
Recomendados
Más contenido relacionado
Destacado
Destacado (19)
Similar a Tsh scorecard corporate - 2010 11 q4 c
Similar a Tsh scorecard corporate - 2010 11 q4 c (20)
Más de The Scarborough Hospital
Más de The Scarborough Hospital (20)
Último
Último (20)
Tsh scorecard corporate - 2010 11 q4 c
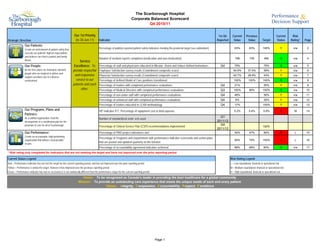
- 1. The Scarborough Hospital Corporate Balanced Scorecard Q4 2010/11 Our 1st Priority 1st Qtr Current Previous Current Risk Strategic Direction (to 30-Jun-11) Indicator Reported Value Value Target Status Rating* Page Our Patients: Create an environment of patient safety that Percentage of publicly reported patient safety indicators meeting the provincial target (see addendum) 63% 63% 100% Y n/a 2 exceeds our patients' highest expectations and delivers care that is patient and family Number of incident reports completed (medication and non-medication) 768 730 490 G n/a 4 driven. Service Our People: Excellence: To Percentage of staff and physicians educated in Mission, Vision and Values defined behaviours Q4 79% 75% G n/a 5 Be the first choice for motivated, talented provide respectful Employee Satisfaction survey results (Commitment composite score) 50.9% 37.5% 59% Y n/a 6 people who are inspired to deliver and and responsive Physician Satisfaction survey results (Commitment composite score) 42.7% 28.8% 43% Y n/a 7 support excellent care in a diverse environment. service to our Percentage of defined Model of Care positions transitioned 100% 100% 100% G n/a 8 patients and each Percentage of leaders with completed performance evaluations Q4 21% 50% Y n/a 9 other. Percentage of Medical Directors with completed performance evaluations Q3 100% 80% 100% G n/a 10 Percentage of non-union staff with completed performance evaluations Q4 46% 50% Y n/a 11 Percentage of unionized staff with completed performance evaluations Q4 6% 30% Y n/a 12 Percentage of leaders educated in LEAN methodology Q4 17% 100% Y n/a 13 Our Programs, Plans and HIT indicator #17, Percentage of equipment cost to total expense 5.2% 5.4% 5.9% R M 14 Partners: As a unified organization, lead the Q1 Number of standardized order sets used development of a coordinated plan for the 2011/12 provision of care for all of Scarborough. Percentage of Clinical Service Plan (CSP) recommendations implemented Q4 100% 2011/12 Our Performance: Percentage of PMO project milestones met 40% 47% 80% R L 15 Create an accountable, high performing Percentage of Programs and Departments with performance indicator scorecards and action plans organization that delivers measureable 65% 75% 100% R L 16 results. that are posted and updated quarterly on the Intranet Percentage of accountability agreement indicators achieved 88% 88% 80% G n/a 17 * Risk rating only completed for indicators that are not meeting the target and have not improved over the prior reporting period Current Status Legend: Risk Rating Legend Red = Performance indicator has not met the target for the current reporting period, and has not improved over the prior reporting period L = Low reputational, financial or operational risk Yellow = Performance is below the target, however it has improved over the previous reporting period M = Medium reputational, financial or operational risk Green = Performance indicator has met or exceeded or is not statistically different than the performance target for the current reporting period H = High reputational, financial or operational risk Vision: To be recognized as Canada’s leader in providing the best healthcare for a global community. Mission: To provide an outstanding care experience that meets the unique needs of each and every patient. Values: I ntegrity, C ompassion, A ccountability, R espect, E xcellence Page 1
