bundle was dropped and the resuscitation bundle was broken into 95% CI, 0.43−0.87; p = 0.006). two parts and modified as shown in Figure 1. For performance B. Screening for Sepsis and Performance improvement quality indicators, resuscitation target thresholds Improvement are not considered. However, recommended targets from the guidelines are included with the bundles for reference purposes. 1. We recommend routine screening of potentially infected seriously ill patients for severe sepsis to increase the early C. Diagnosis identification of sepsis and allow implementation of early 1. We recommend obtaining appropriate cultures before anti- sepsis therapy (grade 1C). microbial therapy is initiated if such cultures do not cause sig- Rationale. The early identification of sepsis and imple- nificant delay ( 45 minutes) in the start of antimicrobial(s) mentation of early evidence-based therapies have been doc- administration (grade 1C). To optimize identification of caus- umented to improve outcomes and decrease sepsis-related ative organisms, we recommend obtaining at least two sets of mortality (15). Reducing the time to diagnosis of severe sepsis blood cultures (both aerobic and anaerobic bottles) before is thought to be a critical component of reducing mortality antimicrobial therapy, with at least one drawn percutaneously from sepsis-related multiple organ dysfunction (35). Lack of and one drawn through each vascular access device, unless early recognition is a major obstacle to sepsis bundle initiation. the device was recently ( 48 hours) inserted. These blood Sepsis screening tools have been developed to monitor ICU cultures can be drawn at the same time if they are obtained patients (37–41), and their implementation has been associ- from different sites. Cultures of other sites (preferably quan- ated with decreased sepsis-related mortality (15). titative where appropriate), such as urine, cerebrospinal fluid, wounds, respiratory secretions, or other body fluids that may 2. Performance improvement efforts in severe sepsis should be be the source of infection, should also be obtained before used to improve patient outcomes (UG). antimicrobial therapy if doing so does not cause significant Rationale. Performance improvement efforts in sepsis have delay in antibiotic administration (grade 1C). been associated with improved patient outcomes (19, 42–46). Improvement in care through increasing compliance with sep- Rationale. Although sampling should not delay timely sis quality indicators is the goal of a severe sepsis performance administration of antimicrobial agents in patients with severe improvement program (47). Sepsis management requires a mul- sepsis (eg, lumbar puncture in suspected meningitis), obtain- tidisciplinary team (physicians, nurses, pharmacy, respiratory, ing appropriate cultures before administration of antimicrobials dieticians, and administration) and multispecialty collaboration is essential to confirm infection and the responsible pathogens, (medicine, surgery, and emergency medicine) to maximize the and to allow de-escalation of antimicrobial therapy after receipt chance for success. Evaluation of process change requires consis- of the susceptibility profile. Samples can be refrigerated or fro- tent education, protocol development and implementation, data zen if processing cannot be performed immediately. Because collection, measurement of indicators, and feedback to facilitate rapid sterilization of blood cultures can occur within a few the continuous performance improvement. Ongoing educational hours after the first antimicrobial dose, obtaining those cultures sessions provide feedback on indicator compliance and can help before therapy is essential if the causative organism is to be iden- identify areas for additional improvement efforts. In addition to tified. Two or more blood cultures are recommended (51). In traditional continuing medical education efforts to introduce patients with indwelling catheters (for more than 48 hrs), at least guidelines into clinical practice, knowledge translation efforts one blood culture should be drawn through each lumen of each have recently been introduced as a means to promote the use of vascular access device (if feasible, especially for vascular devices high-quality evidence in changing behavior (48). Protocol imple- with signs of inflammation, catheter dysfunction, or indicators mentation associated with education and performance feedback of thrombus formation). Obtaining blood cultures peripherally has been shown to change clinician behavior and is associated and through a vascular access device is an important