Chapter 3 Lower Respiratory Tract Infections
•Descargar como DOCX, PDF•
6 recomendaciones•4,152 vistas


Recomendados
Más contenido relacionado
La actualidad más candente
La actualidad más candente (20)
Destacado
Destacado (20)
Similar a Chapter 3 Lower Respiratory Tract Infections
Similar a Chapter 3 Lower Respiratory Tract Infections (20)
Más de Deep Deep
Más de Deep Deep (20)
Último
Último (20)
Chapter 3 Lower Respiratory Tract Infections
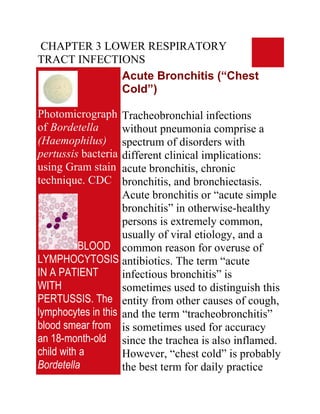
- 1. CHAPTER 3 LOWER RESPIRATORY TRACT INFECTIONS Acute Bronchitis (“Chest Cold”) Photomicrograph Tracheobronchial infections of Bordetella without pneumonia comprise a (Haemophilus) spectrum of disorders with pertussis bacteria different clinical implications: using Gram stain acute bronchitis, chronic technique. CDC bronchitis, and bronchiectasis. Acute bronchitis or “acute simple bronchitis” in otherwise-healthy persons is extremely common, usually of viral etiology, and a BLOOD common reason for overuse of LYMPHOCYTOSIS antibiotics. The term “acute IN A PATIENT infectious bronchitis” is WITH sometimes used to distinguish this PERTUSSIS. The entity from other causes of cough, lymphocytes in this and the term “tracheobronchitis” blood smear from is sometimes used for accuracy an 18-month-old since the trachea is also inflamed. child with a However, “chest cold” is probably Bordetella the best term for daily practice
- 2. pertussis infection since it implies that antibiotics are have lobulated seldom necessary. Bordetella nuclei. pertussis, the agent of whooping Lymphocytosis is cough, is now recognized as a characteristic of cause of acute bronchitis in adults. this disorder and Infection by either Mycoplasma the lymphocyte pneumoniae or Chlamydia morphology is pneumoniae accounts for many of often atypical. The the stubborn cases in which cytology of the symptoms fail to resolve or recur cells could be soon after treatment has been mistaken for discontinued. neoplastic lymphocytes. Infection of the tracheobronchial (Wright-Giemsa mucosa causes local stain) © The Johns inflammation, increased secretion Hopkins Autopsy of mucus, and damage to ciliated Resource (JHAR). cells. Symptoms result both from Image Archive. the inflammatory response and also from the interruption of the mucociliary blanket that normally cleanses the lower respiratory tract. Most cases of acute bronchitis (95% by some estimates) are caused by viruses.
- 3. All of the common viruses affecting the upper respiratory tract have been implicated: rhinoviruses, coronavirus, respiratory syncytial virus, adenoviruses, coxsackieviruses, influenza viruses A and B, and parainfluenza virus. In 2 studies in which attempts were made to establish a precise diagnosis, the etiology was established in only 16% and 29% of cases with viruses being the most common causes. Mycoplasma pneumoniae and Chlamydia pneumoniae probably play minor roles in this illness, at least in most populations. However, M. pneumoniae probably causes more cases of bronchitis than pneumonia, and C. pneumoniae may be an important cause of acute bronchitis in college-aged students. Whether S.
