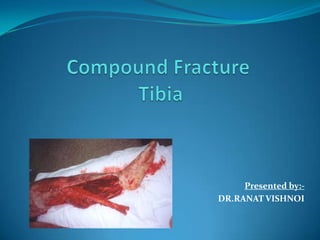
Compound Fracture Tibia
•Download as PPTX, PDF•
89 likes•26,721 views

compound fracture tibia is common ortthopaedic problem so hereby providing a detailed management by consulting various orthopaedic books. good luck..!!

Recommended
More Related Content
What's hot
What's hot (20)
Similar to Compound Fracture Tibia
Similar to Compound Fracture Tibia (20)
Recently uploaded
Recently uploaded (20)
Compound Fracture Tibia
- 2. INTRODUCTION An open fracture is one in which a break in the skin allows for direct communication of the fracture site or fracture hematoma with the elements external to the usual protection of the skin. The prognosis in open fractures is determined by :- the amount of devitalized soft tissue. the level and type of bacterial contamination. geometry of fracture.
- 3. Incidence Open fractures of the tibia are more common than in any other long bone Rate of tibial diaphysis fractures reported 2 per 1000 population and of these approximately one fourth are open tibia fractures.
- 4. PRINCIPLES OF MANAGEMENT ABC’S Assoc Injuries Tetanus Antibiotics Soft Tissue Management Fixation Long term issues
- 5. DIAGNOSIS The diagnosis of an open fracture is straight forward in most cases. An injured patient usually has:- bleeding deep laceration overlying or near a fracture of the underlying bone. In some cases, the fractured bone may be exposed. However, not all open fractures are obvious, and their timely and proper diagnosis and treatment depend on a careful examination of the patient, delineating salient features from the patient's history, a critical reading of x- rays, and good clinical judgment.
- 6. Examine the neurologic function and vascular function of each extremity. Note the state of circulation to the limb as indicated by capillary blush, the filling of veins, and the status of peripheral pulses. Examine meticulously for peripheral nerve function. Initial sensory examination by pressure and light touch gives a gross evaluation of limb sensation. Examination for motor function is difficult in the injured limb owing to pain and muscle spasm. The normal side should be compared with the abnormal side.
- 7. Mechanism of Injury Can occur in low energy, torsional type injury. (e.g. skiing) More common with high energy, direct force. (e.g. car bumper)
- 8. ENVIROMENTAL FACTOR The location where the injury occurred is essential to delineate. People exposed to feces or dirt may occur in a farm setting have possibility of clostridial infection and need additional antibiotics (penicillin) and more aggressive surgical debridement. In automobile collisions there is less risk for development of a clostridial infection. Unusual environments, such as a barnyards or gardens, streams or lakes, will likely be contaminated by unusual organisms, such as soil anaerobes and Aeromonas hydrophilia, respectively. Injuries caused by lawn-mowers and other motorized garden equipment are high-energy injuries with severe contamination. Animal Bite or presence of oral flora.
- 9. HISTORY The patient's tetanus immunity must be determined. The surgeon must also inquire about medical illnesses:- diabetes mellitus, peripheral vascular disease, liver disease, and any immune deficiency syndromes. Any previous injuries and their treatments. Finally, a history of smoking or chronic use of steroids.
- 10. Physical Examination Due to subcutaneous nature of tibia, deformity and open wound usually readily apparent. Circumferential inspection of soft tissue envelope, noting any lacerations, ecchymosis, swelling, and tissue turgidity necessary.
- 11. Neurologic and vascular exam of extremity must be done. Wounds should be assessed and then covered with sterile gauze dressing until treated or through digital camera / cell phone. True classification of wound best done after surgical debridement completed.
- 12. IMAGING EVALUATION Full length AP and lateral views from knee to ankle required for all tibia fractures. Ankle views suggested to examine mortise. Arteriography indicated if vascular compromise present after reduction .
