

Recomendados
Más contenido relacionado
La actualidad más candente
La actualidad más candente (20)
Similar a Symphysis & Angle MANDIBULAR FRACTURES
Similar a Symphysis & Angle MANDIBULAR FRACTURES (20)
Más de Dr-Faisal Al-Qahtani
Más de Dr-Faisal Al-Qahtani (20)
Último
Último (20)
Symphysis & Angle MANDIBULAR FRACTURES
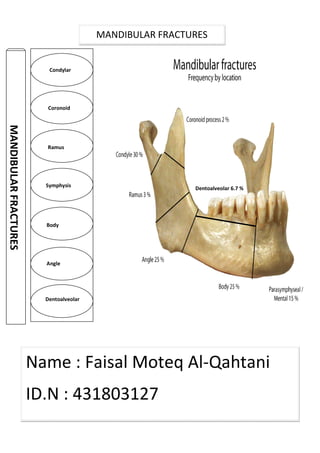
- 1. MANDIBULARFRACTURES Condylar Coronoid Ramus Symphysis Body Angle Dentoalveolar MANDIBULAR FRACTURES Name : Faisal Moteq Al-Qahtani ID.N : 431803127 Dentoalveolar 6.7 %
- 2. Problem • Fractures that occur in the midline of the mandible are classified as present, the fracture line passes between the mandibular central incisors. • Fractures occurring in the area of the mandible from cuspid to cuspid, but not in the midline, are classified as parasymphyseal • The etiology of symphyseal and parasymphyseal fractures is largely from trauma from interpersonal violence or motor • Falls, industrial accidents, and sports injuries are lesser etiologies. • Most trauma is blunt, but penetrating trauma is common with interpersonal violence and war injury. Mandibular Parasymphyseal Fractures The broad red line indicates t The pink area between the cuspid teeth, excepting the symphysis, indicates the parasymphyseal area Etiology Fractures that occur in the midline of the mandible are classified as present, the fracture line passes between the mandibular central incisors. Fractures occurring in the area of the mandible from cuspid to cuspid, but not in the midline, are . The etiology of symphyseal and parasymphyseal fractures is largely from trauma from interpersonal violence or motor vehicle accidents. Falls, industrial accidents, and sports injuries are lesser etiologies. Most trauma is blunt, but penetrating trauma is common with interpersonal violence and war Mandibular Parasymphyseal Fractures " Symphysis " The broad red line indicates the symphyseal area. The pink area between the cuspid teeth, excepting the symphysis, parasymphyseal area. Fall Fractures that occur in the midline of the mandible are classified as symphyseal. When teeth are present, the fracture line passes between the mandibular central incisors. Fractures occurring in the area of the mandible from cuspid to cuspid, but not in the midline, are The etiology of symphyseal and parasymphyseal fractures is largely from trauma from Most trauma is blunt, but penetrating trauma is common with interpersonal violence and war " Symphysis " The pink area between the cuspid teeth, excepting the symphysis,
- 3. • The patient has a history of trauma. Pain and tenderness are present about the anterior mandible, and the patient reports malocclusion. False motion of the mandible is usually evident. • Preoperative examinations are often impaired by tenderness and masticatory muscle spasm; therefore, a thorough reexamination of the face and oral cavity is performed prior to definitive therapy. • The entire mandible is carefully inspected and palpated. All teeth are inspected and evaluated for injury and mobility. • A survey of the dental arches is completed to detect any sockets missing teeth. The maxilla is examined to detect any previously missed injuries. • Fractures of the symphysis/parasymphysis are inherently unstable. • Muscles of mastication insert into posterior portions of the mandible with a net effect of superior rotation about the axis of the temporomandibular joint. • The suprahyoid muscles of the neck act directly on the anterior mandible, with a net effect of inferior rotation around the axis of the temporomandibular joint and scissoring motion around a vertical axis through the symphysis. The later action is from the mylohyoid muscles. • Fractures of the anterior mandible lack 2 of the stabilizing factors provided to fractures of the posterior tooth-bearing mandible: the splinting effects of the masseter and internal pterygoid muscles, which form a natural sling, and the interlocking cusps and fossae of bicuspid and molar teeth. • Presence of a symphyseal/parasymphyseal fracture is the indication for treatment. • Mode of treatment varies among patients. Diagnosis R. Anatomy Indications