- 4. pneumoniae, H. influenzae, and M. catarrahalis cause chest cold in otherwise-healthy persons is unclear, but there is little support for the concept of quot;acute bacterial bronchitisquot; as a community- acquired disease. Recently it has been emphasized that Bordetella pertussis can infect adults, even when vaccinated, providing a reservoir for causing whooping cough among infants. Bordetella parapertussis causes a protracted illness similar to whooping cough but without systemic toxicity. Whether these observations can be generalized to other populations is undetermined. The onset is typically preceded by a prodrome of at least 24 hours with symptoms of coryza and pharyngitis. A dry cough, signifying early inflammation of the upper airway, often evolves
- 5. into a cough productive of moderate amounts of mucopurulent sputum. Fever, headache, myalgias, and retrosternal chest pain or discomfort may be present. Fever is most common when an influenza virus or Mycoplasma pneumoniae is the causative agent. The patient rarely looks toxic. Tracheal tenderness is often present. Auscultation may reveal a few coarse crackles with occasional wheezes in the chest, but there are no signs of consolidation. Transmission electron photomicrograph of a hamster trachea ring infected with M. pneumoniae. Note the orientation of the mycoplasmas through their specialized tip-like organelle, which permits close association with the
- 6. respiratory epithelium. M, mycoplasma; m, microvillus; C, cilia. Both images used with permission. From Baseman and Tully, Emerging Infection Diseases 3 Acute Infectious Exacerbations of Chronic Bronchitis Figure Chronic bronchitis is defined by Chlamydial the American Thoracic Society inclusions © (ATS) as excessive sputum Bristol Biomedical production with cough, present on Archive. Used with most days for at least 3 months a permission year and not less than 2 successive years, without an underlying etiology such as tuberculosis or Figure bronchiectasis. This common Chlamydial disorder, affecting up to 25% of inclusions in an the adult population, can lead to endothelial cell © full-blown chronic obstructive Bristol Biomedical pulmonary disease (COPD), the Archive. Used with fourth-leading cause of death in permission the United States. The extent to
- 7. which acute exacerbations are due to treatable infections remains controversial. Chronic bronchitis is caused mainly by cigarette smoking. Air pollution, cold and damp climates, heredity, frequent lower respiratory tract infections, and immunodeficiency disorders (such as common variable hypogammaglobulinemia or isolated IgA deficiency) play a role in some patients. The essential feature is anatomic change in the larger airways, including an increased number of mucus-producing goblet cells and mucosal gland hypertrophy in the bronchial walls. Increased bronchial secretions and impaired ability to handle them lead to chronic cough and disabling complications.
- 8. Current opinion holds that most acute exacerbations of chronic bronchitis are caused by viruses or by non-infectious agents. Viruses have been found in as few as 7% to as many as 64% of cases in which they were sought. By conservative estimate viruses cause about one-third of cases, the more common ones being influenza viruses A and B, parainfluenza virus, coronaviruses, and rhinoviruses. Cultures of sputum often show non-typable strains of Haemophilus influenzae, Streptococcus pneumoniae, and/or Moraxella catarrhalis. However, the extent to which these bacteria explain exacerbations in a given patient is hard to determine since they often colonize the damaged lower respiratory tract on a more- or-less permanent basis. Evidence suggests that repeated episodes of
- 9. bacterial infections—especially when caused by H. influenzae— contribute to deterioration of pulmonary function. S. aureus and aerobic gram-negative rods occasionally cause exacerbations of chronic bronchitis. The pathogens associated with quot;atypical pneumoniaquot; such as M. pneumoniae, C. pneumoniae, and L. pneumophila probably cause fewer than 10% of exacerbations. Evidence to date suggests that Chlamydia pneumoniae is more strongly associated with the underlying chronic bronchitis than with its acute exacerbations. However, Chlamydia pneumoniae can cause a stubborn respiratory illness lasting several weeks or longer and tending to relapse after each course of antibiotics.
