Pharmacodynamics (updated 2016) - drdhriti
•Descargar como PPT, PDF•
131 recomendaciones•16,300 vistas

An updated PowerPoint presentation on Pharmacodynamics suitable for UG MBBS level Medical students

Recomendados
Más contenido relacionado
La actualidad más candente
La actualidad más candente (20)
Similar a Pharmacodynamics (updated 2016) - drdhriti
Similar a Pharmacodynamics (updated 2016) - drdhriti (20)
Más de http://neigrihms.gov.in/
Más de http://neigrihms.gov.in/ (20)
Último
Último (20)
Pharmacodynamics (updated 2016) - drdhriti
- 1. Pharmacodynamics Dr. D. K. Brahma Department of Pharmacology NEIGRIHMS, Shillong
- 2. What is Pharmacodynamics? What drugs do to the body when they enter? Study of action-effect sequence of drugs and dose-effect relationship Defn.: It is the study of biochemical and physiological effects of drugs and their mechanism of action at organ level as well as cellular level Also Modification of action of one drug by another drug
- 3. Drug Action by Physical/Chemical properties • Color – Tincture Card co. • Physical mass – Ispaghula (laxative) • Physical form – Dimethicone (antifoaming) • Smell - Volatile Oils • Taste - Bitters • Osmotic action – Mannitol, Magsulf • Adsorption – Activated Charcoal • Soothing-demulcent – Soothing agents like calamine • Oxidizing property – Pot. Permanganate • Chelation – EDTA, dimercaprol • Radioactivity - Iodine and others • Radio-opacity – Barium sulfate • Chemical properties – Chelating agents (EDTA, dimercaprol) • Scavenging effect – Mesna (with cyclophosphamide)
- 4. PRINCIPLES OF DRUG ACTION - Do NOT impart new functions on any system, organ or cell - Only alter the PACE of ongoing activity • STIMULATION • DEPRESSION • IRRITATION • REPLACEMENT • CYTOTOXIC ACTION
- 5. PRINCIPLE S OF ACTION MODE EXAMPLE STIMULATION Selective Enhancement of level of activity of specialised cells - Excessive stimulation is often followed by depression of that function Adr stimulates Heart Pilocarpine stimulates salivary glands Picrotoxin – CNS stimulant convulsions coma death DEPRESSION Selective Diminution of activity of specialised cells Certain drugs – stimulate one cell type and depress others Barbiturates depress CNS Quinidine depresses Heart Ach – stimulates smooth muscle but depresses SA node IRRITATION Non-selective often noxious effect – applied to less specialised cells (epithelium, connective tissue) -stimulate associated function Bitters – salivary and gastric secretion Counterirritants increase blood flow to a site REPLACEMENT Use of natural metabolites, hormones or their congeners in deficiency states Levodopa in parkinsonism Iron in anaemia CYTOTOXIC ACTION Selective cytotoxic action for invading parasites or cancer cells – for attenuating them without affecting the host cells Penicillin, chloroquine
- 7. MECHANISM OF DRUG ACTION • MAJORITY OF DRUGS INTERACT WITH TARGET BIOMOLECULES: Usually a Protein 1. ENZYMES 2. ION CHANNELS 3. TRANSPORTERS 4. RECEPTORS
- 8. 1. Enzymes – drug targets • All Biological reactions are carried out under catalytic influence of enzymes – major drug target • Drugs – increases/decreases enzyme mediated reactions • In physiological system enzyme activities are optimally set • Enzyme stimulation is less common by drugs – common by endogenous substrates – Pyridoxine (cofactor in decarboxylase activity) – Adrenaline stimulates hepatic glycogen phosphorylase (hyperglycaemia) • Enzyme inhibition – common mode of DRUG action
- 9. Enzymes – contd. • Nonspecific inhibition: Denature of proteins – strong acids, heavy metals, alkalis, alcohol, phenols etc. • Specific Inhibition: Many Drugs Inhibit Specific enzyme • Competitive Noncompetitive Equilibrium Nonequilibrium
- 10. Competitive Enzyme Inhibition Equilibrium Type: • Structurally similar competes with substrate – binding sites • Product not formed/non functional • New equilibrium – kM increased, Vmax unchanged • Higher conc. of substrate – ½ maximal reaction • Sufficiently high conc. – Equal Vmax
