Nervous system / neurological involvement in ckd

This document discusses nervous system manifestations of chronic kidney disease (CKD). It covers several topics: 1. Neurological complications are common in CKD, affecting the central and peripheral nervous systems. Patients on dialysis tend to have reduced strength, activity levels and exercise capacity compared to healthy individuals. 2. Specific conditions discussed include peripheral neuropathy, carpal tunnel syndrome, autonomic neuropathy, cognitive dysfunction, uremic encephalopathy, dialysis disequilibrium syndrome, stroke, and myopathy. 3. Pathophysiology involves the retention of toxins in CKD that can damage nerves. Treatment focuses on renal replacement therapy through dialysis or transplantation to remove toxins from the body.

Recommended
More Related Content
What's hot
What's hot (20)
Viewers also liked
Viewers also liked (20)
Similar to Nervous system / neurological involvement in ckd
Similar to Nervous system / neurological involvement in ckd (20)
Recently uploaded
Recently uploaded (20)
Nervous system / neurological involvement in ckd
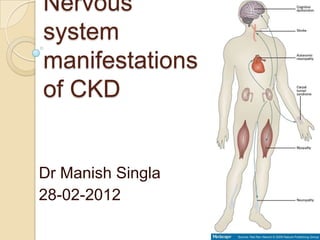
- 1. Nervous system manifestations of CKD Dr Manish Singla 28-02-2012
- 2. Introduction Neurological complications occur in almost all patients with severe CKD, potentially affecting all levels of the nervous system, from the CNS through to the PNS. Patients on dialysis tend to be weaker and less active, and to have reduced exercise capacity, when compared with healthy individuals Cognitive impairment, peripheral and autonomic neuropathy
- 3. Objectives Neuropathy Cognitive dysfunction Uremic encephalopathy Dialysis disequilibrium syndrome Stroke Myopathy
- 4. Neuropathy Peripheral neuropathy Carpal tunnel syndrome Autonomic neuropathy Pruritis
- 6. Peripheral neuropathy About 50 per cent of patients starting treatment had clinical evidence of a peripheral neuropathy in early days of dialysis Because of earlier initiation of dialysis these days, neuropathy is usually asymptomatic Nerve conduction abnormalities have been reported in up to 60% of patients receiving dialysis Abnormalities in motor nerve conduction velocity parallel the decline in GFR
- 7. Peripheral neuropathy Uremic neuropathy is a distal, symmetric, mixed sensorimotor polyneuropathy. Loss of ankle vibration sensation and the ankle jerk are often the first manifestations, progressing to a burning sensation in the feet, followed by motor deficit, such as weakness of ankle dorsiflexion
- 8. Peripheral neuropathy It typically involves the lower extremities more often than the upper extremities, and sensory symptoms precede motor symptoms. Motor involvement usually indicates advanced disease Progress to a stocking neuropathy with weakness and wasting of the distal leg muscles
- 9. Wasting of intrinsic hand muscles, with prominent bilateral atrophy of thenar muscles, in a patient with severe neuropathy resulting from chronic kidney disease
- 10. Pathophysiology of uraemic neuropathy Typically the large diameter axons in the distal nerve trunks supplying the legs are affected, with relative sparing of the unmyelinated and the small myelinated afferent neurons. Predominant defect is one of axonal loss with secondary demyelination Repeated episodes of demyelination followed by remyelination - onion like structures on nerve biopsies
- 11. Pathophysiology of uraemic neuropathy Biochemical pathogenesis of uraemic neuropathy is multifactorial Ouabain sensitive calcium ATPase pump activity has been shown to be decreased in uraemia, thereby affecting the sodium-calcium exchanger, and hence, reducing the normal calcium gradient Various uraemic toxins (middle molecules) have been proposed, including guanidine compounds, particularly methylguanidine which can inhibit the sodium ATPase pump, PTH Polyamines, phenol metabolites, myoinositol, and 3- carboxy-4-methyl-5-propyl-2-fluranpropanoic acid, (which inhibits organic acid transport) toxin induced inhibition of transketolase, and pyridoxal phosphate kinase
- 12. Transketolase Transketolase is a thiamine- dependent enzyme of pentose phosphate pathway. Found mainly in myelinated neurons. it maintains axon-cylinder myelin sheaths. Guanidinosuccinic acid can inhibit transketolase resulting demylination. It also inhibit excitatory synaptic transmission in CA1 region of hippocampus, contributing to cognitive syndrome in UE.