- 10. Bronchiectasis Bronchiectasis is an acquired Figure disorder characterized This PA x-ray anatomically by abnormal depicts dilatation of bronchi and atelectatic, and bronchioles and clinically by bronchiectatic chronic productive cough and changes in this child’s right frequent lower respiratory tract infections. Its prevalence fell upper pulmonary dramatically after the introduction lung field. of broad-spectrum antibiotics and Atelectasis (a widespread immunization against collapse of the measles and pertussis. Although lung) can be due bronchiectasis is now uncommon, to bronchiectasis it often goes undiagnosed until (an enlargement far-advanced. Newer imaging of the bronchial studies now enable earlier tubes) and a diagnosis, and our understanding decrease in the of its causes continues to improve. effectiveness of their ciliated Cigarette smoking, the major mucosal lining, cause of chronic bronchitis, plays which renders little role in bronchiectasis except the lungs unable
- 11. to clear for predisposing to recurrent themselves of infections. The basic problem in clogging mucous bronchiectasis is permanent build-up. structural damage to the walls of CDC/ Dr. bronchi and bronchioles brought Thomas Hooten about by the concerted action of (1) infection and (2) impairment of the pulmonary toilet, airway obstruction, and/or a defect in host defenses. In the past, bronchiectasis was associated especially with frequent or severe lower respiratory infections during childhood. Bronchiectasis continues to be associated with such infections - especially necrotizing pneumonias in which treatment is delayed - but the list of known causes has expanded. Bronchiectasis can be the earliest clue to cystic fibrosis presenting during adolescence or early adulthood. Staphylococcus
- 12. aureus, Pseudomonas aeruginosa, and Pseudomonas cepacia are often isolated from these patients. Mycobacterium avium- intracelluare complex (MAC) infection is not infrequently associated with bronchiectasis, especially in older women and/or thin women. Allergic bronchopulmonary aspergillosis often leads to bronchiectasis, which might be prevented by early recognition of this syndrome. Immunodeficiency disorders, both congenital (hypogammaglobulinemia) and acquired (AIDS) predispose to bronchiectasis. The dyskinetic cilia syndromes are sufficiently common (about 1 in every 20,000 to 60,000 persons) that a case is likely to occur in every medium- sized city. Patients with advanced bronchiectasis experience daily
- 13. cough productive of large amounts of mucopurulent, thick, tenacious sputum. However, most patients produce lesser amounts of sputum, at least during the early stages, and cough may be nonproductive (quot;dry bronchiectasisquot;) or even absent. Dyspnea and hemoptysis are common. Patients often give a history of repeated respiratory infections and sometimes give a history of recurrent pleuritic chest pain. Hard crackles are heard locally over the lung fields in about 70% of patients. Rhonchi and widespread expiratory wheezes are also common. Clubbing is present in only about 3% of patients. Plain chest x-rays (PA and lateral views) are usually abnormal.
- 14. Acute Community-acquired Pneumonia: Overview Figure Pneumonia accounts for an This AP chest x- estimated 45,000 deaths in the ray shows United States each year. It is the pneumonia of the 6th most common cause of death left lower lobe and the most common infectious with early cause of death. Since it is not a consolidation, reportable disease, the precise the etiology of incidence is unknown. Estimates which was suggest that 4 million cases occur unknown. each year, prompting 10 million Pneumonia can physician visits and 600,000 to 1.2 be caused by a million hospitalizations and variety of agents adding $23 billion to health care including costs. Data suggest a 28-fold bacteria, viruses, increased cost for managing the and disease on an inpatient basis mycoplasmas, ($7,517 versus $264 for outpatient among others. therapy). However, the mortality Pneumonia rate is 1% or less for patients remains an managed as outpatients versus important cause 14% to 25% for those admitted to of morbidity and the hospital. Physicians often
- 15. mortality in the overestimate the short-term United States as mortality risk, but erring toward both a primary, hospitalization is understandable and secondary given the potentially fatal nature infection. of the disease. CDC/Dr. Microorganisms can enter the Thomas Hooten lungs by aspiration, inhalation, or by way of the bloodstream (hematogenous pneumonia). Figure Aspiration of bacteria that have This colonized the oropharynx is by far anteroposterior the most common mechanism. x-ray reveals a Most humans aspirate small bilaterally amounts of oropharyngeal progressive secretions on a nightly basis. plague infection Microorganisms that are not involving both removed by the mucociliary lung fields. blanket are taken up and killed by The first signs of pulmonary alveolar macrophages, plague are fever, the last line of defense. This headache, process, called pulmonary weakness, and clearance, is impaired by viral rapidly respiratory infections, tobacco developing smoke, chronic lung disease, pneumonia with alcohol, and many other factors
- 16. shortness of associated with debilitating breath, chest diseases. One or more chronic pain, cough, and diseases are present in the sometimes majority of adult patients with bloody or watery pneumonia (58% to 89% of sputum, patients in various studies). eventually Alcoholism predisposes to progressing for 2 aspiration, but cigarette smoking - 4 days into is the main avoidable risk factor respiratory for community-acquired failure and pneumonia in adults. shock. CDC/Dr. Jack Inhalation of aerosolized particles Poland is an important route of entry for many viruses including the influenza viruses and, most recently, the Hantaviruses. Bacteria that cause pneumonia by airborne transmission include M. tuberculosis, Yersinia pestis (plague), Bacillus anthracis (anthrax), and probably Legionella pneumophila (Legionnaire’s disease) and Francisella tularensis (tularemia).
