IVMS- Basic Medical Science of Valvular Heart Disease
•
7 recomendaciones•1,510 vistas

IVMS- Basic Medical Science of Valvular Heart Disease

Recomendados
Más contenido relacionado
La actualidad más candente
La actualidad más candente (20)
Destacado
Destacado (12)
Similar a IVMS- Basic Medical Science of Valvular Heart Disease
Similar a IVMS- Basic Medical Science of Valvular Heart Disease (20)
Más de Imhotep Virtual Medical School
Más de Imhotep Virtual Medical School (20)
Último
Último (20)
IVMS- Basic Medical Science of Valvular Heart Disease
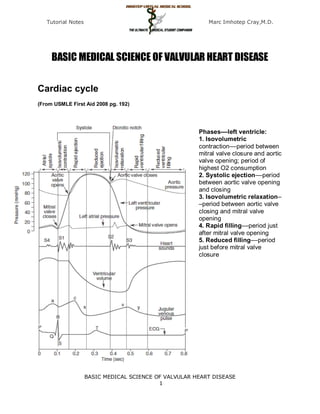
- 1. Tutorial Notes Marc Imhotep Cray,M.D. BASIC MEDICAL SCIENCE OF VALVULAR HEART DISEASE Cardiac cycle (From USMLE First Aid 2008 pg. 192) Phases––left ventricle: 1. Isovolumetric contraction––period between mitral valve closure and aortic valve opening; period of highest O2 consumption 2. Systolic ejection––period between aortic valve opening and closing 3. Isovolumetric relaxation– –period between aortic valve closing and mitral valve opening 4. Rapid filling––period just after mitral valve opening 5. Reduced filling––period just before mitral valve closure BASIC MEDICAL SCIENCE OF VALVULAR HEART DISEASE 1
- 2. Tutorial Notes Marc Imhotep Cray,M.D. Ventricular Pressure-Volume Loop Changes in Valve Disease Phases––left ventricle: 1. Isovolumetric contraction––period between mitral Cardiac valve disease valve closure and aortic valve opening; period of significantly alters ventricular highest O2 consumption pressure and volume 2. Systolic ejection––period between aortic valve relationships during the cardiac opening and closing cycle. A convenient way to analyze cardiac pressure and 3. Isovolumetric relaxation––period between aortic volume changes is by using valve closing and mitral valve opening ventricular pressure-volume 4. Rapid filling––period just after mitral valve loops. The links below will opening illustrate the pressure-volume 5. Reduced filling––period just before mitral valve changes that occur with the closure following valve defects: Mitral stenosis Aortic stenosis Mitral regurgitation Aortic regurgitation BASIC MEDICAL SCIENCE OF VALVULAR HEART DISEASE 2
- 3. Tutorial Notes Marc Imhotep Cray,M.D. Cardiac Valve Disease Tutorial Aortic valve stenosis http://en.wikipedia.org/wiki/Aortic_valve_stenosis Aortic valve stenosis (AS) is a valvular heart disease caused by the incomplete opening of the aortic valve. The aortic valve controls the direction of blood flow from the left ventricle to the aorta. When in good working order, the aortic valve does not impede the flow of blood between these two spaces. Under some circumstances, the aortic valve becomes narrower than normal, impeding the flow of blood. This is known as aortic valve stenosis, or aortic stenosis, often abbreviated as AS. An aortic valve that, due to rheumatic heart disease, has a severe stenosis (centre of image). The pulmonary trunk is seen at the lower right (of the image). The proximal portion of right coronary artery and its ostium can be seen at the lower left (of the image). The proximal left main coronary artery and its ostium are seen on the right (of the image). Autopsy specimen. BASIC MEDICAL SCIENCE OF VALVULAR HEART DISEASE 3
- 4. Tutorial Notes Marc Imhotep Cray,M.D. Simultaneous left ventricular and aortic pressure tracings demonstrate a pressure gradient between the left ventricle and aorta, suggesting aortic stenosis. The left ventricle generates higher pressures than what is transmitted to the aorta. The pressure gradient, caused by aortic stenosis, is represented by the green shaded area. (AO = ascending aorta; LV = left ventricle; ECG = electrocardiogram.) Symptoms of aortic stenosis Congestive heart failure Syncope Angina BMS TUTORIAL/ Cardiovascular Physiology Concepts Cardiovascular Physiology Concepts Cardiac Valve Disease Pathophysiology of valve disease CLINICAL READ/ Emedicine Aortic Stenosis BASIC MEDICAL SCIENCE OF VALVULAR HEART DISEASE 4
- 5. Tutorial Notes Marc Imhotep Cray,M.D. Aortic insufficiency http://en.wikipedia.org/wiki/Aortic_insufficiency Aortic insufficiency (AI), also known as aortic regurgitation (AR), is the leaking of the aortic valve of the heart that causes blood to flow in the reverse direction during ventricular diastole, from the aorta into the left ventricle. Aortic insufficiency can be due to abnormalities of either the aortic valve or the aortic root (the beginning of the aorta). BEFORE SURGICAL REPAIR AFTER SURGICAL REPAIR Pathophysiology In aortic insufficiency, when the pressure in the left ventricle falls below the pressure in the aorta, the aortic valve is not able to completely close. This causes a leaking of blood from the aorta into the left ventricle. This means that some of the blood that was already ejected from the heart is regurgitating back into the heart. The percentage of blood that regurgitates back through the aortic valve due to AI is known as the regurgitant fraction. For instance, if an individual with AI has a stroke volume of 100 ml and during ventricular diastole 25 ml regurgitates back through the aortic valve, the regurgitant fraction is 25%. This regurgitant flow causes a decrease in the diastolic blood pressure in the aorta, and therefore an increase in the pulse pressure (systolic pressure - diastolic pressure). Since some of the blood that is ejected during systole regurgitates back into the left ventricle during diastole, there is decreased effective forward flow in AI. BASIC MEDICAL SCIENCE OF VALVULAR HEART DISEASE 5
