anatomy of TMJ
•Download as PPTX, PDF•
94 likes•20,106 views

basic anatomy of TMJ. i hope this will help everyone

Recommended
More Related Content
What's hot
What's hot (20)
Similar to anatomy of TMJ
Similar to anatomy of TMJ (20)
Recently uploaded
Recently uploaded (20)
anatomy of TMJ
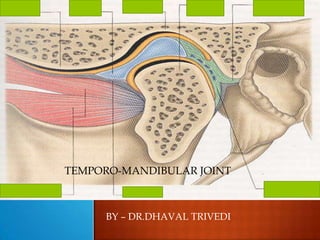
- 1. BY – DR.DHAVAL TRIVEDI TEMPORO-MANDIBULAR JOINT
- 2. Ginglymoid joint Diarthrodial joint Formed by 2 bones Compound joint only synovial joints with an articular disc
- 3. Condyles Articular surface of the temporal bone Capsule Articular disc Ligaments Lateral pterygoid
- 6. - The squamous portion of the temporal bone ( concave ) - Anterior : a convex bony prominence ( tubercle ) = articular eminence - Posterior : squamotympanic fissure anteromedial : petrosquamous fissure posteromedial : petrotympanic fissure
- 7. The posterior roof is thin , not designed to sustain heavy force in which condyle situated - The articular eminence consists of thick dense bone to tolerate such forces - The steepness of the articular eminence surface dictates the pathway of the condyle
- 8. - It is the posterior portion of the ramus mandibula that extends upward - Mediolateral : 15 – 20 mm Anteroposterior : 8 – 10 mm - Anterior view : medial and lateral poles, the medial pole generally more prominent - The actual articulating surface extends anteriorly and posteriorly to the most superior aspect ( P > A ) Lateral pole anterior to medial pole Articular surface: anterior superior aspect
- 9. Articular zone Proliferative zone Fibrocartilaginous zone Calcified cartilage zone Subarticular bone
- 10. The articular surface of the mandibular fossa and condyle are lined with dense fibrous connective tissue affords several advantages over hyaline cartilage : - less susceptible to the effects of aging - less likely to break down over time - a better ability to repair
- 12. The internal surface of the joint cavity are surrounded by specialized endothelial cells that form a synovial lining , produces synovial fluid So TMJ - a synovial joint The synovial fluid serves two purposes : 1. Acts as a medium for providing metabolic requirement, since the articular surfaces of the joint are nonvascular 2. As a lubricant during function Two mechanisms of the lubrication : 1. Boundary lubrication Prevents friction in the moving joint 2. Weeping lubrication Eliminates friction in the compressed but not moving joint
- 13. The articular eminence,which is present anterior to the glenoid fossa consists of a descending slope, transverse ridge that is a medial extension of the zygomatic tubercle, and an ascending slope. The eminence is covered by dense, compact, fibrous tissue that consists primarily of collagen with a few fine elastic fibers.
- 14. Origin: modified periosteum of intramembranous bone, NOT endochondral origin. A consequence of 2 embryonic tissue masses growing towards each other, NOT a single tissue mass cleft to form a joint articulation. Function: 1) load distribution 2) synovial lubrication Character: NOT hyaline cartilage, but fibrous in nature 1) avascular 2) NOT innervated 3) resistant to shear, tension forces 4) increased remodeling potential
- 15. These two bones are actually separated by an articular disc, which divides the TMJ into two distinct compartments. The inferior compartment allows for rotation of the condylar head around an instantaneous axis of rotation, corresponding to the first 20 mm or so of the opening of the mouth. After the mouth is open to this extent, the mouth can no longer open without the superior compartment of the TMJ becoming active.