- 17. Spore-producing fungi such as Histoplasma capsulatum, Blastomyces dermatitidis, and Coccidioides immitis also cause inhalation pneumonia. Hematogenous pneumonia classically develops from septic pulmonary emboli, frequently resulting in patchy or nodular bilateral pulmonary infiltrates sometimes accompanied by pleural effusions. In inner-city populations, a familiar scenario consists of bilateral pneumonia associated with S. aureus endocarditis on the tricuspid or pulmonic valves of injecting drug users. Another scenario consists of emboli from septic thrombophlebitis: for example, of the pelvic veins (pelvic inflammatory disease, septic abortion), internal jugular vein (the Lemierre syndrome) or any
- 18. large vein where a catheter has been inserted. Hematogenous seeding of the lungs possibly explains some pneumonias caused by gram-negative bacteria and by unusually virulent organisms such as F. tularensis (tularemia). The microbial cause of community-acquired pneumonia is usually difficult to determine. In prospective studies of patients requiring hospitalization, a cause is found in only 40% to 70% of cases. In primary care practice, a far greater fraction of cases are never diagnosed. Most of these cases respond to empiric therapy. Published data concerning the causes of pneumonia vary from one region to another, but some generalizations are possible. Mycoplasma pneumoniae has been determined to be the most common cause in some
- 19. communities, when presumptive diagnoses were taken into account, followed by Streptococcus pneumoniae and Chlamydia pneumoniae. Adults with compromised host defenses are likely to have pneumococcal pneumonia, but can also have pneumonia due to H. influenzae, Moraxella catarrhalis, S. aureus, or aerobic gram-negative rods. There is wide agreement that S. pneumoniae is the most common cause of community-acquired pneumonia requiring hospitalization. An emerging and controversial area concerns the frequency of pneumonia caused by more than one microorganism. In one study, a second pathogen was found in about 10% of patients with pneumonia due to a conventional bacterial pathogen, but in 55% of patients in whom an quot;atypicalquot; pathogen was found.
- 20. In 1938, the term quot;atypical pneumoniaquot; was introduced to describe quot;an unusual form of tracheobronchopneumonia with severe constitutional symptomsquot;. It later became customary to distinguish between quot;classical bacterial pneumoniaquot; and quot;atypical pneumoniaquot;. This distinction was challenged during the 1990s when researchers found it difficult if not impossible to differentiate these illnesses on clinical grounds. Some authorities now suggest abandoning the term quot;atypical pneumoniaquot;. Others keep the term since it enriches our appreciation of the disease, forces us to consider unusual etiologies, and reminds us that the quot;atypical pneumoniasquot; do not respond to β- lactam antibiotics. For these latter reasons and for the sake of clarity, we keep the terms here even while
- 21. agreeing that in some cases it may be impossible to distinguish between quot;classic bacterial pneumoniaquot; and quot;atypical pneumoniaquot; in actual clinical practice. quot;Typical pneumoniaquot; is an alveolar disease whereas quot;atypical pneumoniasquot; affects mainly the tracheobronchial mucosa and interstitium of the lung; hence, the different clinical manifestations. Classical bacterial pneumonia begins with sudden onset of fever, chills, pleuritic chest pain, and productive cough. In the absence of impaired consciousness or inebriation, patients usually seek medical care within 6 hours of the onset of symptoms. Chills occur in about 50% and chest pain in about 30% of patients. Most patients are febrile although some,
- 22. especially the elderly, may have normal or subnormal temperatures. The respiratory rate is usually increased. Physical examination often reveals signs of consolidation such as dullness to percussion, pectoriloquy, and egophony (e to a change). Lobar consolidation is present on chest x-ray in about one-third of patients. The white blood count is usually elevated with a shift-to- the-left. However, leukopenia rather than leukocytosis may be present and portends a poor prognosis. Atypical pneumonia, on the other hand, usually begins gradually. The insidious onset is often brought out by asking, quot;When was the last time you were in your usual good health?quot; Constitutional symptoms are usually more prominent than the pulmonary