- 6. Tutorial Notes Marc Imhotep Cray,M.D. Note that while diastolic blood pressure is diminished and the pulse pressure widens, systolic blood pressure generally remains normal or can even be slightly elevated. This is because sympathetic nervous system and the renin-angiotensin-aldosterone axis of the kidneys compensate for the decreased cardiac output. Catecholamines will increase the heart rate and increase the strength of ventricular contraction, directly increasing cardiac output. Catecholamines will also cause peripheral vasoconstriction, which causes increased systemic vascular resistance and ensures that core organs are adequately perfused. Renin, a proteolytic enzyme, cleaves angiotensinogen to angiotensin I, which is converted to angiotensin II, which is also a potent vasoconstrictor. In the case of chronic aortic insufficiency with resultant cardiac remodeling, heart failure will develop, and it is possible to see systolic pressures diminish. Aortic insufficiency causes both volume overload (elevated preload) and pressure overload (elevated afterload) of the heart. The pressure overload (due to elevated pulse pressure and the systemic effects of neuroendocrine hormones) causes left ventricular hypertrophy (LVH). There is both concentric hypertrophy and excentric hypertrophy in AI. The concentric hypertrophy is due to the increased left ventricular systolic pressures associated with AI, while the excentric hypertrophy is due to volume overload caused by the regurgitant fraction. Hemodynamics The hemodynamic sequelae of AI are dependent on the rate of onset of AI. Acute AI and chronic AI will have different hemodynamics and individuals will have different signs and symptoms. Acute aortic insufficiency In acute AI, as may be seen with acute perforation of the aortic valve due to endocarditis, there will be a sudden increase in the volume of blood in the left ventricle. The ventricle is unable to deal with the sudden change in volume. In terms of the Frank-Starling curve, the end-diastolic volume will be very high, such that further increases in volume result in less and less efficient contraction. The filling pressure of the left ventricle will increase. This causes pressure in the left atrium to rise, and the individual will develop pulmonary edema. Severe acute aortic insufficiency is considered a medical emergency. There is a high mortality rate if the individual does not undergo immediate surgery for aortic valve replacement. If the acute AI is due to aortic valve endocarditis, there is a risk that the new valve may become seeded with bacteria. However, this risk is small. Acute AI usually presents as florid congestive heart failure, and will not have any of the signs associated with chronic AI since the left ventricle had not yet developed the eccentric hypertrophy and dilatation that allow an increased stroke volume, which in turn cause bounding peripheral pulses. On auscultation, there may be a short diastolic murmur and a soft S1. S1 is soft because the elevated filling pressures close the mitral valve in diastole (rather than the mitral valve being closed at the beginning of systole). BASIC MEDICAL SCIENCE OF VALVULAR HEART DISEASE 6
- 7. Tutorial Notes Marc Imhotep Cray,M.D. Chronic aortic insufficiency If the individual survives the initial hemodynamic derailment that acute AI presents as, the left ventricle adapts by eccentric hypertrophy and dilatation of the left ventricle, and the volume overload is compensated for. The left ventricular filling pressures will revert to normal and the individual will no longer have overt heart failure. In this compensated phase, the individual may be totally asymptomatic and may have normal exercise tolerance. Eventually (typically after a latency period) the left ventricle will become decompensated, and filling pressures will increase. While most individuals would complain of symptoms of congestive heart failure to their physicians, some enter this decompensated phase asymptomatically. Proper treatment for AI involves aortic valve replacement prior to this decompensation phase. BMS TUTORIAL/ Cardiovascular Physiology Concepts Cardiac Valve Disease Pathophysiology of valve disease CLINICAL READ/eMEDICINE Aortic Regurgitation Mitral stenosis http://en.wikipedia.org/wiki/Mitral_valve_stenosis Mitral stenosis is a valvular heart disease characterized by the narrowing of the orifice of the mitral valve of the heart. BASIC MEDICAL SCIENCE OF VALVULAR HEART DISEASE 7
