Maxillofacial prosthesis of soft cleft palate
•Descargar como PPTX, PDF•
57 recomendaciones•19,207 vistas


Recomendados
Más contenido relacionado
La actualidad más candente
La actualidad más candente (20)
Similar a Maxillofacial prosthesis of soft cleft palate
Similar a Maxillofacial prosthesis of soft cleft palate (20)
Maxillofacial prosthesis of soft cleft palate
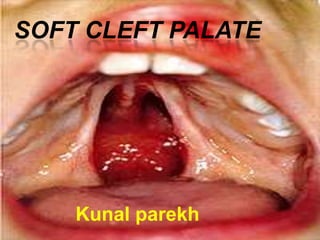
- 1. SOFT CLEFT PALATE Kunal parekh
- 2. In simpler terms, a palatal obturator covers any fistulas (or "holes") in the roof of the mouth that lead to the nasal cavity, providing the wearer with a plastic/acrylic, removable roof of the mouth, which aids in speech, eating, and proper air flow.
- 4. Palatal Obturator Closes or occludes opening caused by cleft or fistula Used to facilitate separation of oral & nasal cavities for speech, feeding, & swallowing hypernasality suckling ability in babies
- 6. A palatal obturator may be used to compensate for hypernasality and to aid in speech therapy targeting correction of compensatory articulation caused by the cleft palate. Speech bulbs and palatal lifts aid in velopharyngeal closure and do not obturate a fistula. A speech bulb, yet another type of prosthetic device often confused with a palatal obturator, contains a pharyngeal section, which goes behind the soft palate.
- 8. General rule for prosthodontist… 1. The obturator for an adult patient shold be located in the nasopharynx at the level of normal palatal closure. 2. The inferior margin of the obturator should be placed at the level of greatest muscular activity exhibited by the residual palatophryngeal complex. 3. The inferior extension of the obturator will usually be an extension of the palatal plane as extended to the posterior pharyngeal wall.
- 9. PROSTHETIC TREATMENT OF SOFT PALATE CLEFTS
- 10. TYPES OF OBTURATOR three types Fixe pharyngeal. Hinged pharyngeal. Meatal. Type---- Immediate surgical obturation Delayed surgical obturation
- 11. Obturator Categories Modification Obturator Short term Interim Obturator Post surgery Definitive Obturator Long term
- 12. TYPES OF OBTURATOR The fixed is an extension of a denture projecting in to the pharynx at about the level of the anterior arch of the atlas and shaped so that it can be griped by the pharyngeal walls. The hinged is attached to the posterior border of a denture by a hinge and its lateral borders are shaped so that they may be griped by the remnants of the soft palate and be raised and lowered with them .
- 13. The meatal obturator is an extension of the back of the denture, upwards at right angles to It, so that it occludes the opening of the posterior nares. The meatal obturator is only used in cases presenting a very large cleft and is difficult to adjust so that it prevents the nasal escape of air when speaking the oral consonants and does not help the patient when swallowing.
- 15. A meatus obturator is designed to close the posterior nasal choanae through a vertical extension from the distal aspect of the maxillary prosthesis. Such a design will reduce leverage factors on the prosthesis but will not permit function of the pharyngeal muscles against it. The meatus oburator is often thought to be mechanical while the fixed pharyngeal obturator is thought to be more physiologic. The hinged pharyngeal oburator is not often referred to in recent times because of the mechanics involved in its fabrication.
- 16. Design of the prosthesis •must apply the basic principles of support, retention and stability so as to minimize the stress generated to the structures of the mouth. • All of these entities need to be considered in detail before prosthetic intervention is undertaken. •The location of the fulcrum line, retentive undercuts and potential for indirect retention will be important factors in determining the prognosis. •In general, the prosthesis will have a fulcrum line near the defect area.
- 17. •If natural teeth or implants are present to provide retention and support for the prosthesis, the fulcrum line will pass between the most posterior occlusal rests on each side of the arch. •Retentive clasps placed into undercuts adjacent to the defect will resist the downward displacement of the prosthesis due to the effects of gravity. •Occlusal rests on the opposite side of the fulcrum line from the defect will act as indirect retainers. Long guide planes on the natural teeth will also assist in prevention of rotational dislodgment of the prosthesis.
- 18. IMPRESSION MAKING Procedure Upper and lower perforated stock trays were selected. Upper tray was modified with wax extension into the defect to record the defect. Then upper and lower preliminary impressions were made with irreversible hydrocolloid. The upper impression also records the defect. Impressions were poured with dental stone to make diagnostic casts.
- 21. Next step is the fabrication of special tray for border molding. Lower special tray is fabricated in conventional manner using autopolymerising acrylic resin.
- 22. But during the fabrication of upper tray following factors were kept in mind. There should be a 5 mm gap between the bulb and posterior pharyngeal wall. Angle of the bulb should be approximately 20° relative to the palatal plane. Keeping in mind all these criteria upper special tray was fabricated with autopolymerising acrylic resin having pharyngeal extension. Impression of the defect area was made with modeling plastic wax.
- 24. Border molding was accomplished by recording all the functional movements of the soft palate, i.e., by asking the patient to tilt her head side-to-side and front-back when sitting upright. the patient is instructed to flex the neck fully to achieve contact of the chin to the chest. This movement will establish contact of the middle third of the soft palate with the soft tissue covering the dorsal tubercle of the atlas. Lateral aspects of the lift are formed by rotation and flexion of the neck to achieve chin contact with the right and left shoulder respectively.
- 25. Check indentation made by the ant. And posterior tonsillar pillars, the tori tubari , passavant’s pas, and the anterior tubercule of the atlas. Shiny area will indicate the lack of tissue contact. Activated pharyngeal musculature will displaced the excess modeling plastic superiorly and inferiorly and these excess should be trimmed.