strategy. If with improved outcomes and cost-effectiveness in severe sepsis the same organism is recovered from both cultures, the likeli- (19, 23, 24, 49). In partnership with the Institute for Healthcare hood that the organism is causing the severe sepsis is enhanced. Improvement, phase III of the Surviving Sepsis Campaign targeted In addition, if equivalent volumes of blood drawn for cul- the implementation of a core set (“bundle”) of recommendations ture and the vascular access device is positive much earlier than in hospital environments where change in behavior and clinical the peripheral blood culture (ie, more than 2 hrs earlier), the impact were measured (50). The SSC guidelines and bundles can data support the concept that the vascular access device is the be used as the basis of a sepsis performance improvement program. source of the infection (36, 51, 52). Quantitative cultures of Application of the SSC sepsis bundles led to sustained, catheter and peripheral blood may also be useful for determin- continuous quality improvement in sepsis care and was associated ing whether the catheter is the source of infection. The volume with reduced mortality (15). Analysis of the data from nearly of blood drawn with the culture tube should be ≥ 10 mL (53). 590 www.ccmjournal.org February 2013 • Volume 41 • Number 2
- 12. Special Article Rationale. The diagnosis of SURVIVING SEPSIS CAMPAIGN BUNDLES systemic fungal infection (usu- TO BE COMPLETED WITHIN 3 HOURS: ally candidiasis) in the critically 1) Measure lactate level ill patient can be challenging, 2) Obtain blood cultures prior to administration of antibiotics 3) Administer broad spectrum antibiotics and rapid diagnostic methodolo- 4) Administer 30 mL/kg crystalloid for hypotension or lactate 4mmol/L gies, such as antigen and antibody detection assays, can be helpful in TO BE COMPLETED WITHIN 6 HOURS: 5) Apply vasopressors (for hypotension that does not respond to initial fluid resuscitation) detecting candidiasis in the ICU to maintain a mean arterial pressure (MAP) ≥ 65 mm Hg patient. These suggested tests have 6) In the event of persistent arterial hypotension despite volume resuscitation (septic shown positive results significantly shock) or initial lactate 4 mmol/L (36 mg/dL): - Measure central venous pressure (CVP)* earlier than standard culture meth- - Measure central venous oxygen saturation (ScvO2)* ods (62–67), but false-positive 7) Remeasure lactate if initial lactate was elevated* reactions can occur with coloni- *Targets for quantitative resuscitation included in the guidelines are CVP of ≥8 mm Hg, zation alone, and their diagnostic ScvO2 of 70%, and normalization of lactate. utility in managing fungal infec- tion in the ICU needs additional Figure 1. Surviving Sepsis Campaign Care Bundles. study (65). Quantitative (or semiquantitative) cultures of respiratory tract 3. We recommend that imaging studies be performed secretions are often recommended for the diagnosis of venti- promptly in attempts to confirm a potential source of infec- lator-associated pneumonia (54), but their diagnostic value tion. Potential sources of infection should be sampled as remains unclear (55). they are identified and in consideration of patient risk for The Gram stain can be useful, in particular for respiratory transport and invasive procedures (eg, careful coordination tract specimens, to determine if inflammatory cells are pres- and aggressive monitoring if the decision is made to trans- ent (greater than five polymorphonuclear leukocytes/high- port for a CT-guided needle aspiration). Bedside studies, powered field and less than ten squamous cells/low-powered such as ultrasound, may avoid patient transport (UG). field) and if culture results will be informative of lower respi- Rationale. Diagnostic studies may identify a source of ratory pathogens. Rapid influenza antigen testing during peri- infection that requires removal of a foreign body or drainage to ods of increased influenza activity in the community is also maximize the likelihood of a satisfactory response to therapy. recommended. A focused history can provide vital informa- Even in the most organized and well-staffed healthcare facili- tion about potential risk factors for infection and likely patho- ties, however, transport of patients can be dangerous, as can gens at specific tissue sites. The potential role of biomarkers be placing patients in outside-unit imaging devices that are for diagnosis of infection in patients presenting with severe difficult to access and monitor. Balancing risk and benefit is sepsis remains undefined. The utility of procalcitonin