- 11. Competitive Enzyme Inhibition • Nonequilibrium type: • Same catalytic site • Form strong covalent Bond • Normal substrate cannot displace • Organophosphorous compounds/Nerve gases (cholinesterase) • Methotrexate – 50,000 times DHFR than DHFA • kM: increased but Vmax reduced
- 12. Competitive Enzyme Inhibition - Examples • Physostigmine Vs Acetylcholine (cholinesterase) • Sulfonamides Vs PABA (folate synthetase) • Moclobemide Vs Catecholamines (MAO-A) • Captopril Vs Angiotensin 1 (ACE) • Finesteride Vs Testosterone (5α-reductase) • Carbidopa Vs Levodopa (dopa decarboxylase)
- 13. Noncompetitive Enzyme Inhibition Inhibitor reacts with an adjacent site not – catalytic site • Alters the Enzyme – loses catalytic property • kM unchanged and V max reduced • Examples: • Acetazolmide – Carbonic anhydrase • Aspirin – COX • Omeprazole (PP) – HKATpase • Digixin – NaKATPase • Theophylline – Phosphodiesterase • Lovastatin – HMG-CoA reductase
- 14. 2. Ion Channel • Proteins take part in transmembrane signaling and regulates ionic composition • Drugs also target these channels: mainly on 3 types – Ligand gated channels – G-protein operated channels – Direct action on channels • Examples: BZD opens ligand gated GABAA Cl- channel, Histamine binds GPCR and activates G-protein, local anesthetics – directly blocks channel • Many drugs modulate opening and closing of channels: Phenytoin, Ethosuximide, Nifedepine, Quinidine Nicorandil and Amiloride, etc.
- 15. + + - - + + -- - - + + + + - - Na+ + ++ + - - - - Resting (Closed**) Open (brief) inactivated Very slow repolarization in presence of LA LA receptor LA have highest affinity for the inactivated form Refractory period LA acting on Na+ receptorsLA acting on Na+ receptors
- 16. 3. Transporters • Substrates are translocated across membrane by binding to specific transporters (carriers) – Solute Carrier Proteins (SLC) • Pump the metabolites/ions in the direction of concentration gradient or against it • Drugs can interact with these transport system • Examples: ANS - Desipramine & cocaine (NET), Fluoxetine (SSRI), Amphetamine (DAT), Reserpine (vesicular reuptake of NA), Hemicholinium (choline uptake) and Vesamicol (active transport of Ach to vesicles); Kidney: Probenecid (penicillin and uric acid - OAT), Furosmide (blocks Na+K+2Cl- cotransport), Thiazides block Na+Cl- symporter, Amphetamine (blocks Dopamine reuptake),
- 17. Biomacromolecular targets of Drugs action 1. ENZYMES 2. CHANNELS 3. TRANSPORTERS 4. RECEPTORS
- 18. 4. Receptors • Many Drugs usually do not bind directly with enzymes, channels, transporters or structural proteins, but act through specific macromolecules – RECEPTORS … • Definition: It is defined as a macromolecule or binding site located on cell surface or inside the effector cell that serves to recognize the signal molecule/drug and initiate the response to it, but itself has no other function, e.g. Muscarinic (M type) and Nicotinic (N type) receptors of Cholinergic system
- 19. Some Common Terms • Agonist: An agent which activates a receptor to produce an effect similar to a that of the physiological signal molecule, e.g. Muscarine and Nicotine • Antagonist: an agent which prevents the action of an agonist on a receptor or the subsequent response, but does not have an effect of its own, e.g. atropine and muscarine • Inverse agonist: an agent which activates receptors to produce an effect in the opposite direction to that of the agonist, e.g. DMCM in BDZ receptors (DMCM (methyl 6,7-dimethoxy-4-ethyl-beta-carboline-3- carboxylate) • Partial agonist: An agent which activates a receptor to produce submaximal effect but antagonizes the action of a full agonist, e.g. opioids • Ligand: (Latin: ligare – to bind) - any molecule which attaches selectively to particular receptors or sites (refers only binding or affinity but no functional change)
- 20. Evidences of Drug action via receptors – Historical 1. Drugs exhibit structural specificity of action: example – Catecholamines (isopropyl substitution on ethylamine side chain of sympathetic drugs – cardiac and bronchial) 2. Competitive Antagonism: Between agonists and antagonists (Atropine - M type receptors) – by Langley 3. Acetylcholine - 1/6000th of cardiac cell surface – maximal effect – by Clark
