
Recomendados
Más contenido relacionado
Destacado
Destacado (15)
Similar a Korte-CSFCynoSOT13
Similar a Korte-CSFCynoSOT13 (20)
Más de Sven Korte, Dr. PhD.
Korte-CSFCynoSOT13
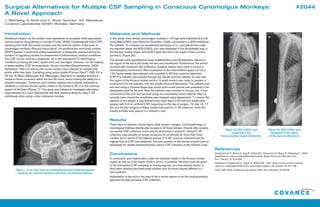
- 1. Introduction Intrathecal infusion via the lumbar route represents an accepted while specialized clinical route for drug delivery in humans (Tuner, 2003). Cerebrospinal fluid (CSF) sampling from both the lumbar location and the ventricle system of the brain of cynomolgus monkeys (Macaca fascicularis), the predominant nonhuman primate (NHP) species in preclinical safety assessment, is frequently required during the conduct of regulatory studies for assessment of inflammatory cerebral conditions. The CSF can be used as a diagnostic aid in the assessment of inflammatory conditions involving the brain, spinal cord, and meninges. However , for the majority of these studies, CSF for bioanalysis, clinical chemistry (Deisenhammer, 2006; Hambleton 1981) as well as cell counts needs to be collected at multiple time points within few days. Sampling using spinal needle (Pencan Paed®: 25G, 50 or 25 mm, B. Braun Melsungen AG, Melsungen, Germany) on sedated animals is limited to three occasions within the first 24 hours, hence limiting the ability for a detailed evaluation. Therefore, port catheter systems are routinely implanted to establish a constant access system either to the lumbar C SF or to the ventricle system of the brain (Figure 1). This study was initiated to investigate alternative subcutaneous (s.c.) port placements and their practical ability for easy C SF withdrawal when using a chair-restrained monkey. Materials and Methods In this study, three female cynomolgus monkeys (~3.5 kg) were implanted (L2-L3) using MID-LOVOL port (Solomon Scientific, USA), connected to a 3FR intrathecal PU catheter. To compare our established technique of s.c. port placement under the shoulder blade, the MID-LOVOL port was implanted in the est ablished way, in the thoraco-lumbar region (animal B; Figure 2a) and in the region of the s acrum (animal C; Figure 2b). The animals were anesthetized using medetomidine and (S)-ketamine, shaved in the region of the back and finally the skin was disinfected. Furthermore, the animal received pain treatment and antibiotics. Surgical drapes were used to ensure a sterile/aseptic environment. After localization of the intervertebral space L2/ L3 a 17G Tuohy needle was inserted until a positive C SF flow could be observed. A 3Fr PU catheter was pushed through the needle until the catheter tip reac hed the region of the thoraco-lumbar section. A small incision was made to prepare a small pouch for the catheter, with the needle removed afterwards. The catheter was secured using a Chinese-finger-trap suture and a small pocket was prepared in the designated area for the port. After the catheter was tunneled to the poc ket, it was connected to the port and secured using non-resorbable suture material. After all wounds were closed the anesthesia was stopped using atipamezole. To ensure the patency of the system it was flushed every three days in the first four weeks after surgery with 0.5 mL artificial CSF, beginning on the day of surgery. On day 14, 17, 20, and 23 after surgery a Huber needle was used for C SF collection, while the trained animals were placed in a restraint c hair. Results There were no adverse clinical signs, body weight c hanges, clinical pathology or neurological findings directly after surgery in all three animals. Directly after surgery , successful CSF collection could only be performed in animal C. Overall C SF collection was possible on single occasions for all animals for more than three months, but in animal C the highest amount of C SF could be collected and the highest flow of CSF was observed. The port position of this animal proved to be an advantage for needle insertion/fixation, hence CSF collection in the restraint chair. Conclusions In conclusion, port implantation under the shoulder blade, in the thoraco-lumbar region as well as in the region of the s acrum, is possible. Attention must be given to the anticipated CSF sampling or dosing regimen, as chair restraint (bolus or short-term infusion) and back-pack infusion over 24 hours require different s.c. port positions. Implantation of the port in the area of the s acrum seems to be the most promising approach for fast and easy CSF collection. Surgical Alternatives for Multiple CSF Sampling in Conscious Cynomolgus Monkeys: A Novel Approach J. Sternberg, S. Korte and C. Rose; Sponsor: G.F. Weinbauer Covance Laboratories GmbH, Münster, Germany #2044 Figure 1. X-ray scan from an intraventricular port implanted animal showing the ventricle system of the brain via contrast medium. 1a 1 Figure 2a. MID-LOVOL port implanted in the thoraco-lumbar region (Animal B). Figure 2b. MID-LOVOL port implanted in the region of the sacrum (Animal C). 2a 2b References Deisenhammer F., Bartos A., Egg R., Gilhus N.E., Giovannoni G., Rauer S., Sellebjerg F ., 2006: Guidelines on routine cerebrospinal fluid analysis. Report from an E FNS task force. Eur. J. Neurol. 13: 913-922. Hambleton P., Baskerville A., Wade J.J., Bailey N.E., 1981: Some normal clinical chemistry values for cerebrospinal fluid of the cynomolgus monkey, Lab. Animals 15:181-186. Turner, MS, 2003: Intrathecal drug delivery 2002, Act a Neurochir, 87:29-35.
- 2. Presented at the 52nd Annual SOT Meeting and ToxExpo™ San Antonio, Texas 10–14 March 2013 #2044 Surgical Alternatives for Multiple CSF Sampling in Conscious Cynomolgus Monkeys: A Novel Approach J. Sternberg, S. Korte and C. Rose; Sponsor: G.F. Weinbauer Covance Laboratories GmbH, Münster, Germany Covance is an independent, publicly held company with headquarters in Princeton, New Jersey, USA.Covance is an independent, publicly held company with headquarters in Princeton, New Jersey , USA. Covance is the marketing name for Covance Inc. and its subsidiaries around the world.Covance is the marketing name for Covance Inc. and its subsidiaries around the world. The Americas +1.888.COVANCE (+1.888.268.2623) +1.6 09.452.4440 Europe/Africa +800.2682.2682 +44.1423.500888 Asia Pacific +800.6568.3000 +65.6.5677333 Web Site: www.covance.com © COPYRIGHT 2013, COVANCE INC.© COPYRIGHT 2013, COVANCE INC.