- 13. Associated Injuries Approximately 30% of patients have multiple injuries. Fibula commonly fractured and its degree of comminution correlates with severity of injury. Proximal or distal tib-fib joints may be disrupted. Ligamentous knee injury and/or ipsilateral femur (‘floating knee’) more common in high energy fractures.
- 14. Neurovascular structures require repeated assessment. Foot fractures also common. Compartment syndrome must be looked.
- 15. CLASSIFICATION OF OPEN FRACTURES
- 16. HELPFUL FOR Communication between health care professionals Formulating a treatment plan Decision on limb salvage Detailed audit of care to ensure optimal management
- 17. METHODS OF CLASSIFICATION GRADING SYSTEM – focus on severity of limb injury only Eg: Gustilo Anderson , Tscherne and Gotzen, Byrd and Spicer etc SCORING SYSTEM – focuses on limb injury and general health; also give ‘amputation score’. Eg: MESS , NISSSA ,LSI,etc COMPREHENSIVE SYSTEM – combines the above two systems Eg: AO system , Ganga hospital score
- 18. GRADING SYSTEMS
- 19. Gustilo Anderson System In 1976 , Gustilo and Anderson treated 1025 open fractures based on his grading system that offered prognosis about outcome of infected fractures In 1984, it was modified and was based on a. Size of wound b. Soft tissue damage c. Periosteal stripping d. Vascular injury Segmental fractures, farmyard injuries, fractures occurring in a highly contaminated environment, shotgun wounds, or high-velocity gunshot wounds automatically result in classification as type III open fracture.
- 20. Type Wound Level of Soft Tissue Injury Bone Injury Contaminatio n I <1 cm long Clean Minimal Simple, minimal comminution II >1 cm long Moderate Moderate, some muscle Moderate comminution damage III Usually >10 cm long High Severe with crushing Usually comminuted; A soft tissue coverage of bone possible Usually >10 cm long High Loss of coverage; periosteal Bone coverage poor; B stripping & usually requires variable, may be soft tissue reconstructive moderate to severe surgery comminution Usually >10 cm long High Very severe loss of coverage Bone coverage poor; C plus vascular injury requiring variable, may be repair; may require soft tissue moderate to severe reconstructive surgery comminution
- 21. Tscherne System GRADE DESCRIPTION 1 Skin laceration mostly inside out injury with little or no contusion of skin 2 Skin laceration with circumscribed skin or soft tissue contusion with moderate contamination 3 Fractures with severe soft tissue injury often with NV injury , severe bone comminution or compartment syndrome 4 Sub total (remaining soft tissue not exceeding ¼ of limb circumference) or total amputation This system includes compartment syndrome which is not included in other grading systems
- 22. Byrd and Spicer TYPE DESCRIPTION I Both endosteal and periosteal supply intact and surrounding soft tissue is healthy II Endosteal supply interrupted but periosteal supply maintained by surrounding soft tissues III Devascularised bone fragment and requires flap coverage This system lacks sophistication and hence not widely used
- 23. SCORING SYSTEMS
- 24. Mangled Extremity Severity Score (MESS) TYPE CHARACTERISTICS INJURIES POINTS SKELETAL/ SOFT-TISSUE GROUP 1 Low energy Simple closed #, small calibre gun shot 1 2 Medium energy Open # , D/L , mulltiple level # 2 3 High energy Shot gun blast , high velocity gun shot 3 4 Massive crush Rail road, oil rig accidents 4 SHOCK GROUP 1 Normotensive BP stable in field and OT 0 2 Transiently BP unstable in field but responds to IV 1 hypotensive fluids 3 Prolonged SBP<90 in field and responding to IV 2 hypoptensive fluids only in OT
- 25. MESS Contd… TYPE CHARACTERISTICS INJURIES POINTS ISCHEMIA GROUP 1 None Pulsatile limb w/o signs of ischemia 0* 2 Mild Diminished pulses w/o signs of 1* ischemia 3 Moderate No pulse, sluggish capillary refill, 2* paraesthesia, motor activity 4 Advanced Pulseless, cool, paralysed, numb, no 3* capillary refill AGE GROUP 1 < 30 yrs 0 2 30 – 50 yrs 1 3 > 50 yrs 2 * If ischemia time > 6 hrs, add 2 points.