- 4. • The only absolute contraindication to managing these fractures exists if the patient is not stable enough to undergo the needed treatment. • A specific contraindication for maxillomandibular fixation (MMF) is poorly controlled seizures. • Patients with uncleared cervical spines present limitations regarding which treatment for facial fractures is safe. • Essentially all symphyseal and parasymphyseal fractures are open to the mouth and, thus, are grossly contaminated. • Antibiotic coverage is essential through the time of initial treatment and early healing. Penicillin is the drug of choice. • Occasionally, fractures on the anterior mandible are nondisplaced and stable. • Most fractures are displaced and unstable, requiring a more aggressive approach to therapy. • Before rigid internal fixation became popular, symphyseal and parasymphyseal fractures were usually treated with open reduction with interosseus wiring combined with MMF. In some patients, a lingual splint was required to affect the desired degree of stability. • A medically stable patient with a mandible fracture should receive definitive care as soon as is practical. • A stable patient, evaluation by the anesthetist, and informed consent, The anesthesia team needs to know that nasal intubation is required. Contraindication Medical therapy Surgical Therapy Preoperative
- 5. • The patient is placed in the supine position and nasally intubated by the anesthesia team. Usually, headlights offer the best illumination. • The fracture site may be approached via an intraoral incision, extraoral incision, or laceration. • Prior to exposing the fracture line reduction of the fracture, places the posterior teeth into occlusion, and produces some stability at the alveolar margin. • After adequate exposure of the fracture lines, anatomic reduction is achieved occlusion and alignment of teeth on either side of fracture lines should confirm that proper reduction has been accomplished. • Rigid hardware is then placed with attention to the technique appropriate for the system chosen. When using the Champy miniplate system inferior margin and the other at the alveolar level as seen in the image below. When using the titanium craniofacial system techniques level is required as seen in the image below, to avoid distraction at the lingual surface of the mandible, dynamic compression plates should be overcontoured by 3 Intraoperative Two miniplates are required for the symphysis/parasymphysis region because it is subjected to torsio miniplate. Tension banding is required to prevent splaying of the fracture line at the superior surface of the mandible when using a dynamic compression plate. A mandibular arch bar can accompli d in the supine position and nasally intubated by the anesthesia team. Usually, headlights offer the best illumination. The fracture site may be approached via an intraoral incision, extraoral incision, or laceration. Prior to exposing the fracture line, the patient is placed in MMF, this accomplishes a gross reduction of the fracture, places the posterior teeth into occlusion, and produces some stability After adequate exposure of the fracture lines, anatomic reduction is achieved occlusion and alignment of teeth on either side of fracture lines should confirm that proper reduction has been accomplished. Rigid hardware is then placed with attention to the technique appropriate for the system Champy miniplate system, two plates are required, inferior margin and the other at the alveolar level as seen in the image below. titanium craniofacial system techniques , tension banding at the alveolar level is required as seen in the image below, to avoid distraction at the lingual surface of mandible, dynamic compression plates should be overcontoured by 3 are required for the symphysis/parasymphysis region because torsional forces, which would be poorly resisted by one is required to prevent splaying of the fracture line at the superior surface of the mandible when using a dynamic compression plate. A mandibular arch bar can accomplish this. In this example, a miniplate is used. d in the supine position and nasally intubated by the anesthesia team. The fracture site may be approached via an intraoral incision, extraoral incision, or laceration. his accomplishes a gross reduction of the fracture, places the posterior teeth into occlusion, and produces some stability After adequate exposure of the fracture lines, anatomic reduction is achieved. Inspection of the occlusion and alignment of teeth on either side of fracture lines should confirm that proper Rigid hardware is then placed with attention to the technique appropriate for the system e required, first plate at the inferior margin and the other at the alveolar level as seen in the image below. tension banding at the alveolar level is required as seen in the image below, to avoid distraction at the lingual surface of mandible, dynamic compression plates should be overcontoured by 3-5°. are required for the symphysis/parasymphysis region because , which would be poorly resisted by one is required to prevent splaying of the fracture line at the superior surface of the mandible when using a dynamic compression plate. A sh this. In this example, a miniplate is used.
