A case of back pain with resistant hypertension resulting from an anomalous accessory renal artery
•
1 recomendación•410 vistas

Jonathan Decker DO and Glenn Chapman III DO Larkin Community Hospital

Recomendados
Más contenido relacionado
La actualidad más candente
La actualidad más candente (19)
Destacado
Similar a A case of back pain with resistant hypertension resulting from an anomalous accessory renal artery
Similar a A case of back pain with resistant hypertension resulting from an anomalous accessory renal artery (20)
Más de Jack Michel MD
Más de Jack Michel MD (12)
Último
Último (20)
A case of back pain with resistant hypertension resulting from an anomalous accessory renal artery
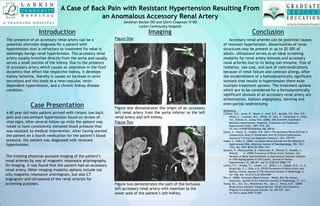
- 1. A Case of Back Pain with Resistant Hypertension Resulting From an Anomalous Accessory Renal Artery Jonathan Decker DO and Glenn Chapman III DO Larkin Community Hospital Introduction The presence of an accessory renal artery can be a potential alternate diagnosis for a patient with hypertension that is refractory to treatment for what is seemingly benign renal hypertension. The accessory renal artery usually branches directly from the aorta and usually serves a small portion of the kidney. Due to the presence of accessory artery which causes an alteration in the fluid dynamics that effect the respective kidney, it develops kidney ischemia, thereby it causes an increase in renin secretions and this leads to a reno-vascular, renin- dependent hypertension, and a chronic kidney disease condition. Imaging The treating physician pursued imaging of the patient’s renal arteries by way of magnetic resonance arteriography. On imaging, it was found that the patient had an accessory renal artery. Other imaging modality options include not only magnetic resonance arteriogram, but also CT angiogram and ultrasound of the renal arteries for screening purposes. Conclusion Accessory renal arteries can be potential causes of resistant hypertension. Abnormalities of renal structures may be present in up to 20-30% of adults. Ultrasound serves as an ideal screening modality for renal artery stenosis and accessory renal arteries due to its being non-invasive, free of radiation, low cost, and lack of contraindications because of renal failure and contrast allergy. After the establishment of a hemodynamically significant stenosis that results in hypertension there exist multiple treatment options. The treatment options which are to be considered for a hemodynamically significant stenosis of an accessory renal artery are embolization, balloon angioplasty, stenting and even partial nephrectomy. References Calhoun, D.A., Jones, D., Textor, S., Goff, D.C., Murphy, T.P., Toto, R.D., White, A., Cushman, W.C., White, W., Sica, D., Ferdinand, K., Giles, T.D., Falkner, B., Carey, R.M. (2008). AHA Scientific Statement: Resistant Hypertension: Diagnosis, Evaluation and Treatment. Hypertension 52(6), 1403-1419. doi: 10.1161/HYPERTENSIONAHA.108.189141 Gupta, A., Gupta, R., Singhla, R.K. (2011) The Accessory Renal Arteries: A Comparative Study in Vertebrates with Its Clinical Implications. Journal of Clinical and Diagnostic Research, 5(5). 970-973. Gupta, A., Tello, R. (2004). Accessory Renal Arteries Are Not Related to Hypertension Risk, American Journal of Roentgenology, 182. 1521- 1524. doi: 0361-803x/04/1826-1521 Kuczera, P., Wloszczynska, E., Adamczak, M., Pencak, P., Chudek, J., Wiecek, A. (2009).Frequency of Renal Artery Stenosis, and Variants of Renal Vascularization in Hypertensive Patients: Analysis of 1550 Angiographies in One Centre, Journal of Human Hypertension, 23, 396-401. doi:10.1038/jhh.2008.149 Lorenz, E.C., Vrtiska, T.J., Lieske, J.C., Dillon, J.J., Stegall, M.D., Li, X., Bergstralh, E.J., Rule, A.D. (2010) Prevalence of Renal Artery and Kidney, Clinical Journal of The American Society of Nephrology, 5, 431-438. doi: 10.2215/CJN.07641009 Ritz, E. (2006). Accessory Renal Arteries – Mostly, But Not Always, Innocuous, Journal of the American Society of Nephrology, 17. 3-11. Zhang, H.L., Sos, T.A., Winchester, P.A., Gao, J., Prince, M.R. (2009) Renal Artery Stenosis: Imaging Options, Pitfalls and Concerns. Progress in Cardiovascular Disease, 52, 209-219. doi: 10.1016/j.pcad.2009.10.003 Case Presentation A 60 year old male patient arrived with chronic low back pain and concomitant hypertension found on review of vital signs. After several follow-up visits the patient was noted to have consistently elevated blood pressure that was resistant to medical intervention. After having started the patient on a fourth medication for the patient’s blood pressure, the patient was diagnosed with resistant hypertension. Figure One Figure one demonstrates the origin of an accessory left renal artery from the aorta inferior to the left renal artery and left kidney. Figure Two Figure two demonstrates the path of the tortuous left accessory renal artery with insertion to the lower pole of the patient’s left kidney.