levels or therefore mandatory in those settings. other biomarkers (such as C-reactive protein) to discriminate the acute inflammatory pattern of sepsis from other causes of D. Antimicrobial Therapy generalized inflammation (eg, postoperative, other forms of 1. The administration of effective intravenous antimicrobials shock) has not been demonstrated. No recommendation can within the first hour of recognition of septic shock (grade be given for the use of these markers to distinguish between 1B) and severe sepsis without septic shock (grade 1C) severe infection and other acute inflammatory states (56–58). should be the goal of therapy. Remark: Although the weight In the near future, rapid, non-culture-based diagnostic meth- of the evidence supports prompt administration of antibi- ods (polymerase chain reaction, mass spectroscopy, microar- otics following the recognition of severe sepsis and septic rays) might be helpful for a quicker identification of pathogens shock, the feasibility with which clinicians may achieve this and major antimicrobial resistance determinants (59). These ideal state has not been scientifically evaluated. methodologies could be particularly useful for difficult-to-cul- ture pathogens or in clinical situations where empiric antimi- Rationale. Establishing vascular access and initiating crobial agents have been administered before culture samples aggressive fluid resuscitation are the first priorities when were been obtained. Clinical experience remains limited, and managing patients with severe sepsis or septic shock. Prompt more clinical studies are needed before recommending these infusion of antimicrobial agents should also be a priority and non-culture molecular methods as a replacement for standard may require additional vascular access ports (68, 69). In the presence of septic shock, each hour delay in achieving admin- blood culture methods (60, 61). istration of effective antibiotics is associated with a measurable 2. We suggest the use of the 1,3 β-d-glucan assay (grade 2B), increase in mortality in a number of studies (15, 68, 70–72). mannan and anti-mannan antibody assays (grade 2C) Overall, the preponderance of data support giving antibiot- when invasive candidiasis is in the differential diagnosis of ics as soon as possible in patients with severe sepsis with or infection. without septic shock (15, 68, 70–77). The administration of Critical Care Medicine www.ccmjournal.org 591
- 13. Dellinger et al antimicrobial agents with a spectrum of activity likely to treat of amphotericin B) should be tailored to the local pattern of the responsible pathogen(s) effectively within 1 hr of the diag- the most prevalent Candida species and any recent exposure nosis of severe sepsis and septic shock. Practical considerations, to antifungal drugs (78). Recent Infectious Diseases Society for example challenges with clinicians’ early identification of of America (IDSA) guidelines recommend either fluconazole patients or operational complexities in the drug delivery chain, or an echinocandin. Empiric use of an echinocandin is pre- represent unstudied variables that may impact achieving this ferred in most patients with severe illness, especially in those goal. Future trials should endeavor to provide an evidence base patients who have recently been treated with antifungal agents, in this regard. This should be the target goal when managing or if Candida glabrata infection is suspected from earlier cul- patients with septic shock, whether they are located within the ture data. Knowledge of local resistance patterns to antifungal hospital ward, the emergency department, or the ICU. The agents should guide drug selection until fungal susceptibility strong recommendation for administering antibiotics within 1 test results, if available, are performed. Risk factors for candi- hr of the diagnosis of severe sepsis and septic shock, although demia, such as immunosuppressed or neutropenic state, prior judged to be desirable, is not yet the standard of care as verified intense antibiotic therapy, or colonization in multiple sites, by published practice data (15). should also be considered when choosing initial therapy. If antimicrobial agents cannot be mixed and delivered promptly Because patients with severe sepsis or septic shock have little from the pharmacy, establishing a supply of premixed antibiotics margin for error in the choice of therapy, the initial selection for such urgent situations is an appropriate strategy for ensuring of antimicrobial therapy should be broad enough to cover all prompt administration. Many antibiotics will not remain stable if likely