- 17. Fibroelastic , highly vascular & innervated Attachments – Lateral aspect – zygomatic tubercle , lateral rim of glenoid fossa , postglenoid tubercle Lateral capsule continues medially and becomes less distinct anteriorly Medially – medial rim of glenoid fossa Close relation medially - spine of sphenoid , sphenomandibular ligament , middle meningeal artery
- 18. Posteriorly – petrotympanic fissure & fuses with superior stratum of the posterior bilaminar zone B/w posterior capsule and postglenoid tubercle – vascular body present , part of parotid gland Lateral capsule becomes thickened to form TM ligament Inferior – periosteum of the neck of the condyle
- 20. - Serves as a nonossified bone - Composed of dense fibrous connective tissue devoid of any blood vessels or nerve fibers - Sagittal plane can be divided into 3 regions according to thickness - anterior border - posterior border slightly thicker than anterior border - central area is the thinnest intermediate zone in which condyle is located normally
- 21. - Anterior view - the disc is generally thicker medially than laterally so increased space between the condyle and the articular fossa toward the medial of the joint - The precise shape of the disc depend on morphology of the condyle and mandibular fossa - During movement the disc is somewhat flexible and can adapt to the functional demands of the articular surface do not imply that morphology of the disc is reversibly altered during movement
- 25. - The articular disc is attached posteriorly to this region - It is a loose connective tissue region that highly vascularized and innervated - Superior : superior retrodiscal lamina ( contains many elastic fibers ) bilaminary zone It attaches the disc posteriorly to the tympanic plate - Inferior : inferior retrodiscal lamina ( composed chiefly collagenous fibers ) It attaches the inferior border of the posterior edge of the disc to the posterior margin of the articular surface of the condyle - The remaining body of the tissue is attached posteriorly to a large venous plexus , it fills with blood as the condyle moves forward
- 26. Anterior region of the disc is attached to the capsular ligament - Superior : anterior margin of the articular surface of the temporal bone Inferior : anterior margin of the articular surface of the condyle - Composed of collagenous fibers Anteriorly the disc is also attached by tendinous fibers to the superior lateral pterygoid muscle
- 28. Disc is attached to capsular ligament medially and laterally Divides the joint in 2 cavities Superior & inferior Endothelial cells that form a synovial lining surrounds the internal surfaces of the cavities – produces synovial fluid
- 29. 1) The collateral Ligaments, (2) The capsular ligament, and (3) The temporomandibular ligament. (4) The sphenomandibular, (5) Stylomandibular, (6) Discomalleolar (Pinto's) ligament
- 30. The collateral ligaments attach the medial and lateral borders of the articular disc to the poles of the condyle. They are commonly called the discal ligaments 1. The medial discal ligament attaches the medial edge of the disc to the medial pole of the condyle. 2. The lateral discal ligament attaches the lateral edge of the disc to the lateral pole of the condyle.
- 31. The discal ligaments are true ligaments, composed of collagenous connective tissue fibers; therefore they do not stretch. They function to restrict movement of the disc away from the condyle. In other words, they allow the disc to move passively with the condyle as it glides anteriorly and posteriorly on the articular surface of the condyle. Thus these ligaments are responsible for the hinging movement of the TMJ which occurs between the condyle and the articular disc.
- 32. The fibres of the capsular ligament are attached superiorly to the temporal bone along the borders of the articular surfaces of the mandibular fossa and articular eminence. Inferiorly the fibres of the capsular ligament attach to the neck of the condyle. The capsular ligament acts to resist any medial, lateral or inferior forces that tend to separate or dislocate the articular surfaces.
- 33. The lateral aspect of the capsular ligament is reinforced by strong tight fibres that make up the lateral ligament or the TM ligament. • An outer oblique portion Arising form outer surface of the articular eminence and extending backward and downward to insert into the outer surface of the condylar neck. • Inner horizontal portion with the same origin but inserting into lateral pole of the condyle and posterior part of the articular disc. • The oblique portion of the TM ligament resists excessive dropping of the condyle and therefore acts to limit the extent of mouth opening
- 34. Sphenomandibular ligament forms a broad impenetrable wall medial to mandibular foramen. It is one of the two TMJ accessory ligament. It arises from the spine of the sphenoid bone and extends downward to a small bony prominence on the medial surface of the ramus of the mandible called the lingula. It doesn’t have any significant limiting effect on the mandibular movement
- 35. The stylomandibular ligament arrises from the styloid process and extends downward and forward to the angle and posterior border of the ramus of the mandible. It becomes taut when the mandible is protruded, but is more relaxed when the mandible is opened. Therefore the stylomandibular ligament limits excessive protrusive movements of the mandible.
- 36. : The discomalleolar ligament ( Pinto's ligament) was described by Pinto (1962) as a connection between the malleus and the medial wall of the joint capsule. However, a separate ligament can be demonstrated here in only 29% of temporomandibular joints
- 37. Damage to structures within the middle ear during surgical manipulation of the temporomandibular joint (TMJ) has been reported. Two structures are proposed as possible intermediaries in this trauma: the discomalleolar ligament @ML), which passes from the malleus to the medial retrodiscal tissue of the TMJ,and the anterior malleolar ligament (AML), which connects the malleus with the lingula of the mandible via the sphenomandibular ligament (SML). It has been hypothesized that when tension is applied to the DML and/or AML, the resulting movement of the malleus could cause damage to the tympanic membrane and associated structures.