- 26. MESS Contd… It was developed to identify those patients who will be benefited by primary amputation In retrospective analysis, the outcome of injured limb was either salvage or amputation A score of 7 or greater is predictive of amputation. MESS is found to be specific but lacks some sensitivity which infers that score predicting limb salvage(<7) is more reliable than score predicting amputation (> or =7) (Bosse MJ JBJS 83A:412,2001)
- 27. Injury Severity Score (ISS) More recently, Rajasekaran et al. proposed a new scoring system for Gustilo type IIIA and IIIB open fractures of the tibia that evaluated skin coverage, skeletal structures, tendon and nerve injury, and comorbid conditions . The high specificity of this new scoring system may make it a much better predictor of amputation.
- 28. Injury Severity Score for Gustilo Type IIIA and IIIB Open Tibial Fractures Covering Structures: Skin and Fascia Wounds without skin loss Not over the fracture: 1 Exposing the fracture: 2 Wounds with skin loss Not over the fracture: 3 Over the fracture: 4 Circumferential wound with skin loss: 5 Skeletal Structures: Bone and Joints Transverse or oblique fracture or butterfly fragment <50% circumference: 1 Large butterfly fragment >50% circumference: 2 Comminution or segmental fractures without bone loss: 3 Bone loss <4 cm: 4 Bone loss >4 cm: 5
- 29. Functional Tissues: Musculotendinous and Nerve Units Partial injury to musculotendinous unit: 1 Complete but repairable injury to musculotendinous units: 2 Irreparable injury to musculotendinous units, partial loss of a compartment, or complete injury to posterior tibial nerve: 3 Loss of one compartment of musculotendinous units: 4 Loss of two or more compartments or subtotal amputation: 5 Comorbid Conditions: Add 2 Points for Each Condition Present Injury leading to débridement interval >12 h Sewage or organic contamination or farmyard injuries Age >65 y Drug-dependent diabetes mellitus or cardiorespirator diseases leading to increased anesthetic risk Polytrauma involving chest or abdomen with injury severity score >25 or fat embolism Hypotension with systolic blood pressure <90 mm Hg at presentation Another major injury to the same limb or compartment syndrome
- 30. Using this system, they divided type III open tibial fractures into four groups to assess the possibilities of limb salvage. Group 1 had scores of 5 or less. Group 2 had scores of 6 to 10. Group 3 had scores of 11 to 15 and, Group 4 had scores of 16 or greater. A score of 14 or greater is an indicator for amputation.
- 31. Other Scoring Systems • NISSSA – Nerve injury Ischemia Soft tissue injury Skeletal injury Shock & Age , is more sensitive and more specific than MESS. • LSI – Limb Salvage Index a.This index is applied to limbs with arterial injury b.Warm ischemia time together with scores for injured skin , muscle , bone , NV are added to give total score.
- 32. COMPREHENSIVE SYSTEMS
- 33. AO System : Skin lesions , muscle -tendon , NV , bone injuries are graded separately AO system allows better prediction of outcome when compared to Gustilo Due to its complexity not widely accepted • Ganga hospital score : Includes additional criteria like age >65 , DM , cardio- respiratory disease , trauma chest/abdomen, farmyard/sewage contaminations, delay in debridement >12h
- 34. ANTIBIOTIC A short course of first-generation cephalosporins, begun as soon as possible after injury, significantly lowers the risk of infection when used in combination with prompt, modern orthopaedic fracture wound management. A broad-spectrum antibiotic, first-generation cephalosporin + aminoglycoside, such as tobramycin or gentamicin, for highly contaminated wounds in which there is a risk of gram-negative contamination (Gustilo type III). If possibility of anaerobic organisms, such as Clostridium, high- dose penicillin is recommended. The duration of antibiotic treatment should be limited because in most series the infecting organisms are hospital acquired.