- 13. Pathophysiology of uraemic neuropathy Clinical symptoms and nerve conduction parameters improve rapidly following renal transplantation, often within days of surgery Rapidity of these changes suggests that toxin-mediated blockade of neural transmission has an important role in the neurological dysfunction associated with CKD.
- 15. Diagnosis of uremic neuropathy First step in the diagnosis of uremic neuropathy is to exclude other causes of neuropathy Serological testing should be undertaken to exclude vas-culitic neuropathy in those rapidly evolving weakness Nerve conduction studies (NCS) remain the gold standard in the diagnosis of uremic neuropathy. NCS demonstrate generalized neuropathy of the axonal type, with reductions in sensory amplitudes > motor amplitudes Sural sensory amplitude is the most sensitive indicator of uremic neuropathy
- 16. Systemic diseases that contribute to ESRD and also affect nerve function- ◦ Diabetes mellitus ◦ Amyloidosis ◦ SLE
- 17. Treatment Renal transplantation remains the only cure for uremic neuropathy and must be considered in any patient with progressive neuropathy. Rapidly progressive neuropathy is an accepted indication for patients to be triaged to urgent, nonmatched transplantation lists. Following transplantation, clinical recovery typically occurs over a period of 3-6 months
- 19. Carpal tunnel syndrome Carpal tunnel syndrome (CTS) is due to compression of the median nerve as it passes deep to the flexor retinaculum at the wrist, causing numbness, tingling, and burning sensations in the hand and fingers Attributable to dialysis-associated amyloidosis or ischemic mononeuropathy associated with an arteriovenous fistula. Prevalence of 26% in patients who have been on dialysis for more than 4
- 22. Carpal tunnel syndrome Pain is typically worse at night and during haemodialysis. Eventually weakness of thumb abduction occurs with wasting of the thenar eminence. CTS is more common in ◦ middle aged and older women ◦ diabetics ◦ patients with hypothyroidism ◦ patients on dialysis > 7 years
- 23. Carpal tunnel syndrome Diagnosis of CTS can be confirmed by measuring a delay in median nerve conduction across the wrist, and also by ultrasound of the wrist demonstrating bone cysts and distortion of the flexor tendons Haemodialysis with a high flux polyacrylonitrile, or haemodiafiltration, have been reported to reduce the deposition of β2- microglobulin
- 24. Carpal tunnel syndrome Splinting or local corticosteroid injections for mild disease Surgical decompression in cases where symptoms are either refractory to conservative treatments or where NCS have demonstrated changes indicative of axonal loss Extended carpal tunnel release procedure
- 26. Autonomic neuropathy Autonomic dysfunction is a common and potentially life-threatening complication of CKD, and can occur in the absence of length-dependent uremic neuropathy. More common in diabetics and elderly patients Cardiovascular autonomic dysfunction in CKD is associated with an increased risk of cardiac arrhythmia and sudden cardiac death
- 27. Impotence remains the most common symptom of autonomic dysfunction in CKD Other common clinical features include bladder and bowel dysfunction, impaired sweating, and orthostatic intolerance Intradialytic hypotension Renal transplantation leads to considerable improvement in autonomic function Sildenafil , midodrine
- 29. Objectives Neuropathy Cognitive dysfunction Uremic encephalopathy Dialysis disequilibrium syndrome Stroke Myopathy
- 31. Cognitive dysfunction Cognitive dysfunction increases in prevalence with CKD severity, potentially affecting up to 80% of patients Cognitive impairment in CKD not only increases the risk of mortality, but also has major implications for informed consent in relation to dialysis initiation and maintenance, and, ultimately, renal transplantation
- 32. Acute Cognitive Impairment In addition to chronic cognitive dysfunction and dementia, acute disturbances of cognition are prevalent in CKD. In the early days of dialysis, these acute disturbances frequently took the form of the 'dialysis disequilibrium syndrome'
- 33. Acute Cognitive Impairment Acute disturbances in cognitive function typically relate to metabolic abnormalities that complicate the uremic state, including electrolyte disturbances (for example, hypercalcemia, hypophosphatemi a and hyponatremia), acute fluid shifts during dialysis, which lead to cerebral hypoperfusion, and malignant hypertension
- 34. EFFECT OF HD Rapid variations in cognitive function was emphasized by a study of patients with CKD who underwent cognitive testing at multiple time points before and after a single dialysis session In these patients, global cognitive function varied markedly, with the greatest impairments being noted during the dialysis session, particularly with regard to memory, executive functioning and verbal fluency.