- 6. When the fracture is midline, an alternative to plate fixation is the use of opposing lag screws as seen in the image below. The fracture must be anatomically reduced prior to drilling the holes. In choosing roots. This is not a method for the inexperienced surgeon, and it requires careful planning and exacting technique. additional stability. • After placement of rigid internal fixation, most surgeons remove the patient from MMF. • If interosseus wiring is used, MMF is required for 4 • Analgesics and antibiotics are indicated postoperatively. Analgesics are usually required for several days. An?bio?cs for 7 • If MMF is used, precautions to help prevent and/or deal with nausea and vomiting are paramount. • If the MMF technique includes having wires hold the teeth in occlusion, a wire should be with the patient for the first day. Opposing lag screws have been used to treat a symphyseal fracture. This procedure requires precise technique and is not for the occasional operator. Postoperative When the fracture is midline, an alternative to plate fixation is the use of opposing lag screws as seen in the image below. The fracture must be anatomically reduced prior to drilling the holes. In choosing the locations for the screws, care is taken to avoid tooth roots. This is not a method for the inexperienced surgeon, and it requires careful planning and exacting technique. When using this techniques , consider using a lingual splint for After placement of rigid internal fixation, most surgeons remove the patient from MMF. rosseus wiring is used, MMF is required for 4-6 weeks. Analgesics and antibiotics are indicated postoperatively. Analgesics are usually required for several days. An?bio?cs for 7-10 days postopera?vely should provide good infec?on If MMF is used, precautions to help prevent and/or deal with nausea and vomiting are If the MMF technique includes having wires hold the teeth in occlusion, a wire should be with the patient for the first day. have been used to treat a symphyseal fracture. This procedure requires precise technique and is not for the occasional operator. When the fracture is midline, an alternative to plate fixation is the use of opposing lag screws as seen in the image below. The fracture must be anatomically reduced prior to the locations for the screws, care is taken to avoid tooth roots. This is not a method for the inexperienced surgeon, and it requires careful planning When using this techniques , consider using a lingual splint for After placement of rigid internal fixation, most surgeons remove the patient from MMF. Analgesics and antibiotics are indicated postoperatively. Analgesics are usually required for 10 days postopera?vely should provide good infec?on prevention. If MMF is used, precautions to help prevent and/or deal with nausea and vomiting are If the MMF technique includes having wires hold the teeth in occlusion, a wire-cutting device have been used to treat a symphyseal fracture. This procedure
- 7. • After discharge from the hospital, the patient should be seen weekly and as needed. Nutritional status, wound healing, oral hygiene, maintenance of secure occlusion, and signs of infection should be assessed during weekly examinations. • Malunion/malocclusion is the most common major complication and results from inadequate reduction and/or loss of reduction during the healing process. • Infection is usually localized and usually responds to antibiotics. Collections of pus should be drained, and hardware, if any, may require removal. • Exposure of implanted hardware requires removal of hardware. • A united fracture with normal dental occlusion is the expected outcome. Once this result is obtained, the prognosis for the future is excellent. Follow-up Complications Prognosis
- 8. • Mandible fractures are also described by the relationship between the direction of the fracture line and the effect of muscle distraction on fracture fragments. • Mandible fractures are favorable when muscles tend to draw bony fragments together and unfavorable when bony fragments are displaced by muscle forces. • Vertically unfavorable fractures allow distraction of fracture segments in a horizontal direction. • These fractures tend to occur in the body or symphysis • Horizontally unfavorable fractures allow displacement of segments in the vertical plane. Mandibular Background A: Horizontally unfavorable. C: Vertically unfavorable. Mandible fractures are also described by the relationship between the direction of the fracture line and the effect of muscle distraction on fracture fragments. Mandible fractures are favorable when muscles tend to draw bony fragments together and unfavorable when bony fragments are displaced by muscle forces. Vertically unfavorable fractures allow distraction of fracture segments in a horizontal direction. These fractures tend to occur in the body or symphysis-parasymphysis area. Horizontally unfavorable fractures allow displacement of segments in the vertical plane. Mandibular angle Fractures A: Horizontally unfavorable. B: Ho C: Vertically unfavorable. D: Vertically favorable. Mandible fractures are also described by the relationship between the direction of the fracture Mandible fractures are favorable when muscles tend to draw bony fragments together and Vertically unfavorable fractures allow distraction of fracture segments in a horizontal direction. parasymphysis area. Horizontally unfavorable fractures allow displacement of segments in the vertical plane. B: Horizontally favorable. D: Vertically favorable.