- 2. The Scarborough Hospital Corporate Balanced Scorecard Quality Improvement Plan (QIP), Hospital Services Accountability Agreement (HSAA) and Publicly Reported Patient Safety Indicators (PRPSI) 1st Qtr 2011/12 QIP TSH Strategic Direction Indicator Indicator Origin QIP Dimension QIP Priority Rating Reported Current Value Previous Value 2010/11 Target Current Status Risk Rating* Target Page 1. Rate of Hospital Acquired C. difficile Associated Diarrhea (CDI) QIP / PRPSI Safety 2 0.50 0.47 0.33 R 0.28 A1 2. Rate of Central Line Infection (CLI) QIP / PRPSI Safety 1 1.48 0.00 0.79 R L 1.93 A2 3. Rate of Ventilator Associated Pneumonia (VAP) QIP / PRPSI Safety 2 0.00 0.61 1.33 G n/a 1.46 A3 Our Patients 4. Rate of hand hygiene compliance before initial patient/patient environment contact QIP Safety 2 83% 93% 90% R L 90% A4 5. Rate of hand hygiene compliance after patient/patient environment contact 90% 100% 90% G n/a A4 6. Rate of Hospital Acquired Methicillin Resistant Staphylococcus Aureus (MRSA) Bacteraemia PRPSI 0.00 0.00 0.02 G n/a A5 7. Rate of Hospital Acquired Vancomycin Resistant Enterococcus (VRE) Bacteraemia PRPSI 0.00 0.00 0.00 G n/a A6 8. Rate of Timely Administration of Prophylactic Antibiotics - Primary Hip PRPSI 100.0% 97.1% 96.1% G n/a A7 9. Rate of Timely Administration of Prophylactic Antibiotics - Primary Knee PRPSI 96.6% 97.7% 96.1% G n/a A8 10. WHO surgical checklist compliance 100% 100% 98% G n/a A9 11. Hospital Standardized Mortality Ratio (HSMR) QIP Effectiveness 2 74 84 100 G n/a 100 A10 12. 30 day readmission rate to any facility - All tracked CMGs QIP Effectiveness 2 14.5% 14.5% 14.5% G n/a 14.5% A11 13. Percentage of ALC days QIP / HSAA Effectiveness 1 15.9% 12.2% 12.2% R H 12.2% A12 14. Emergency Department Wait Time for High Acuity Visits - General Campus PRPSI 17:02 15:12 8:00 R H A14 15. Emergency Department Wait Time for High Acuity Visits - Birchmount Campus PRPSI 20:24 12:12 8:00 R H A15 16. Emergency Department Wait Time for Low Acuity Visits - General Campus PRPSI 5:16 4:48 4:00 R H A16 17. Emergency Department Wait Time for Low Acuity Visits - Birchmount Campus PRPSI 4:55 4:30 4:00 R H A17 18. Admitted patient treated within the LOS target of less than 8 hours - General Campus P4R 30% 32% 31% R H A18 19. Admitted patient treated within the LOS target of less than 8 hours - Birchmount Campus P4R 27% 34% 36% R H A19 20. Non-admitted high acuity patients treated within their respective targets of <=8 hours - General Campus P4R 91% 90% 87% G n/a A20 21. Non-admitted high acuity patients treated within their respective targets of <=8 hours - Birchmount Campus P4R 89% 91% 90% R H A21 22. Non-admitted low acuity patients treated within their respective targets of <=4 hours - General Campus P4R 85% 81% 81% G n/a A22 23. Non-admitted low acuity patients treated within their respective targets of <=4 hours - Birchmount Campus P4R 81% 83% 77% G n/a A23 24. 90th percentile physician initial assessment time - General Campus PRPSI 4:21 4:35 4:06 Y n/a A24 25. 90th percentile physician initial assessment time - Birchmount Campus PRPSI 3:40 3:06 3:48 G n/a A25 26. 90th Percentile ER Lengh of Stay for Admitted Patients QIP / HSAA Access 1 44:14 36:43 25:00 R H 25:00 A26 27. 90th Percentile ER Length of Stay for Complex Condition Patients QIP / HSAA Access 1 8:01 8:19 8:00 Y n/a 8:00 A27 28. Wait Time - General Surgery HSAA / PRPSI 76 67 182 G n/a A28 29. Wait Time - Cancer Surgery HSAA / PRPSI 53 54 84 G n/a A29 30. Wait Time - Cataract Surgery HSAA / PRPSI 120 225 182 G n/a A30 31. Wait Time - Total Hip Replacement HSAA / PRPSI 131 151 182 G n/a A31 32. Wait time - Total Knee Replacement HSAA / PRPSI 108 153 182 G n/a A32 33. Wait Time - CT HSAA / PRPSI 19 23 28 G n/a A33 34. Wait Time - MRI HSAA / PRPSI 97 116 28 Y n/a A34 35. Patient satisfaction - Overall Impression: Emergency Department QIP Patient-Centred 1 54.5 46.7 50 G n/a 50 A35 36. Patient satisfaction - Overall Impression: In-patients QIP Patient-Centred 1 59.2 66.3 70 R H 70 A36 37. Repeat Unplanned Emergency Visited within 30 Days for Mental Health Conditions HSAA Q1 2011/12 38. Repeat Unplanned Emergency Visited within 30 Days for Substance Abuse Conditions HSAA Q1 2011/12