- 23. symptoms. Chest pain is experienced as substernal discomfort. Cough is non- productive or productive of only scanty amounts of sputum. Relative bradycardia is frequently present. The trachea may be tender but the lung fields are essentially clear to auscultation, prompting one to be surprised by the extent of infiltrate present on chest x-ray. The white blood count is often normal or near normal. Modest elevation of liver enzymes (specifically, the aminotransferases - AST (SGOT) and ALT (SGPT) - is often present. Atypical pneumonia, in summary, seldom presents as an acute, life-threatening medical problem but forces the physician to expand the differential diagnosis. Pneumococcal Pneumonia
- 24. Streptococcus pneumoniae remains the major cause of severe community-acquired pneumonia and, worldwide, a leading cause of death. It accounts for about two- thirds of cases of bacteremic pneumonia, and is the most common cause of pneumonia leading to hospitalization in all age groups. Some authorities believe that S. pneumoniae may cause up to one-half of all community-acquired pneumonias. There is concern that the incidence of pneumococcal disease may be increasing at the same time that drug resistance is becoming much more common. Primary care clinicians should strive to make pneumococcal vaccination an imperative for patients at increased risk. S. pneumoniae is a common
- 25. colonizer of the nasopharynx. Invasive pneumococcal disease occurs most often after a new serotype has been acquired, typically after an incubation of one to three days. Viral illness increases the incidence of disease presumably by interfering with normal host defenses. Risk factors for invasive pneumococcal disease include extremes of age, alcoholism, HIV disease, end- stage renal disease, sickle cell disease, diabetes mellitus, dementia, malnutrition, malignancies, diseases affecting B lymphocyte function (notably, multiple myeloma and hypogammaglobulinemia), and immunosuppressive disorders. Patients with asplenia are susceptible to fulminant pneumococcal disease. The pneumococcus does not invade cells as readily as do some of the
- 26. other streptococci. However once in the lungs, it passes easily from one alveolus to another through the pores of hence the basis Cohn until stopped by the dense connective tissue of a fissure for lobar consolidation. As classically described by previous generations of clinicians, S. pneumoniae causes a lobar pneumonia with by the sudden onset of fever with a single, hard- shaking chill, cough productive of rusty-colored mucopurulent sputum, and pleuritic chest pain. The patient presents with systemic toxicity including tachypnea. Physical examination reveals crepitant râles, tubular breath sounds, and signs of lobar consolidation (dullness to percussion, egophony with e to a change, and pectoriloquy). Today, however, pneumococcal disease is
- 27. often a more subtle illness. Patchy infiltrates and bronchopneumonia are relatively common. It is often difficult to say precisely what represents pneumococcal pneumonia and what does not unless blood cultures are positive. Bacterial Pneumonia due to Agents other than S. pneumoniae Figure Haemophilus Among the numerous bacteria influenzae as other than S. pneumoniae that seen using a sometimes cause acute Gram-stain community-acquired pneumonia, technique. the most common are H. During the flu influenzae, S. aureus, outbreak of 1918 Streptococcus pyogenes, H. influenzae miscellaneous aerobic gram- was termed negative rods, and anaerobic Pfeiffer's quot;mouth floraquot; bacteria. Patients Bacillus, where it with these pneumonias often have was found in the significant underlying disease, sputum of many severe pneumonia, or both. influenza
- 28. patients, and Therefore, hospitalization is thought to be the usually indicated. cause of influenza. H. influenzae is a frequent cause CDC of pneumonia in elderly patients and in patients with serious underlying diseases including chronic obstructive lung disease. The pneumonia usually has a patchy or segmental distribution characteristic of bronchopneumonia as opposed to lobar pneumonia. A sputum Gram’s stain showing small, pleomorphic gram-negative coccobacilli can be virtually diagnostic. Staphylococcus aureus pneumonia, when community- acquired, tends to be an acute, fulminant about 1% of cases, except during influenza epidemics. Influenza virus infection markedly predisposes to
- 29. staphylococcal colonization of the respiratory mucosa. Staphylococcal pneumonia tends to be a necrotizing process with abscess formation. The chest x-ray sometimes shows air pockets known as pneumatoceles, especially in children. Streptococcus pyogenes (group A streptococcal) pneumonia is also uncommon except during influenza epidemics. This pneumonia is often accompanied by the rapid development of large empyemas. Chest tube drainage is often necessary, resulting in prolonged hospitalization. Klebsiella pneumoniae is a relatively common cause of pneumonia in patients suffering from alcoholism. The pneumonia often assumes a lobar distribution. Classically, this pneumonia