- 35. Gustilo recommended Type I and II - 2 g of cefamandole on admission and 1 g every 8 hours for 3 days. In type III - an aminoglycoside in dosages of 3 to 5 mg/kg daily. Farm injuries - add penicillin, 10 to 12 million U daily. Gustilo continued double antibiotic therapy for 3 days only and repeated the antibiotic regimen during wound closure, internal fixation, and bone grafting. Okike and Bhattacharyya recommended the administration of cefazolin, 1 g intravenously, every 8 hours until 24 hours after the wound is closed, with intravenous gentamicin (with weight- adjusted dosing) or levofloxacin (500 mg every 24 hours) added for type III fractures. Campbell recommend obtaining cultures when obvious clinical findings of infection are present at the second débridement.
- 36. MANAGEMENT
- 37. Initial Management ABC of initial management is addressed first. Compressive dressings for extremity hemorrhage.. Rule out cervical injuries , chest , abdominal injuries , head injuries in polytrauma patients . As soon as possible careful examination of wound is carried out and serial photographs of wound taken.
- 38. Initial wound management In emergency room : Don’t do digital exploration (to avoid infection and bleeding). Obvious Foreign Body are removed with forceps. If patient will undergo formal debridement in<1 hour just do sterile saline dressing if not irrigate with 1 or 2 ltr of NS. Povidone dressing alters color and impairs osteoblast function (controversial) so better avoided. Patients immunity to tetanus is determined. I.V. antibiotics are given as soon as possible .
- 39. Objectives of Surgical Treatment Prevent Sepsis Achieve Union Restore Function
- 40. DEBRIDEMENT Timing - Debridement done as soon as possible. Skin and wound preparation - dirt and debris removed by gentle scrub brush. Sterile tourniquets kept ready but not used. SUPERFICIAL DEBRIDEMENT: Traumatic wounds extended – to identify and explore the entire zone of injury and to access ends of bone fragments Skin incisions – extensile longitudinal incision to visualize deep tissue and can be extended till (N) tissue encountered. Clearly Nonviable skin and subcutaneous tissue excised but of marginal viability may be left for later debridement. Don’t detach skin and subcutaneous tissue from the fascia. Any nonviable shredded fascia and even the marginally viable ones excised.
- 41. Extensile longitudinal skin incision
- 42. DEEP DEBRIDEMENT: Where skin tend to tear , fascia split or shred , muscle because of water content are subjected to hydraulic damage by fluid waves during injury. In muscle debridement the concept ‘when in doubt take it out’. In type I,II and IIIa open # all non-vital and in doubt muscle can be debrided but IIIb and IIIc removal of entire muscle compartment may be needed so marginally viable ones are left for later re-debridement Viability of muscle checked by its 4C’s = color, capacity to bleed, contractility and consistency(last 2 more reliable).
- 43. Tendons , unless injured beyond repair should be preserved. In open wounds tendons are subject to dessication and hence it should be covered with soft tissues if not with moist dressings. In general bone devoid of soft tissue attachment removed and large ones are utilized provisionally for skeletal fixation and removed once fixation achieved. One exception to strict removal of bone without soft tissue attachment ,is significant portion of articular surface attached to bone fragment.
- 44. IRRIGATION After meticulous debridement irrigation of wound is done. Additives – antiseptics, antibiotics and surfactants can be used.
- 47. Skeletal Stabilization Once the vascular repair has been completed and limb salvaged or irrigation and debridement done , stabilization of bone is next concern. Restoring the length ,rotational and angular alignment has many benefits for healing of soft tissue fracture reduction unkinks NV conduits and helps in soft tissue healing minimizing motion of fragments also decreases further damage, pain and permits mobilization of joints
- 48. Stabilization of Open Tibia Fractures Multiple options depending on fracture pattern and soft tissue injury: Extra osseous immobilisation IM nail- reamed vs. unreamed External fixation ORIF
- 49. Extra Osseous Immobilisation Extra osseous immobilisation –eg: plasters ,weight bearing casts , splints and skeletal tractions Used in Low grade open fractures – eg: Grade-I Tibia # (plasters) and open shaft fractures (skeletal traction).