- 3. 39. Total margin QIP / HSAA Effectiveness 1 0.04% -0.31% 0% G n/a 0% A38 40. Current Ratio HSAA 0.34 0.39 0.39 R M A39 41. Total weighted cases (Inpatient and Day Surgery) HSAA 42,144 43,027 40,712 G n/a A40 Our Performance 42. Mental Health Patient Days HSAA 15,970 15,425 15,000 G n/a A41 43. Rehab Patient Days HSAA 2,397 3,221 3,530 R M A42 44. Emergency Visits HSAA 103,351 99,915 98,000 G n/a A43 45. Ambulatory Visits (excluding ER) HSAA 306,954 303,662 294,773 G n/a A44 46. Total Hip and Knee Replacement HSAA 1,257 1,275 1,225 G n/a A45 47. Cataract Surgeries HSAA 5,756 5,894 5,815 R M A46 48. Computed Tomography (CT) HSAA 8,037 8,352 7,245 G n/a A47 49. Magnetic Resonance Imaging (MRI) HSAA 6,225 6,123 5,657 G n/a A48 * Risk rating only completed for indicators that are not meeting the target and have not improved over the prior reporting period Current Status Legend: Priority Legend Red = Performance indicator has not met the target for the current reporting period, and has not improved over the prior reporting period Priority 1 - Highest priority Yellow = Performance is below the target, however it has improved over the previous reporting period • Current performance below “benchmark” (if one exists) or below long term goal; significant improvements requ Green = Performance indicator has met or exceeded or is not statistically different than the performance target for the current reporting period • Aligned with organizational priorities/strategic plan, defined accreditation priority or recommendation, funding tied to initiative, aligned with government agenda Risk Rating Legend Priority 2 - Moderate priority: L = Low reputational, financial or operational risk • Current performance just below “benchmark” (if one exists) or below long term goal; room for improvement M = Medium reputational, financial or operational risk • Aligned with organizational priorities/strategic plan, defined accreditation priority or recommendation, funding H = High reputational, financial or operational risk tied to initiative, aligned with government agenda Priority 3 - Lower priority: • Current performance at/above” benchmark”, provincial rate or long term goal • Organizational priority Vision: To be recognized as Canada’s leader in providing the best healthcare for a global community. Mission: To provide an outstanding care experience that meets the unique needs of each and every patient. Values: I ntegrity, C ompassion, A ccountability, R espect, E xcellence
- 4. The Scarborough Hospital Corporate Balanced Scorecard Quality Improvement Plan (QIP), Hospital Services Accountability Agreement (HSAA) and Publicly Reported Patient Safety Indicators (PRPSI) Indicator QIP - Rate of Hospital Acquired C. difficile Associated Diarrhea Strategic Direction Our Patients Time Frame June 2011 Source Surveillance and Case Finding Performance Measurement Summary Definition 1.20 1.09, n=9 Overall Rate of hospital acquired C. difficile associated diarrhea. Rate is based on total number of inpatients/patients with confirmed infection per 1000 patient-days. 0.85, n=5 1.00 0.78, n=11 Significance To track hospital acquired C. difficile rates in order to identify and implement infection control measures to prevent nosocomial spread of C.difficile. While C. 0.80 0.58, n=5 0.58, n=5 difficile does not usually present a big problem for reasonably healthy adults, it can 0.53, n=5 0.51, n=3 0.50, n=7 0.49, n=3 0.49, n=3 be quite serious for those who are frail or have other health challenges. 0.48, n=4 0.47, n=7 0.47, n=7 0.47, n=7 0.47, n=3 0.46, n=4 0.45, n=4 0.45, n=4 0.43, n=6 C. difficile is communicable. It can live in the environment and on other surfaces. 