- 9. • The angle of the mandible is the triangular region bounded by the anterior border of the masseter muscle to the posterior and superior attachment of the masseter muscle (usu to the third molar), this area is fracture . • Vehicular accidents and assaults are the primary causes of mandibular fractures throughout the world. • Assault most often causes mandible angle fractures. Problem Etiology Data from industrialized nations suggest that mandible fractures have various causes as follows: The angle of the mandible is the triangular region bounded by the anterior border of the masseter muscle to the posterior and superior attachment of the masseter muscle (usu to the third molar), this area is fracture . Vehicular accidents and assaults are the primary causes of mandibular fractures throughout the Assault most often causes mandible angle fractures. Data from industrialized nations suggest that mandible fractures have various causes as follows: The angle of the mandible is the triangular region bounded by the anterior border of the masseter muscle to the posterior and superior attachment of the masseter muscle (usually distal Vehicular accidents and assaults are the primary causes of mandibular fractures throughout the Data from industrialized nations suggest that mandible fractures have various causes as follows:
- 10. History • Obtain a thorough history specific to preexisting systemic bone disease, neoplasia, arthritis, collagen vascular disorders, and temporomandibular joint (TMJ) dysfunction. • Knowledge of the type and direction of the causative traumatic force helps determine the nature of injury, also assists the clinician in suspecting and diagnosing additional fractures. Physical examination • Change in occlusion may be evident on physical examination. Any change is highly suggestive of mandibular fracture. Ask the patient to compare postinjury and preinjury occlusion. • Posttraumatic premature posterior dental contact (anterior open bite) and retrognathic occlusion may result from a mandibular angle fracture. Unilateral open bite deformity is associated with a unilateral angle fracture. • Change in facial contour or loss of external mandibular form may indicate mandibular fracture, an angle fracture may cause the lateral aspect of the face to appear flattened. Loss of the mandibular angle on palpation may be because of an unfavorable angle fracture in which the proximal segment rotates superiorly. The anterior face may be displaced forward, causing elongation. • Lacerations, hematoma, and ecchymosis may be associated with mandibular fractures. Their presence should alert the clinician that thorough investigation is necessary to exclude fracture. • Use the simplest means possible to reduce and fixate a mandibular fracture. Because open reduction can carry an increased morbidity risk. • Use closed techniques for Nondisplaced favorable fractures • Indications for open reduction include Displaced unfavorable angle, body, or parasymphyseal fractures. Diagnosis Indications
- 11. • Evaluate and monitor the patient's general physical condition prior to treating mandibular fractures.any force capable of causing a mandibular fracture may also injure other organ systems. • Bilateral cervical subcutaneous emphysema, pneumothorax, pneumomediastinum, and spleen lacerations have also been associated with mandible fractures after trauma, patients should not undergo surgical reduction of mandible fractures until these issues are addressed. Multiple approaches for open reduction and internal fixation (ORIF) exist. Consider fracture location, nerve position, and skin-crease lines when choosing the appropriate approach. Intraoral approach • The intraoral approach is usually used in fractures that are nondisplaced or only slightly displaced. The mandible base may require additional stab incisions to place screws for plate fixation. Intraoral lacerations may be used for access in fixation of mandible fractures. • Local anesthesia may be sufficient for simple or nondislocated fractures when 1-plate fixation is required. Extraoral approach • External incisions are usually necessary with fractures that have a high degree of dislocation or with comminuted fractures, since placing longer and stronger plates is difficult via the intraoral approach. • General anesthesia is indicated in the extraoral approach, give careful attention to the marginal mandibular branch of the facial nerve. Contraindications Surgical Therapy
- 12. Transverse fracture line without displacement • Semirigid fixation using miniplates and monocortical screws may be used in a transverse fracture line with limited exposure. • This fracture is better managed using two first in the area of the oblique line and the second at the inferior border. Fixation is also possible using a single lag screw in the anteroposterior Transverse fracture and its fixation are seen in the image below. e line without displacement Semirigid fixation using miniplates and monocortical screws may be used in a transverse fracture is better managed using two miniplates (4-6 holes, 2-3 screws on each side), the n the area of the oblique line and the second at the inferior border. Fixation is also possible using a single lag screw in the anteroposterior-oblique approach in nonosteoporotic bones. Transverse fracture and its fixation are seen in the image below. Semirigid fixation using miniplates and monocortical screws may be used in a transverse fracture 3 screws on each side), the n the area of the oblique line and the second at the inferior border. Fixation is also possible oblique approach in nonosteoporotic bones.