- 35. Chronic Cognitive Impairment and Dementia ◦ mild cognitive impairment, ◦ subclinical dementia, ◦ residual syndrome, and ◦ chronic dialysis-dependent encephalopathy
- 36. Chronic Cognitive Impairment and Dementia Moderate renal impairment that does not require dialysis is also associated with a significantly increased risk of dementia Cognitive tests demonstrate objective evidence of moderate to severe cognitive impairment in 70% of patients with CKD, with dysfunction most commonly noted in the domains of memory and executive function.
- 38. Dialysis dementia Dialysis dementia is a term reserved to describe a syndrome of progressive dementia related to aluminum intoxication and first described several decades ago when aluminum contamination of dialysate fluid and the use of aluminum-containing binders were more prevalent; however, this disorder is now rare.
- 39. Treatment :- DFO therapy
- 40. Pathophysiology of Cognitive Impairment vascular dementia high incidence of clinically silent cerebrovascular disease MRI studies have shown that clinically silent white matter disease is present in 50% of patients with CKD, compared with 10% in the general population Traditional and non traditional vascular risk factors (inflammatory mediators)
- 41. Pathophysiology of Cognitive Impairment Modern techniques of water purification and the use of non- aluminum phosphorus binders have, however, made aluminum intoxication a rare complication of CKD Potential roles of secondary hyperparathyroidism and anemia as risk factors for cognitive impairment PTH – neurotoxic
- 43. Clinical evaluation of dementia The Mini-Mental State Exam is the best known cognitive test for dementia screening and requires 7 to 10 minutes to administer. A score below 24 (out of a maximum score of 30) has a sensitivity and specificity of greater than 80% for dementia detection in the general population. Other cognitive tests that can be administered in 5 minutes or less, such as the clock drawing task, the Minicog (consisting of the clock drawing task plus uncued recall of three words), and the Short Portable Mental Status Questionnaire, have similar performance characteristics in the general population
- 44. Effects of Renal Transplantation Improvements in cognition in relation to baseline values were demonstrated 6 months after transplantation Improvements in both neuropsychological tests, such as the Mini-Mental State Examination, and neurophysiological markers of cognitive function, as measured using evoked potential latencies and EEG rhythms
- 45. Treatment Although kidney transplantation is optimal therapy for most patients with ESRD, many patients with chronic cognitive impairment may not be eligible for transplantation Intensification of the dialysis regimen remains a potential management strategy
- 46. EEG from a patient with uraemic encephalopathy. The recording is predominantly δ (4-8 Hz) and θ (4 Hz) wave activity, with no normal α (>8-13 Hz) or β (>13 Hz) waves
- 47. Uremic encephalopathy Uremic encephalopathy is an acute or subacute organic brain syndrome that regularly occurs in patients with acute or chronic renal failure when glomerular filtration rate declines to less than 10% of normal Seen in untreated or inadequately treated ESRD Characterized by lethargy and confusion in early stages and can progress to seizures or coma May be accompanied by other neurologic signs, such as tremor, myoclonus, or asterixis
- 50. Pathophysiology A large number of solutes are retained in uremia and several may have direct neurotoxicity or contribute indirectly to the pathogenesis of uremic encephalopathy by altering the blood– brain barrier. guanidine compounds, including guanidinosuccinic acid, methylguanidine, and homoarginine induce seizures, possibly through their effects on N-methyl-D-aspartic acid (NMDA) receptors or by modulating calcium channels ADMA, is a potent endogenous inhibitor of nitric oxide synthesis and causes cerebral vasoconstriction by impairing endothelial relaxation Anemia and hyperparathyroidism
- 51. A 50 year old male , known case of DM / ESRD on intermittent acute PD, getting HD sessions in between as well, past h/o smoking, receiving diuretics for edema, poor dietry intake, received one HD session from regional centre and brought in altered state ( history : duration?? ) On probing attendants gave h/o low grade fever for last 3-4 days Medication review – aluminium based phosphate binders, OHA tablets Residents notices some weakness on left side of body – but not sure Diagnosis : ………………..
- 53. Treatment After other causes of delirium have been ruled out, prompt treatment of uremic encephalopathy with initiation or intensification of renal replacement therapy is indicated. Resolution of symptoms typically occurs within days. Correction of anemia (i.e., hemoglobin <10 g/dL) may also be of benefit. Dietary protein restriction is another adjunctive measure used to delay the development of uremic symptoms,
- 54. A 12 year old male child, recently diagnosed to have b/I contracted kidneys, received 2 HD sessions at regional hospital and brought in altered state On probing attendants gave h/o low grade fever for last one day, headache and vomiting Diagnosis : ………………..
