Spinal TB in Non-Endemic Area
•
1 recomendación•842 vistas

- The patient presented with chronic back pain and MRI showed multiple osteolytic lesions in her spine. Biopsy of the lesions showed granulomatous inflammation but no malignancy. Cultures later grew Mycobacterium tuberculosis. - Vertebral tuberculosis must be considered even in non-endemic areas when evaluating osteolytic spinal lesions. Biopsy is essential for early diagnosis and proper treatment to avoid incorrect therapy. - The patient was likely diagnosed with reactivated latent tuberculosis despite having no symptoms of active disease previously.
Recomendados

Recomendados
Más contenido relacionado
La actualidad más candente
La actualidad más candente (20)
Similar a Spinal TB in Non-Endemic Area
Similar a Spinal TB in Non-Endemic Area (20)
Más de Bassel Ericsoussi, MD
Más de Bassel Ericsoussi, MD (20)
Último
Último (20)
Spinal TB in Non-Endemic Area
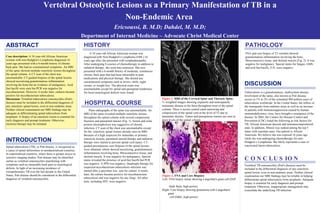
- 1. ABSTRACT Case description: A 54 year-old African American woman with non-Hodgkin's Lymphoma diagnosed 16 years ago presented with a 6-month history of chronic back pain. She had no constitutional symptoms. An MRI of the spine showed multiple osteolytic lesions throughout the spinal column. A CT scan of the chest was unremarkable. CT-guided biopsies of the spinal lesions showed necrotizing granulomatous inflammation involving the bone but no evidence of malignancy. Acid fast bacilli were seen but PCR was negative for mycobacterium. However, 6 weeks later, cultures became positive for mycobacterium tuberculosis. Discussion: Vertebral tuberculosis osteomyelitis (Pott's disease) must be included in the differential diagnosis of any osteolytic spinal lesion, even in non-endemic areas. Neither clinical examination nor MRI findings may be adequate in differentiating spinal tuberculosis from neoplasm. A biopsy of an osteolytic lesion is essential for early diagnosis and prompt treatment. Otherwise, incorrect therapy may be initiated. Vertebral Osteolytic Lesions as a Primary Manifestation of TB in a Non-Endemic Area Ericsoussi, B. M.D; Dahdel, M. M.D; Department of Internal Medicine – Advocate Christ Medical Center INTRODUCTION Spinal tuberculosis (TB), or Pott disease, is recognized as a cause of spinal deformities in unindustrialized countries. In industrialized countries, where there is greater access to sensitive imaging studies, Pott disease may be identified earlier as vertebral osteomyelitis manifesting with symptoms such as intractable back pain or neurological deficits. In light of an increasing incidence of extrapulmonary TB over the last decade in the United States, Pott disease should be considered in the differential diagnosis of vertebral osteomyelitis. HISTORY A 54 year-old African American woman was diagnosed with Non-Hodgkin's Lymphoma (NHL) 16 years ago after she presented with lymphadenopathy. After undergoing 8 courses of chemotherapy in addition to radiation therapy, she went into remission. She now presented with a 6-month history of moderate, continuous chronic back pain that had been intractable to pain medications and physical therapy. She denied any constitutional symptoms such as fevers, chills, night sweats, or weight loss. The physical exam was unremarkable except for spinal and paraspinal tenderness. No focal neurological deficits were found. Plain radiographs of the spine was unremarkable. An MRI of the spine revealed multiple osteolytic lesions throughout the spinal column with several compression fractures and paraspinal masses (Fig. 1). Serum and urine protein electrophoresis was suggestive of chronic infection. CT scan of the chest was unremarkable except for the osteolytic spinal lesions already seen on MRI. Because of a high suspicion for metastatic or primary osteolytic lesions, parenteral steroid therapy and radiation therapy were started to prevent spinal cord injury. CT-guided percutaneous core biopsies of the spinal lesions were obtained, which showed necrotizing, granulomatous inflammation involving bone, fibroconnective tissue, and skeletal muscle. It was negative for malignancy. Special stains revealed the presence of acid-fast bacilli but PCR was negative. A PPD was negative. Quadruple therapy for suspected mycobacterium tuberculosis infection was started after a specimen was sent for culture. 6 weeks later, the culture became positive for mycobacterium tuberculosis and was negative for any fungi. All other tests, including HIV, were negative. CONCLUSION Vertebral TB osteomyelitis (Pott's disease) must be included in the differential diagnosis of any osteolytic spinal lesion, even in non-endemic areas. Neither clinical examination nor MRI findings may be reliable in helping differentiate spinal tuberculosis from neoplasm. Adequate biopsy is essential for early diagnosis and prompt treatment. Otherwise, inappropriate management may exacerbate the underlying TB infection. DISCUSSION Tuberculosis is a granulomatous, multisystem disease. Involvment of the spine, also known as Pott disease, occurs in 1% to 2% of the estimated 400 million cases of tuberculosis worldwide. In the United States, the inflow of the immigrants from endemic areas as well as an increase in patients with immunosuppression caused by human immunodeficiency virus, have brought a resurgence of the disease. In 2005, the Centers for Disease Control and Prevention (CDC) listed the following as risk factors for TB; African American descent and immunocompromized state. In addition, Illinois was ranked among the top 5 states with reported cases. Our patient is African American. We believe she was exposed 16 years ago while she was undergoing chemotherapy for non-Hodgkin’s Lymphoma. She likely represents a case of reactivated latent tuberculosis. Figure 1. MRI of the Cervical Spine and Thoracic Spine : T 2 -weighted images showing expansile and nonexpansile metastatic disease to the bone throughout most of the spinal column. There is severe central canal narrowing and compression of the spinal cord at the level of T5 due to metastatic disease. Tumor and paraspinous masses are seen at most levels of the spinal column. Figure 2. FNA and Core Biopsies Left: FNA biopsy smear showing Langerhan's giant cell (Diff Quik Stain, high power) Right: Core biopsy showing granuloma with Langerhan's giant cell (H&E, high power) HOSPITAL COURSE FNA and core biopsy of T3 vertebra showed granulomatous inflammation involving the bone, fibroconnective tissue, and skeletal muscle (Fig. 2). It was negative for malignancy. Special stains for fungus, GMS, and acid fast bacilli, Z-N, were negative PATHOLOGY