- 30. affects the upper lobes and causes a “bulging fissure” on chest x-ray. E. coli and other aerobic gram- negative rods are relatively common causes of pneumonia in the frail elderly. Pseudomonas aeruginosa, although a common cause of nosocomial pneumonia, is rarely associated with community-acquired pneumonia in patients without underlying lung disease or severe debility. Pneumonia due to quot;mouth floraquot; bacteria - by which is meant a combination of anaerobic and aerobic bacteria with the anaerobes usually predominating - occurs most frequently in patients suffering from alcoholism and poor oral hygiene and results from aspiration. The sputum is usually copious and often foul smelling. quot;Mouth floraquot; pneumonia in an edentulous patient should prompt
- 31. suspicion of underlying lung cancer. A foul odor to the breath is present in many but not all of these patients. This form of pneumonia is often associated with lung abscess and with empyema due to bronchopleural fistula. Mycoplasma pneumoniae pneumonia Formerly known as the quot;Eaton agentquot;, Mycoplasma pneumoniae is the most commonly identified cause of atypical pneumonia although its precise incidence is unknown. Various investigators have determined this microorganism to be the cause of 13% to 27% of community- acquired pneumonias. It can also cause hospital-acquired pneumonias, and it has caused as many as 50% of pneumonias
- 32. during epidemics in closed populations. Mycoplasma pneumoniae pneumonia becomes less common after age 40, but older persons may experience more severe manifestations. M. pneumoniae is a cell-wall- deficient organism with particular affinity for the respiratory tract epithelium. Many of the disease manifestations are now thought to be immune-mediated. Close, prolonged contact promotes transmission by respiratory secretions. There is currently interest in the extent to which M. pneumoniae accompanies other agents as a co-pathogen. In one study, an additional pathogen was found in about two-thirds of patients with M. pneumoniae pneumonia who required hospitalization; S. pneumoniae was most commonly found, but
- 33. Legionella species and Chlamydia pneumoniae were also identified. It is estimated that of persons infected with M. pneumoniae, about 20% are symptomatic, about 70% develop a mild respiratory illness (pharyngitis and/or tracheobronchitis), and fewer than 10% develop pneumonia. The disease occurs in all age groups including toddlers and the elderly but peaks between ages 5 to 15 years. After an incubation period of about 3 weeks, symptoms begin gradually with fever, headache, malaise, chills, sore throat, substernal productive, and cough. The cough is initially non- productive, paroxysmal, and worse at night. It commonly becomes productive later in the illness. Physical examination is
- 34. usually unimpressive. Bullous myringitis (inflammation of the tympanic membrane with bullae) is uncommon, occurring at most in about 5% of patients, but has a high positive predictive value for M. pneumoniae infection. More commonly there is mild tenderness over the paranasal sinuses, mild erythema of the posterior pharyngeal mucosa, soft cervical lymphadenopathy, and tracheal tenderness. Scattered râles and wheezes may be present but are usually unimpressive. The white blood count is normal in 75% or more of cases. Thrombocytosis can occur as an acute-phase response. Liver enzymes, notably the aminotransferases (AST and ALT), are often mildly elevated. The chest x-ray commonly shows infiltrates that are much more
- 35. extensive than one would have suspected from physical examination. The most common pattern is a peribronchial pneumonia in which thickened bronchial shadows are surrounded by streaky interstitial infiltrates and patchy atelectasis. Other patterns include nodular infiltrates and hilar lymphadenopathy. The lower lobes are most commonly involved, and pleural effusions - which can be especially severe in patients with sickle cell disease - occur in up to 20% of patients when carefully sought. Extrapulmonary manifestations of M. pneumoniae pneumonia sometimes dominate the clinical picture and include hemolytic anemia, rashes including the life- threatening Stevens-Johnson syndrome, central nervous system complications (about 0.1% of
- 36. patients, especially children), cardiac complications, and polyarthritis. Chlamydia pneumoniae pneumonia Chlamydia pneumoniae, described in 1986 as the TWAR agent, has been determined by some researchers to be the third or fourth most common cause of community-acquired pneumonia, explaining perhaps 10% to 14% of cases (up to 28% in some series). Pneumonia is recognized most frequently among the elderly, in whom it can be severe. Chlamydia pneumoniae is classified as a bacterium on the basis of its cell wall and growth properties. Unlike most bacteria, however, it grows only as an intracellular parasite. Serologic