- 50. IM Nail IM Nail- currently the treatment of choice for grade I,II,IIIa and IIIb fractures. Excellent results with type 1 open fractures.
- 51. Unreamed IM Nail Time to union with unreamed nails can be prolonged- in one study of 143 open tibia fractures 53% were united at 6 months. Vast majority of fractures united, but 11% required at least one secondary procedure to achieve union.
- 52. Reamed Tibial Nailing In one study of type 2 and type 3a fractures good results- average time to union 24 and 27 weeks respectively; deep infection rate 3.5%. Complications increased with type 3b fractures- average time to union was 50 weeks and infection rate 23%.
- 53. External Fixation Used in high grade open fractures gives excellent access to wound dressing and surveillance possible. Compared to IM nails, increased rate of malunion and need for secondary procedures. Most common complication with ex-fix is pin track infection.
- 54. Conversion from Ex-Fix to IM Nail Conversion between ex- fix and IM nail. 9% infection 90%union. Infection rates decreased with shorter duration of ex-fix time.
- 55. Plate Fixation Traditional plating technique with extensive soft tissue dissection and devitalization has generally fallen out of favor for open tibia fractures. After meticulous debridement, copious irrigation with minimal stripping and accurate anatomical reduction in extraperiosteal plate fixation can be done. Increased incidence of superficial and deep infections compared to other techniques. In one study 13% patients developed osteomyelitis after plating compared to 3% of patients after ex-fix.
- 56. Percutaneous Plate Fixation Newer percutaneous plating techniques using indirect reduction may be a more beneficial alternative Large prospective studies yet to be evaluated
- 57. Gunshot Wounds Tibia fractures due to low energy missiles rarely require debridement and can often be treated like closed injuries Fractures due to high energy missiles (e.g. assault rifle or close range shot gun) treated as standard open injuries
- 58. Amputation Lange proposed two absolute indications for amputation of tibia fractures with arterial injury: crush injury with warm ischemia greater than 6 hours, and anatomic division of the tibial nerve. In general amputation performed when limb salvage poses significant risk to patient survival, when functional result would be better with a prosthesis, and when duration and course of treatment would cause intolerable psychological disturbance.
- 59. Bone Defects PMMA –aminoglycoside +/- vancomycin Bead pouch Solid spacer
- 60. Large Fragments: What to do? • Infection Rates with retained - 21% • Infection Rates with removed- 9% • Use to assist in determining length, rotation and alignment
- 61. Wound closure and coverage Wounds without skin loss : Definitive coverage should be performed within 7-10 days if possible. Most type 1 wounds will heal by secondary intent or can be closed primarily. Delayed primary closure usually feasible for type 2 and type 3a fractures. Tension free primary closure after thorough debridement Contraindications for primary closure are 1. Delayed presentation >12hr 2. Delayed administration of antibiotic >12hr 3. Deep seated contamination 4. Immunocompromised 5. NV injury 6. Inability to achieve tension free suture 7. High risk of anaerobic contamination like farm yard injuries
- 62. Wounds with skin loss: Type 3b fractures require either local advancement or rotation flap, split-thickness skin graft, or free flap.