0.60 0.38, n=6 0.37, n=3 0.36, n=3 Rigorous cleaning regimes, patient isolation and hand washing are some of the 0.35, n=5 0.34, n=2 0.34, n=5 0.34, n=2 0.33, n=2 0.32, n=5 strategies used to combat C. difficile. 0.26, n=4 0.26, n=2 0.25, n=2 0.25, n=2 0.24, n=2 0.23, n=2 0.22, n=3 0.22, n=3 0.22, n=3 0.40 CHART PLACEHOLDER 0.20, n=3 Target 0.17, n=1 0.16, n=1 0.15, n=1 0.15, n=1 0.15, n=2 Ontario Average - 0.33, lower value is desired. 0.13, n=1 0.13, n=1 0.07, n=1 Risk Rating 0.20 0.00, n=0 0.00, n=0 0.00, n=0 0.00, n=0 0.00, n=0 n/a Analysis - QIP use rate for January to December 2010. There have been a few months of Jul 10 Mar 10 Nov 10 Dec 10 Jan 11 Mar 11 Oct 10 Feb 10 Apr 10 May 10 Aug 10 Sep 10 Feb 11 Apr 11 May 11 Jun 10 Jun 11 increased cases of C. difficile at the General Campus since February 2010. Rates have begun to decline with increased monitoring and vigilance of infection control practices in the inpatient areas. The Birchmount Campus remains below the General Campus Birchmount Campus Ontario Average. TSH Ontario Average per 1,000 patient-days TSH Rolling 12-month Average QIP Reported Value=0.26 Action Plan SMART Initiative (Specific, Measureable, Attainable, Realistic, Time-Bound) Lead Date Initiated Current Status Indicator meeting or exceeding target, no action plan required n/a n/a n/a Page A1
- 5. The Scarborough Hospital Corporate Balanced Scorecard Quality Improvement Plan (QIP), Hospital Services Accountability Agreement (HSAA) and Publicly Reported Patient Safety Indicators (PRPSI) Indicator QIP - Rate of Central Line Infection (CLI) Strategic Direction Our Patients Time Frame Q1 2011/12 Source Surveillance and Case Finding Performance Measurement Summary Definition Overall rate of hospital acquired Central Line Infection. Rate is based on total 8.00 6.32, n=6 number of CLI incidents diagnosed after two days of Critical Care admission per 1000 patient days. 7.00 4.98, n=5 Significance 6.00 4.58, n=6 To track hospital acquired CLI rates in order to identify and implement necessary 3.90, n=6 prevention plans to reduce the risk of infection from spreading. 5.00 4.00 2.54, n=1 2.36, n=1 2.31, n=3 Target 2.21, n=2 2.06, n=3 Ontario Average - 0.79, lower value is desired. 1.87, n=1 3.00 CHART PLACEHOLDER 1.48, n=3 Risk Rating 0.78, n=1 2.00 0.69, n=1 0.62, n=1 Low - Controlling the rate of infection is very important to TSH. The increase in the rate of infection may cause some financial and reputational risk to the organization. 0.00, n=0 0.00, n=0 0.00, n=0 0.00, n=0 0.00, n=0 0.00, n=0 0.00, n=0 0.00, n=0 0.00, n=0 0.00, n=0 1.00 Analysis QIP use rate for January to December 2010. There has been a marked improvement to the number of CLI cases in 2010/11 at the General Campus. CLI 0.00 strategies to standardize processes across the campuses is showing improvements Q2 2009/10 Q3 2009/10 Q4 2009/10 Q1 2010/11 Q2 2010/11 Q3 2010/11 Q4 2010/11 Q1 2011/12 in the rates. There is lower rate of infection associated with PICC, therefore the use of PICC has been increased. General Campus Birchmount Campus TSH Ontario Average per 1,000 patient-days TSH Rolling 12-month Average QIP Reported Value=1.76 Action Plan SMART Initiative (Specific, Measureable, Attainable, Realistic, Time-Bound) Lead Date Initiated Current Status Monthly monitoring of insertions and maintenance Bundle which includes hand H. Clasky, D. Rose, P. Apr-10 Monthly audits hygiene, maximal barrier precautions, and chlorhexidine skin antisepsis and optimal Tamlin, R. Lovinsky, C. catheter side selection to adhere the compliance of 90% to decrease rate of CLI for Shelton the next quarter Expanded data collection to include the program that the hemodialysis patients are H. Clasky, R. Lovinsky, Mar-11 Data collection in progress coming from, type of line being used, and CLI reduction interventions such as the IPAC use of chlorhexidine dressing and bath to investigate higher rate of CLI in the hemodialysis population by Q2 of 2011/12 Page A2