- 37. studies suggest that most humans gain experience with C. pneumoniae at some point in their lives, although immunity is short- lived. About 50% of all persons have antibodies by age 20, and up to 75% of elderly persons are seropositive. It is also thought that most infections (up to 90%) are asymptomatic. Transmission is probably person-to-person by respiratory secretions. After an incubation period of several weeks, most patients experience gradual onset of non- specific upper and lower respiratory symptoms including those of sinusitis, otitis, and pharyngitis. Sore throat with hoarseness is often prominent among the initial symptoms and tends to be the dominant symptom in college-aged persons. Symptoms of pneumonia tend to
- 38. develop slowly. Often, patients have experienced symptoms for several weeks before seeking medical care. The history sometimes suggests a biphasic illness, as follows: (1) upper respiratory infection with sore throat that resolved, then (2) lower respiratory infection with cough. The severity is age-dependent. Children under age 5 seldom have evidence of significant disease. University students often present with a 10-day history of sore throat or hoarseness with minimal fever. The mean age of patients with pneumonia is about 56 years. Ronchi and râles are present on physical examination more frequently than in M. pneumoniae pneumonia, even among patients who do not complain of cough. The white blood count is usually normal. Chest x-ray may show
- 39. one or more infiltrates, the most common finding being a single, patchy, subsegmental infiltrate. Wheezing is sometimes present. Accumulating evidence suggests that C. pneumoniae sometimes precipitates adult-onset asthma. Reported extrapulmonary manifestations of C. pneumoniae infection include meningoencephalitis, cerebellar dysfunction, Guillain-Barré syndrome, reactive arthritis, and myocarditis. The possibility that C. pneumoniae might cause coronary artery disease has received much attention. High antibodies to C. pneumoniae have been observed in patients with chronic obstructive lung disease, sarcoidosis, and lung cancer but an etiologic link is unclear. Chlamydia psittaci
- 40. (Psittacosis; Ornithosis) About 100 to 200 cases of psittacosis are reported in the U.S. each year, but the true incidence is thought to be much higher. Mortality can be high if the diagnosis is not suspected. Chlamydia psittaci infects many and perhaps all species of birds, which may remain asymptomatic or show symptoms and signs of illness such as anorexia, dyspnea, and ruffled feathers. Strains of C. psittaci that are most virulent for humans tend to be those associated with psittacine birds (from the Latin psittacus, or parrot), such as parrots, parakeets, macaws, cockatoos, and budgerigars, and also with turkeys. Humans who develop psittacosis are commonly bird fanciers or work in poultry farms
- 41. (notably, turkey farms), abattoirs, processing plans, pet shops, or veterinarians’ offices. The organism is usually acquired by inhalation, but human-to-human transmission occurs on rare occasions. After an incubation period of 5 to 15 days, patients develop symptoms and signs of illness ranging in severity from mild to life threatening. Atypical pneumonia, the most characteristic form of the disease, is manifest by headache, fever, and non-productive cough. Chest x-ray is usually abnormal (75%) of cases, most commonly showing consolidation of one lower lobe. The radiographic findings are usually much more striking than the findings on auscultation of the chest. Psittacosis can also present as a typhoidal illness (fever,
- 42. malaise, relative bradycardia, hepatosplenomegaly), a non- specific flu-like quot;viral syndromequot;, a mononucleosis-like syndrome, or as fever of unknown origin. Legionnaire’s disease Figure First identified in 1976 during an This micrograph outbreak at an American Legion of a biopsied Convention in Philadelphia, lung tissue Legionnaire’s disease is now specimen stained recognized as a relatively with the CDC's common cause of both modified community-acquired and hospital- Dieterle silver acquired pneumonia. The impregnation incidence exhibits wide procedure, geographic variation - from less revealed small, than 1% to more than 16% of blunt, community-acquired pneumonias pleomorphic - reflecting to a large extent the intracellular, and degree of contamination of water extracellular reservoirs by the causative bacilli, which organisms. Unlike pneumonias stain brown to due to M. pneumoniae and C.