- 27. If the position and contours of the obturators are satisfactory , reduced all extension approximately by 1mm. Add thermoplastic wax because this will ensure the overextension of obturator. Contour modification are done if required.
- 28. Oral surface should be concave to provide space for tongue. Superior surface should be convex and well polished to facilitate the deflection of nasal secretion into oropharynx. Area of excessive pressure are relieved using pressure indicating paste on lateral and posterior wall.
- 29. Placement of thermoplastic corrective wax onto oropharyngeal extension.
- 30. Recording of surgical defect with thermoplastic corrective wax.
- 31. A. Thermoplastic corrective wax removed from base. B, Autopolymerizing resin added to space provided by thermoplastic corrective wax.
- 32. If hyponasal voice is still evident ..then postero- lateral dimensions of the obturator is reduced judiciously.
- 33. Size and position of obturator….factors to be consider 1.The closure of soft palate against the posterior pharyngeal wall extends approximately 5-7mm in vertical height with closure at o above the level of the palatal plane. 2.At pharyngeal wall activity ( middle position of obturator) the speech is is best for patients.
- 34. Test for speech,,-- aids in assessing the perceived resonance balance 1. Manometric air pressure recordings. 2.Comparatie oral and nasal airflow measurements. 3. Sound spectrographic analyses
- 35. Lower Border molding was done in conventional manner. Boxing was done and impressions were poured with die stone to fabricate master casts.
- 36. Procedure for edentulous patient Autopolymerising acrylic resin record bases were made. In case of upper record base did not include the pharyngeal extension. Jaw relations and try in was done in accordance with for conventional complete denture fabrication procedures. After try in was over, all the undercuts of the defect area were blocked with wax. Flasking and dewaxing was done. Then dentures were processed with heat cure acrylic resin. Lid for the bulb was processed separately with heat curing acrylic resin and was attached to the completed denture with autopolymerising acrylic resin.
- 37. Patient found drastic improvement in speech and nasal regurgitation was reduced. Patient was advised to continue her referral to speech therapist. . Once surgical care and speech therapy have been completed, the need for follow-up care is needed unless specific problems manifest. Preventive care is imperative if long-term preservation of the supporting structures is desired.
- 38. SILICONE RETENTIVE OBTURATOR In congenital clefts of the hard palate , enclosed or open- ended, and acquired clefts , a use fullform of obturator is made of silicone ( or latex rubber ) which is attached to the denture by studs . The obturator is removable and adjustments can be made . the design is useful in the edentulous cleft patient and in large acquired defects of the palate where retention is a major problem.
- 39. STAGES Cut a postdam 5mm from the edge of the cleft on the master cast . Fill the cleft with wax and carve to the contour of a normal palate . Add a sheet of wax . Embed two studs. Take an impression of the cast in elastomer . Add to studs to the impression and pour it to produce a working cast.
- 40. Use working cast to make a complete denture. Pour a plaster register to the master cast to hold the studs in relation to the cleft. Fill the cleft with silicone rubber in produce the obturator which is retained on the studs on the denture. The master cast serves as a permanent mould for replacement obturators If soft palate obturation is required then gutta-percha can be added to the silicone obturator and, after moulding in the mouth , returned to the master mould and studs prior to making a new , accurate mould.
- 41. A modification obturator may be used in the short-term to block a palatal fistula, for augmentation of the seal and to separate the oral and nasal cavities. An interim palatal obturator is used post-palatal surgery. A definitive obturator is used when further rehabilitation is not possible for the patient and is intended for long-term use
- 42. This obturator aids in closing the remaining fistula and is used when no further surgical procedures are planned. It must be frequently revised.
- 43. Limitations of Prosthetic Devices • Require insertion and removal Have to redo periodically due to growth Can be lost or damaged May be very uncomfortable Compliance is often poor Don’t permanently correct the problem Many centers use only if surgery is not possible
- 44. Speech Bulb
- 45. Speech Bulb Occludes nasopharynx when the velum is short (velopharygeal indufficiency) Aids in velopharyngeal closure Contains pharyngeal section, goes behind soft palate Can be combined with an obturator
- 47. One Researcher’s Results ‘Eighty-seven percent (39/45) of all patients increased their functional oral intake of food/liquid including 92% of stroke patients and 80% of head/neck cancer patients.’
- 50. reference
- 51. American Speech-Language-Hearing Association. (2001). Roles of Speech-Language Pathologists in Swallowing and Feeding Disorders: Technical Report [Technical Report]. Retrieved from www.asha.org/policy. doi:10.1044/policy.TR2001-00150 Mark S. Chambers, DMD, MS,a James C. Lemon, DDSb and Jack W. Martin, DDS, MS,c M.D. Anderson Cancer Center, The University of Texas, Houston, Tex Curtis TA, Beumer J. Speech, velopharyngeal function, and restoration of soft palate defects. In: Beumer J, Curtis TA, Marunick MT, editors. Maxillofacial rehabilitation: prosthodontic and surgical considerations. St. Louis: Isbiyaku EuroAmerica; 1996. p. 304-19 Taylor TD (2000) Clinical maxillofacial prosthetics. Quintessence Pub Chicago, 129-131
- 52. Thank you
Notas del editor
- A modification obturator may be used in the short-term to block a palatal fistula, for augmentation of the seal and to separate the oral and nasal cavities. An interim palatal obturator is used post-palatal surgery. This obturator aids in closing the remaining fistula and is used when no further surgical procedures are planned. It must be frequently revised. A definitive obturator is used when further rehabilitation is not possible for the patient and is intended for long-term use