- 55. Dialysis disequilibrium syndrome Attributable to the dialysis procedure itself and is seen during or shortly after the first several dialysis treatments. It is most likely to occur in pediatric or elderly patients, patients with severe azotemia, and patients undergoing high-efficiency hemodialysis However, it has also been reported in patients undergoing peritoneal dialysis and maintenance hemodialysis Dialysis dysequilibrium is characterized by symptoms of headache, visual disturbance, nausea, or agitation and in severe cases, delirium, lethargy, seizures, and even coma.
- 56. Two hypotheses have been suggested to explain the development of brain edema. In the first, rapid removal of urea by dialysis leads to a urea gradient between the blood and brain, in turn leading to influx of water into the brain In the second theory, the formation of idiogenic osmoles within the brain contributes to the development of cytotoxic edema when an osmolar gradient is developed during dialysis. (MRI similarities with ODS)
- 57. Differential diagnosis of dialysis disequilibrium syndrome
- 60. Objectives Neuropathy Cognitive dysfunction Uremic encephalopathy Dialysis disequilibrium syndrome Stroke Myopathy
- 61. Stroke Compared with the general population, stroke event rates and stroke mortality rates are increased six- to 10- fold among patients on dialysis Like the general population, ischemic stroke is more common than hemorrhagic stroke Posterior circulation strokes involving the vertebrobasilar system occur more commonly in patients on dialysis than in the general population
- 62. Kidney transplantation is associated with 30% lower risk for stroke or TIA compared with patients remaining on the transplant wait list, allograft failure increases the risk for stroke or TIA by 150%
- 64. Risk factors Traditional risk factors Proteinuria was associated with a 50% to 70% increased risk for stroke (meta- analysis of stroke cohort studies involving more than 140,000) Dialysis related factor ◦ Intradialytic hypotension ◦ Overcorrection of anemia, especially in the setting of ultrafiltration, may lead to vascular stasis and thrombosis ◦ anticoagulation
- 65. Risk factors
- 66. Management Non contrast CT gadolinium-enhanced MR angiography must be carefully weighed against the potential benefits of the imaging procedure Safety, efficacy, and practicality of thrombolytic therapy in the setting of CKD and ESRD remain unclear In trials of thrombolytic therapy conducted in the setting of acute MI, patients with CKD were2-4 times as likely to experience major bleeding, including ICH Prevention – role of aspirin
- 67. Uremic myopathy Leads to proximal muscle weakness and wasting, predominantly in the muscles of the lower limbs Uremic myopathy typically develops with glomerular filtration rates of <25 ml/min, and has been associated with fatigability and reduced exercise capacity Electromyography and creatine kinase levels are generally normal, and the diagnosis is, therefore, made largely on clinical grounds. Muscle biopsy tends to demonstrate nonspecific features, including type II fiber atrophy with internalized nuclei and fiber
- 68. Possible etiologies include :- ◦ Hyperparathyroidism, ◦ Metabolic bone disease with vitamin D deficiency ◦ Impaired potassium regulation ◦ Accumulation of uremic toxins ◦ Carnitine deficiency, which can lead to mitochondrial dysfunction ◦ Malnutrition
- 69. summery
- 70. Key points Urenic toxin mediated disturbances in resting axonal membrane potential leads to length-dependent neuropathy in CKD ◦ Polyneuropathy ◦ Mononeuropathy ◦ Autonomic neuropathy Presentation in acute delirius/ confusional state is common in CKD patients and can have wide array of differential diagnosis Cognitive impairment is common in patients on dialysis, typically manifesting as a vascular-type dementia with prominent deficits in executive function Renal transplantation improves cognitive function, peripheral neuropathy and autonomic neuropathy Stroke is a common factor adding to morbidity and mortality in these patients. Management strategies - unclear Exercise programs, adequate nutritional intake and treatment
- 71. Medicolegal Pitfalls 71
- 72. Medicolegal Pitfalls 1. Failure to recognize RF as the cause of encephalopathy in a patient who presents with altered mental status. 2. Failure to promptly initiate dialysis in a patient with UE. 3. Failure to adequately monitor drug levels may lead to toxicity & further complications. 4. The slow onset of symptoms may lead to complications that might be grounds for litigation.
- 73. Thank you 73