- 43. black against a pneumoniae, cases that can be pale yellow treated on an outpatient basis tend background; to be the exception rather than the Mag. 500x. rule. Dieterle’s stain is a preparation Legionella species are gram- used when negative bacteria that stain poorly and survive intracellularly. More Legionella than 40 species, and more than 60 pneumophila bacteria are serogroups, of Legionella are now suspected. recognized. Legionella Uranyl nitrate is pneumophila is the most applied in order commonly encountered species, to first sensitize causing at least 80% of clinical the slide mount, infections. which is subsequently Legionellosis seems to be a treated with gum disease of human progress mastic, followed brought about by devices that by an incubation maintain water at warm period, after temperatures and produce which the slide is aerosols. In water, the organisms soaked in silver multiply within amebas; in nitrate. Lastly, humans they multiply within the slide is alveolar macrophages. The
- 44. “developed” in a disease is spread by water rather hydroquinone, than by person-to-person contact. sodium sulfite, Contamination of water sources acetone, has been associated with formaldehyde, numerous outbreaks in settings pyridine, and ranging from inner-city hospitals gum mastic bath. to luxury cruise liners. The Legionella Clinically severe cases of pneumophila Legionnaire’s disease tend to bacteria, if present, will occur in persons with stain black. CDCcompromised host defenses, most often in the setting of chronic obstructive pulmonary disease, Figure immunosuppression, or advanced age. A mild form of Legionellosis, This silver- known as Pontiac fever, is a self- stained micrograph of a limited disease presenting as fever, malaise, headaches, and lung tissue chills without pneumonia. Pontiac specimen fever resolves within a few days revealed the without antibiotic therapy. presence of Legionnaire’s disease, the more Legionella familiar and more severe form of pneumophila Legionellosis, affects persons of bacteria. The
- 45. specimen was all ages and presents with taken from a symptoms that overlap those of victim of the quot;classic bacterialquot; and quot;atypicalquot; 1976 pneumonia. Legionnaires’ disease outbreak After an incubation period of 2 to in Philadelphia. 10 days, patients experience the CDC onset of fever, headache, anorexia, malaise, and myalgia. At this point, respiratory symptoms are usually not prominent, the cough Figure being only minimally productive. Legionella Some patients have chest pain pneumophila and, if the sputum is blood-tinged, multiplying pulmonary embolism is often inside a cultured suspected. Gastrointestinal human lung symptoms with nausea, vomiting, fibroblast diarrhea, and abdominal pain can CDC also dominate the clinical picture. Alternatively, neurologic Figure symptoms can be the presenting Anteroposterior complaint, variably manifested as headache, lethargy, and change in x-ray reveals mental status. bilateral pulmonary
- 46. infiltrates in a Fever is usually present. Relative patient with bradycardia is found more often in Legionnaires' older patients and in those with disease CDC severe pneumonia. Examination of the chest usually shows râles and, later in the illness, signs of consolidation. The peripheral blood commonly shows leukocytosis and thrombocytopenia. Hyponatremia (serum sodium < 130 mEq/L) is more common in Legionnaire’s disease than in most other pneumonias. Hypophosphatemia also occurs. There is frequently evidence of liver and renal dysfunction. Hematuria and proteinuria are common. There is no characteristic feature on chest x-ray. The most common pattern is a patchy infiltrate involving one lobe, which progresses to consolidation. Infiltrates can assume a diffuse or interstitial pattern, and pleural effusions are
- 47. common.