- 21. Drug – Receptor occupation theory – Clark`s equation (1937) • Drugs are small molecular ligands (pace of cellular function can be altered) • Drug (D) and receptor (R) interaction governed by “law of mass action” • Effect (E) Is the direct function of the Drug-Receptor complex • But DR complex may not be sufficient to elicit E (response) • D must be able to bring a conformational change in R to get E • Affinity and Intrinsic activity (IA) D + R DR E (direct function of DR complex) K1 K2
- 22. Receptor occupation theory – contd. • Affinity: Ability to bind with a Receptor • Intrinsic activity (IA): Capacity to induce functional change in the receptor • Competitive antagonists have Affinity but no IA • Therefore, a theoretical quantity (S) – denoting strength of stimulus imparted to the cell was interposed D + R DR S E K1 K2
- 23. Definitions redefined If explained in terms of “affinity and IA”: • Agonist: Affinity + IA (1) • Antagonist: Affinity + IA (0) • Partial agonist: Affinity + IA (0-1) • Inverse agonist: Affinity + IA (0 to -1)
- 25. Nature of Receptors • Not hypothesis anymore – proteins and nucleic acids • Isolated, purified, cloned and amino acid sequencing done • Cell surface receptors remain floated in cell membrane lipids • Non-polar hydrophobic portion of the amino acid remain buried in membrane while polar hydrophilic remain on cell surface • Binding of small ligand – capable of tripping balance at distance site – brings conformational changes • Major classes of receptors have same structural motif – individual receptors differ in amino acid sequence, length of extra and intracellular loops etc. • Most drugs act on Physiological receptors – neurotransmitters, autacoides, hormones etc. • True drug receptors - BZD, Sulfonylureas (SUR1)
- 26. Receptor Subtypes • Evaluation of receptors and subtypes – lead to discovery of various newer target molecules • Example Acetylcholine - Muscarinic and Nicotinic – M1, M2, M3 etc. – NM and NN – α (alpha) and β (beta) …. • Criteria of Classification: 1. Pharmacological criteria – potencies of selective agonist and antagonists – Muscarinic, nicotinic, alpha and beta adrenergic etc. 2. Tissue distribution – beta 1 and beta 2 3. Ligand binding – Radiological radio-labelled ligands 4. Transducer pathway: MN and MM 5. Molecular cloning – based on cloning, amino acid sequencing and three dimensional structure
- 27. Action – effects ! • Receptors : Two essential functions: • Recognition of specific ligand molecule • Transduction of signal into response • Two Domains: • Ligand binding domain (coupling proteins) • Effectors Domain – undergoes functional conformational change • “Action”: Initial combination of the drug with its receptors resulting in a conformational change (agonist) in the later, or prevention of conformational change (antagonist) • “Effect”: It is the ultimate change in biological function brought about as a consequence of drug action, through a series of intermediate steps (transducers)
- 28. The Transducer mechanism • Most transmembrane signaling is accomplished by a small number of different molecular mechanisms (transducer mechanisms) • Complex multistep process - amplification and integration of concurrently received extra /intra cellular signals • Large number of receptors share these handful of transducer mechanisms to generate an integrated and amplified response • Mainly 4 (four) major categories: A. G-protein coupled receptors (GPCR) B. Receptors with intrinsic ion channel C. Enzyme linked receptors D. Transcription factors (receptors for gene expression)
- 29. A. G-protein Coupled Receptors (GPCR) • Large family of cell membrane receptors linked to the effector enzymes or channel or carrier proteins through one or more GTP activated proteins (G- proteins) • All receptors has common pattern of structural organization • The molecule has 7 α-helical membrane spanning hydrophobic amino acid segments – 3 extra and 3 intracellular loops • Agonist binding - on extracellular face and cytosolic segment binds coupling G-protein Transducer A ….