- 63. Soft Tissue Coverage Proximal third tibia fractures can be covered with gastrocnemius rotation flap. Middle third tibia fractures can be covered with soleus rotation flap. Distal third fractures usually require free flap for coverage
- 64. Negative Pressure Would Therapy (NPWT)/ Vacuum Dressing Can lower need for free flaps Dedmond BT, The use of negative- pressure wound therapy (NPWT) in the temporary treatment of soft-tissue injuries associated with high-energy open tibial shaft fractures. J Orthop Trauma 2007 Cannot lower infection rates for Type IIIB open fractures Bhattacharyya T, Routine use of wound vacuum-assisted closure does not allow coverage delay for open tibia fractures. Plast Reconstr Surg 2008
- 66. BMPs BMP-2 (Infuse) FDA approval in subset of open tibia fractures BESTT study group JBJS 84, 2002 Significant reduction in the incidence of secondary procedures Accelerated healing Lower infections
- 67. COMPLICATIONS
- 68. Complications 1. Nonunion. 2. Malunion. 3. Infection- deep and superficial. 4. Compartment syndrome. 5. Fatigue fractures. 6. Hardware failure. 7. Chronic Osteomyelitis.
- 69. Nonunion Time limits vary from 6 months to one year Fracture shows no radiologic progress toward union over 3 month period Important to rule out infection Treatment options for uninfected nonunions include onlay bone grafts, free vascularized bone grafts, reamed nailing, compression plating, or ring fixator
- 70. Malunion In general varus malunion more of a problem than valgus In one study deformity up to 15 degrees did not produce ankle complications* For symptomatic patients with significant deformity treatment is osteotomy.
- 71. Deep Infection Often presents with increasing pain, wound drainage, or sinus formation. Treatment involves debridement, stabilization (often with ex-fix), coverage with healthy tissue including muscle flap if needed, IV antibiotics, delayed bone graft of defect if needed. Staged reconstruction with the used of PMMA + antibiotics.
- 72. Superficial Infection Most superficial infections respond to elevation of extremity and appropriate antibiotics (typically gram + cocci coverage) If uncertain whether infection extends deeper and/or it fails to respond to antibiotic treatment , then surgical debridement with tissue cultures necessary
- 73. Compartment Syndrome Diagnosis same as in closed tibial fractures Common with high energy tibia fractures Release ALL 4 compartments
- 74. Hardware Failure Usually due to delayed union or nonunion Important to rule out infection as cause of delayed healing Treatment depends on type of failure- plate or nail breakage requires revision, whereas breakage of locking screw in nail may not require operative intervention
- 75. Chronic Osteomyelitis Osteomyelitis is a common complication of compound fracture of long bones which is difficult to treat. Fever, Pain, swelling are seen in acute exacerbation of chronic osteomyelitis. Sequestrectomy and saucerization. Open Bone Grafting (Papineau Technique).
- 76. Management of sequelae of chronic osteomyelitis by Illizarov’s technique Group A – acute onset but ends up as chronic osteomyelitis with persistent infection A 1- no alteration in bone length bifocal osteosynthesis resection and bone transport A 2 – with limb length monofocal osteosynthesis and discrepancy lenthgning. A 3 – with deformities monofocal osteosynthesis and deformities correction A 4- with both length discrepancy monofocal or bifocal osteosynthesis and deformity with simultaneously lengthening and deformity correction A 5 – infective pseudoarthosis and bifocal osteosynthesis compression non union distraction or distraction – compression osteosynthesis
- 77. Outcomes
- 78. Outcomes Outcome most affected by severity of soft tissue and neurovascular injury Most studies show major change in results between type 3a and 3b/c fractures In one study of reamed nailing, the deep infection rate was 3.5% for type 2 and 3a fractures, but 23% for type 3b fractures* *Court-Brown JBJS 1991
- 79. Outcomes For type 3b and 3c fractures early soft tissue coverage gives best results In one study of 84 type 3b and 3c fractures, results with single stage procedure involving fixation with immediate flap coverage better than when coverage delayed more than 72 hours (deep infection 3% vs. 19%)* *Gopal et al. JBJS[Br] 2000
- 80. Suggested treatment algorithm Melvin JS, Open Tibial Shaft Fractures: I and II, JAAOS, Jan-Feb 2010
- 81. THANK YOU….!!