pathogens. Antibiotic choices should be guided by local premixed in a solution. This risk must be taken into consideration prevalence patterns of bacterial pathogens and susceptibility in institutions that rely on premixed solutions for rapid availabil- data. Ample evidence exists that failure to initiate appropriate ity of antibiotics. In choosing the antimicrobial regimen, clinicians therapy (ie, therapy with activity against the pathogen that is should be aware that some antimicrobial agents have the advan- subsequently identified as the causative agent) correlates with tage of bolus administration, while others require a lengthy infu- increased morbidity and mortality in patients with severe sep- sion. Thus, if vascular access is limited and many different agents sis or septic shock (68, 71, 79, 80). Recent exposure to anti- must be infused, bolus drugs may offer an advantage. microbials (within last 3 months) should be considered in the choice of an empiric antibacterial regimen. Patients with 2a. We recommend that initial empiric anti-infective therapy severe sepsis or septic shock warrant broad-spectrum therapy include one or more drugs that have activity against all until the causative organism and its antimicrobial susceptibili- likely pathogens (bacterial and/or fungal or viral) and that ties are defined. Although a global restriction of antibiotics is penetrate in adequate concentrations into the tissues pre- an important strategy to reduce the development of antimi- sumed to be the source of sepsis (grade 1B). crobial resistance and to reduce cost, it is not an appropri- Rationale. The choice of empirical antimicrobial therapy ate strategy in the initial therapy for this patient population. depends on complex issues related to the patient’s history, However, as soon as the causative pathogen has been identi- including drug intolerances, recent receipt of antibiotics (previ- fied, de-escalation should be performed by selecting the most ous 3 months), underlying disease, the clinical syndrome, and appropriate antimicrobial agent that covers the pathogen susceptibility patterns of pathogens in the community and hos- and is safe and cost-effective. Collaboration with antimicro- pital, and that previously have been documented to colonize bial stewardship programs, where they exist, is encouraged to or infect the patient. The most common pathogens that cause ensure appropriate choices and rapid availability of effective septic shock in hospitalized patients are Gram-positive bac- antimicrobials for treating septic patients. All patients should teria, followed by Gram-negative and mixed bacterial micro- receive a full loading dose of each agent. Patients with sepsis organisms. Candidiasis, toxic shock syndromes, and an array often have abnormal and vacillating renal or hepatic function, of uncommon pathogens should be considered in selected or may have abnormally high volumes of distribution due to patients. An especially wide range of potential pathogens exists aggressive fluid resuscitation, requiring dose adjustment. Drug for neutropenic patients. Recently used anti-nfective agents i serum concentration monitoring can be useful in an ICU set- should generally be avoided. When choosing empirical therapy, ting for those drugs that can be measured promptly. Significant clinicians should be cognizant of the virulence and growing expertise is required to ensure that serum concentrations max- prevalence of oxacillin (methicillin)-esistant Staphylococcus r imize efficacy and minimize toxicity (81, 82). aureus, and resistance to broad-spectrum beta-lactams and car- 2b. The antimicrobial regimen should be reassessed daily for bapenem among Gram-negative bacilli in some communities potential de-escalation to prevent the development of resis- and healthcare settings. Within regions in which the prevalence tance, to reduce toxicity, and to reduce costs (grade 1B). of such drug-resistant organisms is significant, empiric therapy adequate to cover these pathogens is warranted. Rationale. Once the causative pathogen has been identified, Clinicians should also consider whether candidemia is a the most appropriate antimicrobial agent that covers the pathogen likely pathogen when choosing initial therapy. When deemed and is safe and cost-effective should be selected. On occasion, warranted, the selection of empirical antifungal therapy (eg, an continued use of specific combinations of antimicrobials echinocandin, triazoles such as fluconazole, or a formulation might be indicated even after susceptibility testing is available 592 www.ccmjournal.org February 2013 • Volume 41 • Number 2