- 30. GPCR - 3 Major Pathways 1. Adenylyl cyclase:cAMP pathway 2. Phospholipase C: IP3-DAG pathway 3. Channel regulation
- 31. 1. Adenylyl cyclase: cAMP pathway PKA Phospholamban Increased Interaction with Ca++ Faster relaxation Troponin Cardiac contractility Other Functional proteins PKA alters the functions of many Enzymes, ion channels, transporters and structural proteins. Faster sequestration of Ca++ in SR
- 32. Adenylyl cyclase: cAMP pathway • Main Results: – Increased contractility of heart/impulse generation – Relaxation of smooth muscles – Lipolysis – Glycogenolysis – Lipolysis – Modulation of junctional transmission – Hormone synthesis – Opens specific type of Ca++ channel – Cyclic nucleotide gated channel (CNG) - - -heart, brain and kidney – Responses are opposite in case of AC inhibition
- 33. 2. Phospholipase C:IP3-DAG pathway PKc
- 34. IP3-DAG pathway • Main Results: – Mediates /modulates contraction – Secretion/transmitter release – Neuronal excitability – Intracellular movements – Eicosanoid synthesis – Cell Proliferation – Responses are opposite in case of PLc inhibition
- 35. 3. Channel regulation • Activated G-proteins can open or close ion channels – Ca++, Na+ or K+ etc. • These effects may be without intervention of any of above mentioned 2nd messengers – cAMP or IP/DAG • Bring about depolarization, hyperpolrization or Ca ++ changes etc. • Gs – Ca++ channels in myocardium and skeletal muscles • Go and Gi – open K+ channel in heart and muscle and close Ca+ in neurones
- 36. B. Receptors with Intrinsic Ion Channel • Cell Surface ligand gated ion channels – enclose ion selective channels – for Na+ , K+ , Ca+ or Cl- • Agonist binding opens the channel – depolarization/hyperpolarization etc. • Most useful drugs in clinical medicine act by mimicking or blocking the actions of endogenous ligands that regulate the flow of ions through plasma membrane channels • The natural ligands include acetylcholine, serotonin, aminobutyric acid (GABA), and the excitatory amino acids (e.g, glycine, aspartate, and glutamate) Transducer B ….
- 37. Receptors with Intrinsic Ion Channel (Ligand gated)
- 38. C. Enzyme Linked Receptors • Receptors with enzymatic property • Extracellular agonist-binding domain and a cytoplasmic catalytic domain – connected through transmembrane peptide chain • 2 (two) types of receptors: 1. Intrinsic enzyme linked receptors • Protein kinase or guanyl cyclase domain 1. JAK-STAT-kinase binding receptor Transducer C ….
- 39. i. Enzyme linked receptors • Agonist Binding - Upon binding to the receptor induces conversion of monomeric state to an active dimeric state – Activates tyrosine protein kinase (t-Pr-K) - sometimes serine and threonine Pk • Auto phosphorylates tyrosine residues on each other – also phosphorylates other SH2-Pr domain substrate proteins • Increases affinity for binding substrate proteins • Ultimately downstream signaling function • Examples – Insulin, EGF ------- Trastuzumab, antagonist of a such type receptor – used in breast cancer • Dimerization – also promotes internalization, degradation in lysosomes and down regulation
- 40. ii. JAK-STAT-kinase Binding Receptor • Mechanism closely resembles that of receptor tyrosine kinases • Only difference - protein tyrosine kinase activity is not intrinsic to the receptor molecule • Dimerization – activates intracellular domain- affinity to bind Free cytosolic protein kinase JAK (Janus kinase) • JAK phosphorylates tyrosine residues – binds to STAT (Signal transducer and activation of transcription) • Activated JAK phosphorylates STAT tyrosine residues • Phosphorylated STAT dimerize, dissociate from receptor and moves to nucleus • Examples – cytokines, growth hormones, interferones etc.
- 42. Receptors regulating gene expression • Intracellular – cytoplasmic or nuclear – responds to lipid soluble chemical messenger • The receptor proteins – specific for each hormone/regulator – capable of binding to specific genes – but kept inhibited • Agonist binding exposes the DNA binding regulatory segment
- 43. Receptors of gene expression - Image
- 44. D. Receptors regulating gene expression • Intracellular (cytoplasmic or nuclear) receptors • Lipid soluble biological signals cross the plasma membrane and act on intracellular receptors • Receptors for corticosteroids, mineralocorticoids, thyroid hormones, sex hormones and Vit. D etc. stimulate the transcription of genes in the nucleus by binding with specific DNA sequence – called - “Responsive elements” – to synthesize new proteins • Hormones produce their effects after a characteristic lag period of 30 minutes to several hours – gene active hormonal drugs take time to be active (Bronchial asthma) • Beneficial or toxic effects persists even after withdrawal Transducer D ….
