Value of Medication Adherence in Chronic Vascular Disease
•
1 like•300 views

1) The study examined the relationship between medication adherence and health services utilization and costs for patients with congestive heart failure, hypertension, diabetes, and dyslipidemia using insurance claims data. 2) The results showed that medication adherence was associated with fewer hospitalizations and emergency department visits, more outpatient doctor visits, and higher pharmacy costs that were offset by lower medical costs. 3) Adherence led to annual total healthcare savings of $7,823 for heart failure, $3,908 for hypertension, $3,756 for diabetes, and $1,258 for dyslipidemia, with benefit-cost ratios ranging from 2:1 to over 13:1 depending on the condition and patient age.
Recommended

Recommended
More Related Content
More from M. Christopher Roebuck
More from M. Christopher Roebuck (9)
Recently uploaded
Recently uploaded (20)
Value of Medication Adherence in Chronic Vascular Disease
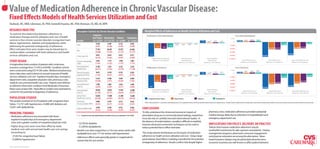
- 1. Value of Medication Adherence in Chronic Vascular Disease: Fixed Effects Models of Health Services Utilization and Cost Roebuck, MC, MBA; Liberman, JN, PhD; Gemmill-Toyama, MC, PhD; Brennan, TA, MD, JD, MPH RESEARCH OBJECTIVE Descriptive Statistics by Chronic Vascular Condition Marginal Effects of Adherence on Health Services Utilization and Cost To examine the relationship between adherence to Congestive medication therapy and the utilization and cost of health Utilization (All Individuals) Cost (All Individuals) Heart Failure Hypertension Diabetes Dyslipidemia 2 $2,000 services in four chronic vascular disorders (congestive heart Variable (n = 16,353) (n = 112,757) (n = 42,080) (n = 53,041) 1 ns 0.35 0.27 $1,058 $429 $656 $601 1.13 0.04 $0 failure, hypertension, diabetes and dyslipidemia); while 0.550 0.487 0.532 0.502 0 -0.03 -0.02 -0.01 ($1,860) ($1,258) Male -0.04 ($2,000) addressing the potential endogeneity of adherence. (0.497) (0.500) (0.499) (0.500) -1 -2.14 -2.39 -1.78 ($3,908) ($3,756) -2 ($4,337) ($4,413) Effect estimates from prior studies may be biased due to Age 77.301 68.401 67.872 65.096 -3 ($4,000) unobservables correlated with both adherence and health (10.600) (13.692) (13.745) (14.157) -4 ($6,000) ($7,823) services utilization and cost. Senior (age≥65) 0.872 0.614 0.615 0.517 -5 -5.72 ($8,000) ($8,881) (0.334) (0.487) (0.487) (0.500) -6 Annual Inpatient Hospital Days Annual Emergency Annual Outpatient ($10,000) STUDY DESIGN Charlson Comorbidity 2.025 1.112 1.696 1.001 (Adherent vs. Non-Adherent) Department Visits (Adherent vs. Non-Adherent) Physician Visits (Adherent vs. Non-Adherent) Annual Pharmacy Costs (Adherent vs. Non-Adherent) Annual Medical Costs (Adherent vs. Non-Adherent) Annual Total Health Care Costs (Adherent vs. Non-Adherent) Index (1.365) (1.222) (1.179) (1.173) A longitudinal claims analysis of patients with continuous insurance coverage from 1/1/05 to 6/30/08. Condition cohorts Annual Inpatient 11.901 3.291 4.255 2.239 Cost (Seniors) Hospital Days Utilization (Seniors) (26.973) (13.967) (16.458) (11.148) were constructed using ICD-9-CM codes. Medical and pharmacy 2 $2,000 $467 $676 $655 Annual Emergency 0.613 0.318 0.353 0.265 1 ns 0.45 0.37 $1,040 claims data were used to derive six annual measures of health Department Visits (1.156) (0.827) (0.891) (0.745) 0 1.22 0.01 $0 ns -0.02 -0.01 ($1,847) services utilization and cost: inpatient hospital days, emergency -1 -1.88 -0.01 -0.05 ($2,000) ($2,502) Annual Outpatient 11.651 8.506 9.407 8.660 department visits, outpatient physician visits, pharmacy costs, Physician Visits (10.306) (7.811) (8.458) (7.836) -2 -3.14 -3.41 ($4,000) ($5,170) -3 medical costs and total health care costs. Patients were defined -4 ($6,000) ($6,292) ($5,847) ($5,824) Annual Pharmacy 3,780 2,867 3,624 2,920 as adherent where their condition-level Medication Possession Costs ($) (4,493) (3,901) (4,371) (4,078) -5 -5.87 ($8,000) ($7,893) ($8,934) Ratios were at least 0.80. Fixed effects models were estimated to 39,076 14,813 17,955 12,688 -6 Annual Inpatient Hospital Days Annual Emergency Annual Outpatient Annual Medical ($10,000) Annual Pharmacy Costs Annual Medical Costs Annual Total Health Care Costs control for the potential endogeneity of adherence. Costs ($) (81,569) (42,371) (50,042) (39,477) (Adherent vs. Non-Adherent) Department Visits Physician Visits (Adherent vs. Non-Adherent) (Adherent vs. Non-Adherent) (Adherent vs. Non-Adherent) (Adherent vs. Non-Adherent) (Adherent vs. Non-Adherent) Annual Total 42,856 17,680 21,580 15,608 POPULATION STUDIED Health Care Costs ($) (82,058) (43,047) (50,753) (40,256) Congestive Heart Failure Hypertension Diabetes Dyslipidemia The sample consisted of 16,353 patients with congestive heart Medication 0.400 0.591 0.513 0.522 Notes: Unless denoted with “ns”, presented are statistically signi cant (p<0.01) marginal e ect estimates from linear xed e ects models of health services utilization and cost. All models included a weighted Charlson Comorbidity Index; two year indicator variables; dummy variables for senior, male, and adherent; and interaction terms for adherent with male and senior. failure, 112,757 with hypertension, 42,080 with diabetes and Possession Ratio (MPR) (0.435) (0.417) (0.426) (0.427) 53,041 with dyslipidemia. Adherent (MPR≥0.80) 0.340 (0.474) 0.505 (0.500) 0.412 (0.492) 0.426 (0.495) CONCLUSIONS To fully understand the clinical and economic impacts of pharmacy costs, medication adherence provided substantial PRINCIPAL FINDINGS medical savings, likely due to reductions in hospitalization and • Medication adherence was associated with fewer Notes: Presented are means with standard deviations in parentheses for last year of study period (7/1/07-6/30/08). prescription drug use in community-based settings, researchers must also rely on carefully executed observational studies. In emergency department use. inpatient hospital days and emergency department visits, and a greater number of outpatient physician visits the absence of randomization, causality is difficult to establish, - $3,756 for diabetes however advanced econometric techniques can be used to IMPLICATIONS FOR POLICY, DELIVERY, OR PRACTICE • Higher drug costs were more than offset by lower - $1,258 for dyslipidemia Policies that improve medication adherence may be reduce potential bias in effect estimates. medical costs with annual total health care cost savings • Benefit-cost ratios ranged from 2:1 for non-senior adults with worthwhile investments for plan sponsors and patients. Disease amounting to: dyslipidemia to over 13:1 for seniors with hypertension This study extends the literature on the impact of medication management programs, pharmacist-consumer engagement, - $7,823 for congestive heart failure adherence on health services utilization and cost. Using a large and physician education are among the alternatives. Value- • Adherence effects were generally greater in magnitude for - $3,908 for hypertension panel dataset, fixed effects modeling controlled for the potential based insurance designs may be particularly attractive since seniors than for non-seniors endogeneity of adherence. Results confirm that despite higher economic incentives are well-known to affect patient behavior. ©2010 Caremark. All rights reserved.