- 13. Transverse fracture line with displacement • With dislocation, the medial pterygoid and masseter muscles cause vertically and horizontally unfavorable vector forces, which make reduction more difficult. • For a minimally displaced fracture, achieve reduction to the proximal fragment on the medial aspect of the anterior border of the ramus using 2 screws. Reduce the fracture using the plate as a handle to complete IMF. Bend the free end of the plate to conform to the distal oblique ridge and fix with monocortical screws. • A widely displaced fracture may require stabilization by using a reconstruction plate. Angular fractures with basal triangle • As with displaced fractures, use an angulated 2.4 reconstruc?on plate wi of the mandible aHer IMF. The triangle can be fixed to the plate, or lag screws (2.0, 2.4) can be placed. Use a 2.0 miniplate along the oblique line. Comminuted angular fractures • These often occur in association with other mandibu • After temporary IMF, reduction and fixation of fragments within simpler fractures can be accomplished using 1.5 or 2.0 miniplates and lag screws and then bridging with a 2.4 reconstruction plate. Miniplates are often used to re angular fracture. a: Transverse and longitudinal fractures. b: A lag screw and reconstruction plate used to provide fixation. Transverse fracture line with displacement With dislocation, the medial pterygoid and masseter muscles cause vertically and horizontally unfavorable vector forces, which make reduction more difficult. For a minimally displaced fracture, achieve reduction by fixing a 2.0 miniplate of suitable length to the proximal fragment on the medial aspect of the anterior border of the ramus using 2 screws. Reduce the fracture using the plate as a handle to complete IMF. Bend the free end of he distal oblique ridge and fix with monocortical screws. A widely displaced fracture may require stabilization by using a reconstruction plate. Angular fractures with basal triangle As with displaced fractures, use an angulated 2.4 reconstruc?on plate wi of the mandible aHer IMF. The triangle can be fixed to the plate, or lag screws (2.0, 2.4) can be placed. Use a 2.0 miniplate along the oblique line. These often occur in association with other mandibular and maxillary fractures. After temporary IMF, reduction and fixation of fragments within simpler fractures can be accomplished using 1.5 or 2.0 miniplates and lag screws and then bridging with a 2.4 reconstruction plate. Miniplates are often used to reduce large fragments of a comminuted : Transverse and longitudinal fractures. : A lag screw and reconstruction plate used to provide fixation. With dislocation, the medial pterygoid and masseter muscles cause vertically and horizontally by fixing a 2.0 miniplate of suitable length to the proximal fragment on the medial aspect of the anterior border of the ramus using 2-3 screws. Reduce the fracture using the plate as a handle to complete IMF. Bend the free end of he distal oblique ridge and fix with monocortical screws. A widely displaced fracture may require stabilization by using a reconstruction plate. As with displaced fractures, use an angulated 2.4 reconstruc?on plate with 6-8 holes at the base of the mandible aHer IMF. The triangle can be fixed to the plate, or lag screws (2.0, 2.4) can be lar and maxillary fractures. After temporary IMF, reduction and fixation of fragments within simpler fractures can be accomplished using 1.5 or 2.0 miniplates and lag screws and then bridging with a 2.4 duce large fragments of a comminuted : A lag screw and reconstruction plate used to provide fixation.
- 14. Comminuted fractures of the ascending mandibular ramus • In the case of concurrent fractures of the ascending ramus, a combined submandibular and preauricular approach may be warranted. • Simplify the fracture using 2.0 miniplates and subsequent bridging and then stabilize it with a 2.4 universal fracture plate or reconstruction plate. Com mandibular ramus and its reduction is seen in the image below. a : A comminuted fracture of the left ascending ramus. b : Reduction using miniplates of the superior aspect of the ascending ramus. c : Bridging of the comminuted area using a reconstruction plate. Comminuted fractures of the ascending mandibular ramus fractures of the ascending ramus, a combined submandibular and preauricular approach may be warranted. Simplify the fracture using 2.0 miniplates and subsequent bridging and then stabilize it with a 2.4 universal fracture plate or reconstruction plate. Comminuted fracture of the ascending mandibular ramus and its reduction is seen in the image below. : A comminuted fracture of the left ascending ramus. : Reduction using miniplates of the superior aspect of the ascending ramus. the comminuted area using a reconstruction plate. fractures of the ascending ramus, a combined submandibular and Simplify the fracture using 2.0 miniplates and subsequent bridging and then stabilize it with a 2.4 minuted fracture of the ascending : Reduction using miniplates of the superior aspect of the ascending ramus.