- 45. Receptor Regulation • Receptors – exist in Dynamic state – density and efficacy being regulated by the level of ongoing activity • Up regulation of receptors: – In typically active systems, prolonged deprivation of agonist (by denervation or antagonist) results in supersensitivity of the receptor as well as to effector system to the agonist. Sudden discontinuation of Propranolol, Clonidine, opioid withdrawal etc. – 3 mechanisms - Unmasking of receptors or proliferation (up regulation) or accentuation of signal amplification
- 46. Receptor Regulation – contd. • Conversely - continued exposure to an agonist or intense receptor stimulation causes desensitization or refractoriness: receptor become less sensitive to the agonist • Examples – beta adrenergic agonist and levodopa • Causes: 1. Masking or internalization of the receptors 2. Decreased synthesis or increased destruction of the receptors (down regulation) - Tyrosine kinase receptors
- 47. Mechanism of Masking or internalization ßARK (beta-adrenergic receptor kinase) Beta-arrestin
- 48. Desensitization • Sometimes response to all agonists which act through different receptors but produce the same overt effect is decreased by exposure to anyone of these agonists – heterologous desensitization • Homologous – when limited to the agonist which is repeatedly activated • Mechanism: Homologous – BARK-arrestin; Heterologous - In GPCRs (PKA or PKC) Kinases may also phosphorylate the GPCRs R+ TransducerHomologous Ach Hist Heterologous
- 49. Functions of Receptors - Summary 1. To Regulate signals from outside the cell to inside the effector cell – signals not permeable to cell membrane 2. To amplify the signal 3. To integrate various intracellular and extracellular signals 4. To adapt to short term and long term changes and maintain homeostasis.
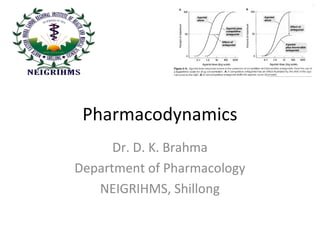
- 50. Dose-Response Relationship • Drug administered – 2 components of dose- response – Dose-plasma concentration – Plasma concentration (dose)-response relationship – Obeys law of mass action • E is expressed as Emax X [D] Kd + [D] E is observed effect of drug dose [D], Emax = maximum response, KD = dissociation constant of dose of drug receptor complex at which half maximal response is produced E max
- 51. Dose-Response Curve dose in ml of 10 mcg/ml dose Log dose %response %response 100% - 50% - 100% - 50% - E = Emax X [D] Kd + [D] ! ! ! ! ! ! 0.2 0.4 0.8 1.6 3.2 6.4
- 52. Dose-Response Curve • Advantages: – Stimuli can be graded by Fractional change in stimulus intensity – A wide range of drug doses can easily be displayed on a graph – Potency and efficacy can be compared – Comparison of study of agonists and antagonists become easier
- 53. How we get DRC in vitro Practically?? • Example: Frog rectus muscle and Acetylcholine response – in millimeters – Can compare with a drug being studied for having skeletal muscle contracting property
- 54. Potency and efficacy • Potency: It is the amount of drug required to produce a certain response • Efficacy: Maximal response that can be elicited by the drug Response Drug in log conc. 1 2 3 4
- 55. Potency and efficacy - Examples • Aspirin is less potent as well as less efficacious than Morphine • Pethidine is less potent analgesic than Morphine but eually efficacious • Diazepam is more potent but less efficacious CNS depressant than phenobarbitone • Furosemide is less potent but more efficacious than metozolone • Potency and efficacy are indicators only in different clinical settings e.g. Diazepam Vs phenobarbitone (overdose) and furosemide vs thaizide (renal failure)
- 56. Slope of DRC • Slope of DRC is also important • Steep slope – moderate increase in dose markedly increase the response (individualization) • Flat DRC – little increase in response occurs in wide range of doses (standard dose can be given to most ptients) • Example: Hydralazine and Hydrochlorothiazide DRC in Hypertension Hydralazine Thiazide FallinBP
- 57. Selectivity • Drugs produce different effects – not single • DRC of different effects may be different • Example – Isoprenaline – Bronchodilatation and cardiac stimulation – same DRC • Salbutamol – different (selective bronchodilatation)
- 58. Therapeutic index (TI) • It is defined as the gap between therapeutic effect DRC and maximal acceptable adverse effect DRC (also called margin of safety)
- 59. Therapeutic index (TI) • In experimental animals • Therapeutic Index = Median Lethal Dose (LD50) Median Effective dose (ED50) Idea of margin of safety Margin of Safety
- 60. Risk-benefit Ratioo • Estimated harm (ADRs, Cost, inconvenience) Vs • Expected advantages (relief of symptoms, cure, reduction of complications, mortality, improvement of life etc.)