- 6. Page A2
- 7. The Scarborough Hospital Corporate Balanced Scorecard Quality Improvement Plan (QIP), Hospital Services Accountability Agreement (HSAA) and Publicly Reported Patient Safety Indicators (PRPSI) Indicator QIP - Rate of Ventilator Associated Pneumonia (VAP) Strategic Direction Our Patients Time Frame Q1 2011/12 Source Surveillance and Case Finding Performance Measurement Summary Definition Overall Rate of hospital acquired Ventilator Associated Pneumonia. Rate is based 7.0 on total number of VAP incidents diagnosed after two days of Critical Care admission per 1000 patient days. 6.0 0.00, n=0 Significance 5.0 To track hospital acquired VAP rates in order to identify and implement necessary prevention plans to reduce the risk of development of pneumonia in the ICU patient population. 4.0 2.47, n=2 Target 3.0 1.63, n=2 Ontario Average - 1.33, lower value is desired. 1.58, n=2 1.40, n=1 1.36, n=2 CHART PLACEHOLDER 1.14, n=1 0.97, n=1 0.90, n=1 2.0 0.76, n=1 Risk Rating n/a 0.00, n=0 0.00, n=0 0.00, n=0 0.00, n=0 0.00, n=0 0.00, n=0 0.00, n=0 0.00, n=0 4.56, n=2 0.00, n=0 0.00, n=0 0.00, n=0 0.00, n=0 2.26, n=1 1.0 Analysis QIP use rate for January to December 2010. There were zero VAP case 0.0 identified in the Q4. Currently meeting target. Q2 2009/10 Q3 2009/10 Q4 2009/10 Q1 2010/11 Q2 2010/11 Q3 2010/11 Q4 2010/11 General Campus Birchmount Campus TSH Ontario Average per 1,000 patient-days TSH Rolling 12-month Average QIP Reported Value=1.22 Action Plan SMART Initiative (Specific, Measureable, Attainable, Realistic, Time-Bound) Lead Date Initiated Current Status Indicator meeting or exceeding target, no action plan required n/a n/a n/a Page A3
- 8. The Scarborough Hospital Corporate Balanced Scorecard Quality Improvement Plan (QIP), Hospital Services Accountability Agreement (HSAA) and Publicly Reported Patient Safety Indicators (PRPSI) Indicator QIP - Rate of hand hygiene compliance Strategic Direction Our Patients Time Frame Q1 2011/12 Source Surveillance and Case Finding Performance Measurement Summary Definition The single most common way of transferring health care-associated infections (HAIs) 140% in health care settings is on the hands of health care providers. Health care providers 100%, n=56 100%, n=56 100%, n=7 96%, n=392 96%, n=392 move from patient to patient and room to room while providing care and working in the 92%, n=1180 92%, n=1187 97%, n=58 96%, n=25 96%, n=25 96%, n=25 96%, n=25 120% 95%, n=57 93%, n=52 93%, n=52 93%, n=62 90%, n=301 90%, n=361 89%, n=412 patient environment. This movement provides many opportunities for the transmission 85%, n=1070 85%, n=1063 88%, n=354 87%, n=360 87%, n=360 90%, n=60 85%, n=391 84%, n=334 83%, n=330 88%, n=7 of organisms on hands that can cause infections. 81%, n=268 100% Significance Proper hand hygiene protects patients and providers and will reduce the spread of 80% infections and the associated treatment costs, reduce hospital lengths of stay and readmissions, reduce wait times, and prevent deaths. 60% Target. CHART PLACEHOLDER Ontario Target - 90% Before and 90% After, higher value is desired. 40% Risk Rating 20% 0%, n=0 0%, n=0 0%, n=0 0%, n=0 0%, n=0 0%, n=0 Low- Reputational, financial or operational risk. Analysis 0% QIP use rate for 2009/10, only for before patient contact. Due to the lack of hand Before After Before After Before After Before After Before After Before After hygiene auditors and the VRE issue, there were not enough audits done to report for Q3 at the General Campus. In Q4 IPAC trained unit based auditors to carryout the Q3 2009/10 Q4 2009/10 Q1 2010/11 Q2 2010/11 Q3 2010/11 Q4 2010/11 audits to meet mandatory reporting requirements. The results of the before compliance are below TSH target; however, well above the Ontario average of 72.17%. General Campus Birchmount Campus TSH Target QIP Reported Value=92.3% Action Plan SMART Initiative (Specific, Measureable, Attainable, Realistic, Time-Bound) Lead Date Initiated Current Status Development of a audit process to monitor unit based hand hygiene audits and IPAC Mar-11 In progress, on a monthly basis program overseen by IPAC and Decision Support. Monthly audit to observe number of times hand hygiene performed before patient contact. Page A4