- 8. Tutorial Notes Marc Imhotep Cray,M.D. Mitral stenosis with marked thickening of the leaflets and left atrial hypertrophy. Superior view. Autopsy preparation. Rheumatic heart disease at autopsy with characteristic findings (thickened mitral valve, thickened chordae tendineae, hypertrophied left ventricular myocardium). BASIC MEDICAL SCIENCE OF VALVULAR HEART DISEASE 8
- 9. Tutorial Notes Marc Imhotep Cray,M.D. Intracardiac pressure measurements in an individual with severe mitral stenosis. Pressure tracings in the left atrium (LA) and the left ventricle (LV) in an individual with severe mitral stenosis. Blue areas represent the diastolic pressure gradient due to the stenotic valve. Pathophysiology The normal area of the mitral valve orifice is about 4 to 6 cm2. Under normal conditions, a normal mitral valve will not impede the flow of blood from the left atrium to the left ventricle during (ventricular) diastole, and the pressures in the left atrium and the left ventricle during ventricular diastole will be equal. The result is that the left ventricle gets filled with blood during early ventricular diastole, with only a small portion of extra blood contributed by contraction of the left atrium (the "atrial kick") during late ventricular diastole. When the mitral valve area goes below 2 cm2, the valve causes an impediment to the flow of blood into the left ventricle, creating a pressure gradient across the mitral valve. This gradient may be increased by increases in the heart rate or cardiac output. As the gradient across the mitral valve increases, the amount of time necessary to fill the left ventricle with blood increases. Eventually, the left ventricle requires the atrial kick to fill with blood. As the heart rate increases, the amount of time that the ventricle is in diastole and can fill up with blood (called the diastolic filling period) decreases. When the heart rate goes above a certain point, the diastolic filling period is insufficient to fill the ventricle with blood and pressure builds up in the left atrium, leading to pulmonary congestion. When the mitral valve area goes less than 1 cm2, there will be an increase in the left atrial pressures (required to push blood through the stenotic valve). Since the normal left ventricular diastolic pressures is about 5 mmHg, a pressure gradient across the mitral valve of 20 mmHg due to severe mitral stenosis will cause a left atrial pressure of about 25 mmHg. This left atrial pressure is transmitted to the pulmonary vasculature and causes pulmonary hypertension. Pulmonary capillary pressures in this level cause an imbalance between the hydrostatic pressure and the oncotic pressure, leading to extravasation of fluid from the vascular tree and pooling of fluid in the lungs (congestive heart failure causing pulmonary edema). The constant pressure overload of the left atrium will cause the left atrium to increase in size. As the left atrium increases in size, it becomes more prone to develop atrial fibrillation. When atrial fibrillation develops, the atrial kick is lost (since it is due to the normal atrial contraction). In individuals with severe mitral stenosis, the left ventricular filling is dependent on the atrial kick. The loss of the atrial kick due to atrial fibrillation can cause a precipitous decrease in cardiac output and sudden congestive heart failure. Patients with mitral stenosis prompts a series of hemodynamic changes that frequently cause deterioration of the patient's clinical status. A reduction in cardiac output, associated with acceleration of heart rate and shortening of the diastolic time, frequently leads to congestive heart failure. In addition, when AF sets in, systemic embolization becomes a real danger. BMS TUTORIAL/ Cardiovascular Physiology Concepts Cardiac Valve Disease Pathophysiology of valve disease CLINICAL READ/ eMEDICINE BASIC MEDICAL SCIENCE OF VALVULAR HEART DISEASE 9
