Heart dysfunction protocol
•Descargar como PPTX, PDF•
5 recomendaciones•569 vistas

heart dysfunction protocol

Recomendados
Más contenido relacionado
La actualidad más candente
La actualidad más candente (20)
Destacado
Destacado (20)
Similar a Heart dysfunction protocol
Similar a Heart dysfunction protocol (20)
Más de Rakesh Verma
Más de Rakesh Verma (11)
Último
Último (20)
Heart dysfunction protocol
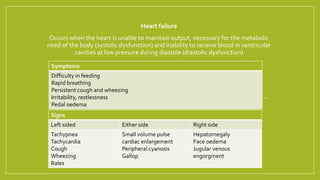
- 1. Heart failure Occurs when the heart is unable to maintain output, necessary for the metabolic need of the body (systolic dysfunction) and inability to receive blood in ventricular cavities at low pressure during diastole (diastolic dysfunction) Signs Left sided Either side Right side Tachypnea Tachycardia Cough Wheezing Rales Small volume pulse cardiac enlargement Peripheral cyanosis Gallop Hepatomegaly Face oedema Jugular venous engorgment Symptoms Difficulty in feeding Rapid breathing Persistent cough and wheezing Irritability, restlessness Pedal oedema
- 4. Step wise management Congestive Heart Failure Start digoxin and diuretics. Furesemide with spironolactone better than furosemide with K+ supplement Add ACE inhibitors, if persistant cough; change to ARB Add isosorbite nitrate if ACE are not tolerated Inadequate response especially if tachycardia, start carvedilol Consider once or twice weekly infusion of dobutamine who continue to deteriote. Add carnitine as supplement Consider for surgical treatment Rest, propped up position, humidified oxygen, diet, sodium restriction From : Ghai Paediatrics Last 2 step applicable especially to rare condition e.g. DCM
- 5. Initial therapy based on the sign and symptoms Suggestive sign and symptoms of low output state • Narrow pulse pressure • Altered mental sensorium • Cool extremities • Decrease urine output Suggestive sign and symptoms of volume overload • Dyspnoea • Increased JVP • Hepatomegaly • Rales • Peripheral odema • Recent weight gain • Increase BNP Mild volume overload IV Loop diuretics Is patient was on oral diuretics at home Moderate to severe volume overload • Fatigue • Oral diuretics • Spo2 <93% • Raised creatinine levels • May require CPCP,BIPAP,Ventilation Mild to moderate Consider very low output state • Narrow pulse pressure • Altered mental sense • Pre – renal azotemia • Cool extremities • Decreased urine output Management of Acute Decompensated Heart FailureFrom : AHA guideline
- 6. Give total oral dose as IV Give IV diuretics Furesemide 1mg/kg Adequate response NoYes Milrinone SBP normal Inadequate response Dobutamine May require inotrope support for BP On beta blocker therapy chronically No Yes Yes No No Step wise management as above Yes Add inotrops
- 7. IV DIURETICS + IVVASODILATOR If Furesemide was given, double the dose if not start with 1 mg/kg If SBP > lower limit according to age Start nitroglycerine 0.5-8mcg/min Or Nesiritide 0.01mcg/min Consider moderate to severe overload Or Low cardiac output state Consider moderate to severe overload Or Low cardiac output state
- 8. Doses (Nelson and Ghai) • Dopamine 5-20 mcg/kg/min • Dobutamine 5-20 mcg/kg/min • Milrinone 0.25-1 mcg/kg/min • Amrinone 3-10 mcg/kg/min • Nitroglycerine 0.25-5 mcg/kg/min • Isosorbide nitrate 0.01 mg/kg/day • Enalapril 0.1-1 mg/kg/day • Furesemide 1-3 mg/kg/day (oral) 1mg/kg/day (iv) • Spinolactone 1-3 mg/kg/day • Digoxin Premature 20 μg/kg Full term 20-30 μg/kg Infant and children 25-40 μg/kg Digitalisation (orally ) ½ dose initially followed by ¼ after 8 hours followed by ¼ dose after 16 hrs of 1st dose Maintainence 5-10 μg/kg/day
- 9. Comparison of Guidelines for the Management of Systolic Dysfunction* Drug class Heart Failure Society of America4 ACE inhibitors All patients with systolic dysfunction Beta blockers All patients in NYHA class II and III Insufficient evidence to recommend for patients in NYHA class IV Considered for patients in NYHA class I Spironolactone (Aldactone) “Considered for patients receiving standard therapy who have severe heart failure (class IV)” Diuretics All symptomatic patients, dosed as necessary to control symptoms Digoxin (Lanoxin) “Considered for patients who have symptoms of heart failure and NYHA class IV…while receiving standard therapy”