Low Rate Call Girls Pune Esha 9907093804 Short 1500 Night 6000 Best call girl...
Head and neck anat fin
1. Anatomy of head and neck
By Amenu Tolera 2010
Tolera,
HEAD AND NECK
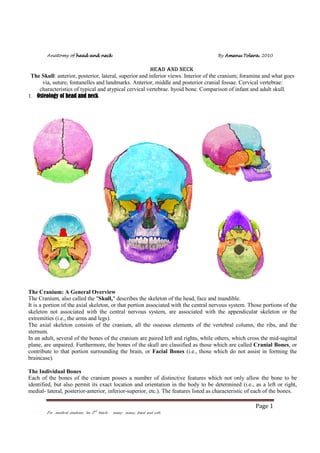
The Skull: anterior, posterior, lateral, superior and inferior views. Interior of the cranium; foramina and what goes
via, suture, fontanelles and landmarks. Anterior, middle and posterior cranial fossae. Cervical vertebrae:
characteristics of typical and atypical cervical vertebrae. hyoid bone. Comparison of infant and adult skull.
1. Osteology of head and neck
The Cranium: A General Overview
The Cranium, also called the "Skull," describes the skeleton of the head, face and mandible.
It is a portion of the axial skeleton, or that portion associated with the central nervous system. Those portions of the
skeleton not associated with the central nervous system, are associated with the appendicular skeleton or the
extremities (i.e., the arms and legs).
The axial skeleton consists of the cranium, all the osseous elements of the vertebral column, the ribs, and the
sternum.
In an adult, several of the bones of the cranium are paired left and rights, while others, which cross the mid-sagittal
plane, are unpaired. Furthermore, the bones of the skull are classified as those which are called Cranial Bones, or
contribute to that portion surrounding the brain, or Facial Bones (i.e., those which do not assist in forming the
braincase).
The Individual Bones
Each of the bones of the cranium posses a number of distinctive features which not only allow the bone to be
identified, but also permit its exact location and orientation in the body to be determined (i.e., as a left or right,
medial- lateral, posterior-anterior, inferior-superior, etc.). The features listed as characteristic of each of the bones.
Page 1
For medical students “au 2nd batch: many many, hard and soft:
2. Anatomy of head and neck
By Amenu Tolera 2010
Tolera,
1. Paired Cranial Bones: Parietals and Temporals
2. Unpaired Cranial Bones:Frontal, Occipital. Sphenoid and Ethmoid
1. Paired Facial Bones: Lacrimals, Nasals, Zygomatics, Maxillae, Palatines and the Inferior Nasal Conchae.
2. Unpaired Facial Bones: Vomer, and Mandible.
Exercise: Learn the different views of the skull as shown below.
Page 2
For medical students “au 2nd batch: many many, hard and soft:
3. Anatomy of head and neck
By Amenu Tolera 2010
Tolera,
Page 3
For medical students “au 2nd batch: many many, hard and soft:
4. Anatomy of head and neck
By Amenu Tolera 2010
Tolera,
Page 4
For medical students “au 2nd batch: many many, hard and soft:
5. Anatomy of head and neck
By Amenu Tolera 2010
Tolera,
The cranial bones
The Frontal Bone
The frontal bone may be divided into two main portions, a vertical squamous portion which articulates
with the paired parietals along the Coronal Suture and forms the forehead, and two orbital plates, which
contribute to the ceiling and lateral walls of the left and right eye orbits. On the external surface the
squamous portion frequently possesses a left and right Frontal Eminence. Additionally, the bone
possesses two Supra-Orbital Ridges (i.e., Superciliary or Brow Ridges) which are bumps above each of
the eye orbits. In early hominids these ridges formed a Torus or large shelf-like process protruding from
above the eyes. Associated with each Superior Orbital Margin of the eye orbit the frontal bone may
posses a Supra-Orbital Notch or if completely surrounded by bone, a Supra-Orbital Foramen. Above
the fronto-nasal suture which allows articulation between the frontal and nasal bones there is generally a
trace of the vertical Metopic Suture. In early life the metopic suture divided the frontal bone into left and
right halfs. With in the bone, and above and the metopic suture, is the Frontal Sinus. The left and right
Frontal Crest, begins at each Zygomatic Process of the frontal bone, and provides the anterior origin of
the Temporal Line to which the left and right temporal muscle is attached. Internally, the frontal bone
possesses the Median Sagittal (i.e., Sagittal-Frontal) Crest which separates the two frontal hemispheres
of the brain. The frontal touches, or articulates with, the following bones: Sphenoid , Parietals Ethmoid ,
Lacrimals , Nasals , Zygomatics and Maxillae.