- 10. Tutorial Notes Marc Imhotep Cray,M.D. Mitral Stenosis Mitral regurgitation http://en.wikipedia.org/wiki/Mitral_insufficiency Mitral regurgitation (MR), mitral insufficiency or mitral incompetence is a disorder of the heart in which the mitral valve does not close properly when the heart pumps out blood. It is the abnormal leaking of blood from the left ventricle, through the mitral valve, and into the left atrium, when the left ventricle contracts, i.e. there is regurgitation of blood back into the left atrium. MR is the most common form of valvular heart disease. An illustration of mitral annular calcification, an aging phenomenon which can cause mitral regurgitation. It can also be associated with calcifications of aortic cusps causing stenosis and extension of calcification into cardiac skeleton causing heart block. Acute phase Acute mitral regurgitation (as may occur due to the sudden rupture of a chordae tendineae or papillary muscle) causes a sudden volume overload of both the left atrium and the left ventricle. The left ventricle develops volume overload because with every contraction it now has to pump out not only the volume of blood that goes into the aorta (the forward cardiac output or forward stroke volume), but also the blood that regurgitates into the left atrium (the regurgitant volume). The combination of the forward stroke volume and the regurgitant volume is known as the total stroke volume of the left ventricle. BASIC MEDICAL SCIENCE OF VALVULAR HEART DISEASE 10
- 11. Tutorial Notes Marc Imhotep Cray,M.D. In the acute setting, the stroke volume of the left ventricle is increased (increased ejection fraction), this happens because of more complete emptying of heart. However, as it progresses the LV volume increases and the contractile function deteriorates and thus leading to dysfunctional LV and a decrease in ejection fraction.The mechanism by which the total stroke volume is increased is known as the Frank-Starling mechanism. The regurgitant volume causes a volume overload and a pressure overload of the left atrium. The increased pressures in the left atrium inhibit drainage of blood from the lungs via the pulmonary veins. This causes pulmonary congestion. Chronic phase Compensated If the mitral regurgitation develops slowly over months to years or if the acute phase can be managed with medical therapy, the individual will enter the chronic compensated phase of the disease. In this phase, the left ventricle develops eccentric hypertrophy in order to better manage the larger than normal stroke volume. The eccentric hypertrophy and the increased diastolic volume combine to increase the stroke volume (to levels well above normal) so that the forward stroke volume (forward cardiac output) approaches the normal levels. In the left atrium, the volume overload causes enlargement of the chamber of the left atrium, allowing the filling pressure in the left atrium to decrease. This improves the drainage from the pulmonary veins, and signs and symptoms of pulmonary congestion will decrease. These changes in the left ventricle and left atrium improve the low forward cardiac output state and the pulmonary congestion that occur in the acute phase of the disease. Individuals in the chronic compensated phase may be asymptomatic and have normal exercise tolerances. Decompensated An individual may be in the compensated phase of mitral regurgitation for years, but will eventually develop left ventricular dysfunction, the hallmark for the chronic decompensated phase of mitral regurgitation. It is currently unclear what causes an individual to enter the decompensated phase of this disease. However, the decompensated phase is characterized by calcium overload within the cardiac myocytes. In this phase, the ventricular myocardium is no longer able to contract adequately to compensate for the volume overload of mitral regurgitation, and the stroke volume of the left ventricle will decrease. The decreased stroke volume causes a decreased forward cardiac output and an increase in the end-systolic volume. The increased end-systolic volume translates to increased filling pressures of the ventricular and increased pulmonary venous congestion. The individual may again have symptoms of congestive heart failure. The left ventricle begins to dilate during this phase. This causes a dilatation of the mitral valve annulus, which may worsen the degree of mitral regurgitation. The dilated left ventricle causes an increase in the wall stress of the cardiac chamber as well. BASIC MEDICAL SCIENCE OF VALVULAR HEART DISEASE 11
- 12. Tutorial Notes Marc Imhotep Cray,M.D. Demonstrations: Heart Sounds & Murmurs While the ejection fraction is less in the chronic decompensated phase http://depts.washington.edu/p than in the acute phase or the chronic compensated phase of mitral hysdx/heart/demo.html regurgitation, it may still be in the normal range (ie: > 50 percent), and Description Sounds may not decrease until late in the disease course. A decreased ejection fraction in an individual with mitral regurgitation and no other cardiac Normal abnormality should alert the physician that the disease may be in its heart sounds decompensated phase. Murmurs Audio examples Aortic stenosis ( early) & AS- late Mitral regurgitation Pulmonic stenosis Aortic insufficiency Mitral stenosis Benign murmur Atrial septal defect Ventricular septal defect Patent ductus arteriosus Extra heart Audio examples sounds Split S2 S3 BASIC MEDICAL SCIENCE OF VALVULAR HEART DISEASE 12