- 15. • Approach mandibular fractures methodically. Patients rarely die solely from mandibular fractures. Diagnose and treat in an efficient manner. • As with all trauma patients, strictly adhere to advanced trauma life support (ATLS) protocols. Particular attention to the airway is of critical importance to any patient with craniofacial trauma. • Use prophylactic antibiotics for compound fractures. Penicillin remains the antibiotic of choice. Evaluate nutritional needs. • The goal of treatment is to reestablish occlusion. Function is compromised with malunion. • The three separate techniques for rigid fixation of the mandible that have been developed are (1) the bicor?cal Luhr system, using vitallium plates, (2) system of stainless steel compression or reconstruc?on plates with bicor?cal screws, and (3) the Champy miniplate technique placed along the line of ideal osteosynthesis, using monocortical screws. • Perform intraoral surgery prior to an extraoral approach. IMF time varies according to type, location, number, and severity of fracture(s). • Generally, 6 weeks of IMF are prescribed, although this is only an empiric approximation. • Treat dental injuries concurrently with the fracture. Fractured teeth may become infected or jeopardize bone union and should be removed in consultation with a dentist. Mandibular cuspids help determine occlusion and should be preserved if possible. • Administer analgesic medications in the postoperative period. Administer antibiotic therapy covering gram-positive organisms to patients with open fractures. • Keep wire cutters at the bedside in case of emesis. Reevaluate nutritional needs. Preoperative Intraoperative Postoperative
- 16. • Maintain IMF for 4-6 weeks. Tighten wires every 2 weeks. • After wires are removed, a Panoramic radiograph is usually taken to ensure complete fracture union. • The most common complication is infection or osteomyelitis. • Malunion and nonunion of the mandible occur because of failure to observe treatment goals as previously outlined. • Contributing factors include oral sepsis, teeth in the fracture line, alcohol abuse and chronic disease, prolonged time prior to treatment, poor patient compliance, and displacement of fracture fragments. • In addition, plate fracture has been identified as a complication. • Both closed and open reductions of mandibular fractures cause favorable results for bony union. • In a study of 922 mandibular body and angle fractures that were repaired using an intraoral approach without IMF, solid bony union was achieved in more than 99% of pa?ents. Follow-up Complications Prognosis
- 17. SIGNS AND SYMPTOMS GeneralSpecific General Swelling Pain Drooling Tendernes Bony discontinuity Lacerations Bleeding from the mouth Ecchymosis Fractured, subluxe , luxated teeth Limitation in mouth opening Specific DENTO- ALVEOLAR THE BODY THE RAMUS SYMPHYSEALCONDYLAR CORONOIDTHE ANGLE BilateralUnilateral
- 18. DENTOALVEOLAR FRACTURES SIGNS AND SYMPTOMS • Lip bruises and laceration • Step deformity • Bony discontinuity • Fracture, luxation or subluxation of teeth • Laceration of the gingivae FRACTURE OF THE BODY SIGNS AND SYMPTOMS • Swelling • pain • Tenderness • Step deformity • Anaesthesia or paraesthesia of the lip • Intra oral hemorrhage SYMPHYSEAL/PARASYMPHYSEAL FRACTURES SIGNS AND SYMPTOMS • Tenderness • Sublingual haematoma • Loss of tongue control • soft tissue injury to the chin and lower lip FRACTURE OF THE RAMUS SIGNS AND SYMPTOMS • Swelling • Ecchymosis • Pain • Trismus
- 19. FRACTURE OF THE ANGLE SIGNS AND SYMPTOMS • Swelling • Posterior gag • Deranged occlusion • Anaesthesia or paraesthesia of lower lip • Haematoma • Step deformity behind the last molar tooth • Tenderness CORONOID FRACTURE SIGNS AND SYMPTOMS • Tenderness over the anterior part of the tragus • Haematoma • Painful limitation of movement • Protrusion of mandible may be present. UNILATERAL CONDYLAR FRACTURES SIGNS AND SYMPTOMS • Swelling over the TMJ • Hemorrhage from ear on the affected side • Battle’s sign • Locked mandible • Hollow over the condylar region after edema has subsided • rarely, Paraesthesia of lower lip • Deviation to the affected side upon opening • Painful limitation of movement BILATERAL CONDYLAR FRACTURES SIGNS AND SYMPTOMS • Same as above • Limitation in mouth opening • Restricted mandibular movement • Anterior open bite The End Good luck