- 61. Combined Effects of Drugs • Drug Synergism: – Additive effect (1 + 1 = 2) • Aspirin + paracetamol, amlodipine + atenolol, nitrous oxide + halothane – Supra-additive effect (1 + 1 = 4) • Sulfamethoxazole + trimethoprim, levodopa + carbidopa, acetylcholine + physostigmine • PABA DHFA THFA Sulfamethoxazole Trimethoprim Folate synthase Dihydrofolate Reductase
- 62. Drug Antagonism 1. Physical: Charcoal 2. Chemical: KMnO4, Chelating agent 3. Physiological antagonism: Histamine and adrenaline in bronchial asthma, Glucagon and Insulin 4. Receptor antagonism: One drug blocks receptor action of others, also blocks physiological signal molecules – relatively selective (Ach Vs Histamine in SM contraction) a. Competitive antagonism (equilibrium) b. Non-competitive c. Non-equilibrium (competitive)
- 63. Receptor antagonism - curves o Competitive: o Antagonist is chemically similar to agonist and binds to same receptor molecules o Affinity (1) but IA (0), Result – no response o Log DRC shifts to the right o But, antagonism is reversible – increase in concentration of agonist overcomes the block o Parallel shift of curve to the right side o Non-competitive: o Allosteric site binding altering receptor not to bind with agonist o No competition between them – no change of effect even agonist conc. .is increased o Flattening of DRC of agonist by increasing the conc. Of antagonist o Experimental - no clinical basis
- 64. Receptor antagonism - curves • Non – equilibrium: – Antagonists Binds receptor with strong bond – Dissociation is slow and agonists cannot displace antagonists (receptor occupancy is unchanged) – Irreversible antagonism developes – DRC shifts to the right and Maximal response lowered
- 66. Drug antagonism DRC – competitive nonequillibrium antagonismResponse Shift to the right and lowered response Drug in log conc. Agonist Agonist + CA (NE)
- 67. Spare Receptor • When only a fraction of the total population of receptors in a system, are needed to produce maximal effect, then the particular system is said to have spare receptors • Example – Adrenaline (90%)
- 68. Competitive Vs NC antagonism Competitive • Binds to same receptor • Resembles chemically • Parallel right shift of DRC in increasing dose of agonist • Intensity depends on the conc. Of agonist and antagonist • Example – Ach and atropine, Morphine and Naloxone Noncompetitive • Binds to other site • No resemblance • Maximal response is suppressed • Depends only on concentration of antagonist • Diazepam - Bicuculline
- 69. Summary • Basic Principles of Pharmacodynamics • Mechanisms of drug action – Enzymes, Ion channels, Transporters and Receptors with examples • Definitions of affinity, efficacy, agonist and antagonists etc. • Drug transducer mechanisms • GPCR and different GPCR transducing mechanisms – cAMP, Protein kinase etc. • Up regulation and down regulation of receptors and desensitization • Principles of dose response curves and curves in relation to agonist, competitive antagonist etc. • Therapeutic index, margin of safety and risk-benefit ratio concepts • Combined effects of drugs – synergism etc. • Dose response curve (DRC) – agonist and antagonist
- 70. Thank you
Notas del editor
- PIP2 – phosphatidyl inositol 4,5-bisphosphate
- Ligand gated channels – enclose ion selective channels – Na, K+, ca++ or Cl within their molecules. 4 domains in each of which amino acid chains traverse