- 9. The Scarborough Hospital Corporate Balanced Scorecard Quality Improvement Plan (QIP), Hospital Services Accountability Agreement (HSAA) and Publicly Reported Patient Safety Indicators (PRPSI) Indicator Rate of Hospital Acquired Methicillin Resistant Staphylococcus Aureus (MRSA) Bacteraemia Strategic Direction Our Patients Time Frame Q1 2011/12 Source Surveillance and Case Finding Performance Measurement Summary Definition 0.16 Overall Rate of hospital acquired Methicillin Resistant Staphylococcus Aureus (MRSA) bacteraemia. Rate is based on total number of inpatients/patients with 0.14 confirmed infection per 1000 patient-days. 0.12 Significance Higher MRSA colonization rates will lead to higher rates of blood stream infections 0.10 with MRSA. Tracking hospital acquired MRSA Bacteraemia rates helps to identify 0.06, n=1 the clinical significance of MRSA colonization. This will help identify a need for 0.08 further strategies to prevent nosocomial spread of MRSA. 0.04, n=1 0.04, n=1 0.04, n=1 0.04, n=1 Target 0.06 0.02, n=1 0.02, n=1 0.02, n=1 0.02, n=1 0.02, n=1 Ontario Average - 0.02, lower value is desired. 0.04 CHART PLACEHOLDER Risk Rating 0.00, n=0 0.00, n=0 0.00, n=0 0.00, n=0 0.00, n=0 0.00, n=0 0.00, n=0 0.00, n=0 0.00, n=0 0.00, n=0 0.00, n=0 0.00, n=0 0.00, n=0 0.00, n=0 0.00, n=0 0.00, n=0 0.00, n=0 0.00, n=0 0.00, n=0 0.00, n=0 n/a 0.02 0.00 Analysis Both General Campus and Birchmount Campus remains below the Ontario Average. General Campus Birchmount Campus TSH Ontario Average per 1,000 patient-days TSH Rolling 12-month Average Action Plan SMART Initiative (Specific, Measureable, Attainable, Realistic, Time-Bound) Lead Date Initiated Current Status Indicator meeting or exceeding target, no action plan required n/a n/a n/a Page A5
- 10. The Scarborough Hospital Corporate Balanced Scorecard Quality Improvement Plan (QIP), Hospital Services Accountability Agreement (HSAA) and Publicly Reported Patient Safety Indicators (PRPSI) Indicator Rate of Hospital Acquired Vancomycin Resistant Enterococcus (VRE) Bacteraemia Strategic Direction Our Patients Time Frame Q1 2011/12 Source Surveillance and Case Finding Performance Measurement Summary Definition Overall Rate of hospital acquired Vancomycin Resistant Enterococcus (VRE) 0.012 bacteraemia. Rate is based on total number of inpatients/patients with confirmed infection per 1000 patient-days. 0.010 Significance To track hospital acquired VRE bacteraemia rates in order to identify and implement 0.008 necessary prevention plans to reduce the risk of infection from spreading. 0.006 Target 0.004 Ontario Average - 0.00, lower value is desired. CHART PLACEHOLDER 0.00, n=0 0.00, n=0 0.00, n=0 0.00, n=0 0.00, n=0 0.00, n=0 0.00, n=0 0.00, n=0 0.00, n=0 0.00, n=0 0.00, n=0 0.00, n=0 0.00, n=0 0.00, n=0 0.00, n=0 0.00, n=0 0.00, n=0 0.00, n=0 0.00, n=0 0.00, n=0 0.00, n=0 0.00, n=0 0.00, n=0 0.00, n=0 0.00, n=0 0.00, n=0 0.00, n=0 0.00, n=0 0.00, n=0 0.00, n=0 Risk Rating 0.002 n/a 0.000 Analysis There have been no reportable cases of VRE bacteraemia despite increased numbers of VRE colonized patients since April 2010. General Campus Birchmount Campus TSH Ontario Average per 1,000 patient-days TSH Rolling 12-month Average Action Plan SMART Initiative (Specific, Measureable, Attainable, Realistic, Time-Bound) Lead Date Initiated Current Status Indicator meeting or exceeding target, no action plan required n/a n/a n/a Page A6