- 38. Trigeminal nerve Most innervation by auriculotemporal nerve Deep temporal Massetric
- 39. Superficial temporal – posterior Middle meningeal – anterior Internal maxillary – inferior Deep auricular Anterior tympanic Ascending pharyngeal The condyle receives supply through its marrow spaces by inferior alveolar artery and feeder vessels
- 40. Preauricular - Blair 1914 and Al-Kayat,Bamley 1979 Advantage Exposure of anterior portion of zygomatic arch Complications - Facial nerve paralysis, Paresthesia of auriculotemporal nerve, Salivary fistula, sialocele , Scarring , Frontal nerve injury
- 41. Postauricular - Alexander 1975 Adv- Avoid possible facial nerve injury, salivary fistula and formation of a sialocele, Minimal swelling ,Less discomfort Com - Stenosis of external auditory canal , Infection , Paresthesia (temporary or permanent) of the external pinna , Deformity of the auricle
- 42. Endaural - Rogetti 1954 Adv - Excellent access to the lateral and posterior aspect of TMJ , Good exposure of the anterior aspect of TMJ , Esthetics Com - Perichondrtis with esthetic compromise , (loss of tragal projection)
- 43. Perimeatal (preauricular + postauricular) - Eggleston6 1978 Adv - Access to glenoid fossa, No damage to frontal branch of facial nerve ,Avoid stenosis or infection of the cartilage Com - Poor access to the entire zygomatic arch , Difficult to extend the incision
- 44. Submandibular - Risdon 1934 Adv - Better access and visualization (in combination with preauricular) com - Possible injury to the marginal mandibular and cervical branches of facial nerve
- 45. Bicoronal - Pogrel 1991 Adv - Simultaneous access to both TMJs using one incision Superior approach , Good access , Enables harvesting of the temporalis m and fascia , Minimal chance of facial injury Com - Greater area for reflection, Time- consuming for pre-op preps , Compromised esthetic as hair shaving required, Temporary weakness of frontal nerve
- 46. The superficial temporal artery, the transverse facial artery, the auriculotemporal nerve, and the facial nerve (cranial nerve VII) are intimately involved in the surgical dissection to the TMJ. The superficial temporal artery, one of the terminal branches of the external carotid, begins behind the mandibular condylar neck deep to the parotid gland as it emerges from behind the parotid gland. It crosses over the posterior root of the zygomatic process of the temporal bone and enters the temporal region of the scalp.
- 47. The transverse facial artery arises from the base of the superficial temporal artery and runs almost transversely across the face, lying upon the outer surface of the masseter muscle about 1.5 cm below the zygomatic arch but above the parotid duct. The auriculotemporal nerve, a cutaneous sensory branch of the mandibular division of the trigeminal nerve , travels just posterior to the neck of the condyle at the inferior level of the capsule attachment. It travels upward across the root of the zygomatic arch just posterior to the superficial temporal artery, which it accompanies into the scalp.
- 48. The distance from the most anterior concavity of the bony external auditory canal to the most posterior significant temporal branch of the facial nerve was measured, with a mean of 2.0 * 0.5 cm and a range of 0.8 to 3.5 cm. The mean distance from the bifurcation of the main trunk of the facial nerve to the lowest concavity of the external auditory canal was 2.3 *0.28 cm, with a range of 1.5 to 2.8 cm. The mean distance from the bifurcation of the facial nerve to the postglenoid tubercle was 3.0 + 0.31 cm, with a range of 2.4 to 3.5 cm. Knowledge of the distances and the range of the facial nerve branches from fixed bony landmarks within the surgical field alerts the surgeon to the areas of highest risk.
- 50. To locate the facial nerve, an incision is made just in front of the tragus of the ear from the root of the zygoma to the angle of the jaw. Here the incision is carried forward about one finger breadth below the ramus of the mandible as far as is necessary to obtain adequate exposure. The incision is carried down through skin and subcutaneous tissue to the cartilage bounding the anterior extremity of the external auditory canal. Then, with blunt dissection, the cartilage of the external auditory canal is separated from the capsule of the parotid gland as far & medially as is possible or until a firm bony resistance is met. This is the base of the styloid process and is encountered at a depth of about 1.5 inches (4 em.) from the skin incision. It is important to remember to stay high just under the root of the zygoma, so that the base of the styloid process is the first important structure to be identified.
- 51. With finger dissection and palpation, the styloid process can next be identified immediately below its base; a good headlight and a dry field greatly facilitate this stage of the operation. With gentle traction on the capsule of the parotid gland anteriorly, the facial nerve is brought into view, emerging from the medial aspect of the styloid process and coursing sharply upward and laterally to enter immediately the capsule of the parotid gland. The nerve usually is heavily invested in fascia and a.ccompanied by the stylomastoid artery that may prove troublesome if severed.