Test yourself: The incorrect statement is:
a.
b.
c.
d.
e.
Hyoid does not articulate with any other bones
Atlas lacks a body and spine
Atlas doesn’t posses odontoid process
All skull bones doesn’t contain air cells
All cervical vertebrae posses bifid spinus process
Answer:__________?
Page 5
For medical students “au 2nd batch: many many, hard and soft:
6. Anatomy of head and neck
By Amenu Tolera 2010
Tolera,
The Parietal Bones
The Parietals are paired left and right. Externally, each possess a Superior, and Inferior Temporal Line, to which
the temporal muscle is attached. The lines run from the Frontal Crest of the anterior frontal bone to the SupraMastoid Crest on the posterior portion of the temporal bone. The parietals articulate with each other by way of the
Mid-Sagittal Suture, and with the frontal bone anteriorly by way of the Coronal Suture. These two sutures
generally form a right angle with one another. Posteriorly, the parietals articulate with the Occipital Bone by way
of the Lambdoid Suture. The intersection of the Lambdoid and Sagittal Sutures approximate a 120 degree angle
on each of the parietals and the occipital bone. Among the sutures the Lambdoid is by far more serrated than either
the Sagittal or the Coronal. Inferiorly the Parietal articulates with the temporal bone by way of the Squamosal and
Parieto-Mastoid Sutures. On the external surface near the center of the bone is the Parietal Eminence. Slightly
posterior to the eminence there may be a Parietal Foramen.
Internally, the bones possess a number of Meningeal Groves as well as perhaps some number of Arachnoid
Foveae. The groves generally branch from the inferior/anterior edge of the bone to superior/posterior, while the
foveae are frequenly found along the sagittal suture. At the area of intersection of the lambdoid and parieto-mastoid
sutures there is a brief portion of the Sigmoid (i.e., Transverse) Sulcus. The parietals touch, or articulate with, the
following bones: Occipital , Frontal , Temporal , Sphenoid and Parietals.
Test yourself: sella turcica belong to which cranial bone?
Answer:_________________?
Page 6
For medical students “au 2nd batch: many many, hard and soft:
7. Anatomy of head and neck
By Amenu Tolera 2010
Tolera,
The Occipital Bone
The Occipital Bone consists of a large squamous, or flattened portion separated from a small thick basal portion
by the Foramen Magnum on either side of which is a left or right Occipital Condyle. The occipital condyles
articulate with the first cervical vertebrae (the Atlas). Externally, the squamous portion of the bone possesses
Superior, Middle, and Inferior Nuchal Lines to which the muscles at the back of the neck are attached. The
External Occipital Protuberance lies on the superior nuchal line in the mid-sagittal plain. Lateral to each occipital
condyle are the Condylar Fossae and Foramen while the Hypoglossal Canal is medial to them.
Internally, are the Sagittal and Transverse Sulci, or grooves which converge at the Confluence of Sinuses. A
single internal Occipital Protuberance or Cruciform Eminence is also found in this area. Running inferior from
the eminence to the foramen magnum is the Internal Occipital Crest which separates the Cerebellar Fossae. The
transverse sulci assist in directing the developing jugular vein to the Jugular Notch on either side of the basilar
portion of the occipital.
The occipital touches, or articulates with, the following bones: Parietals , Temporals , Sphenoid and Atlas. The atlas
is not part of the skull. It is the first of the seven cervical vertebrae and the one upon which the base of the skull sits.
It is the bone around which the skull rotates, hence the name "atlas."
The Temporal
Page 7
For medical students “au 2nd batch: many many, hard and soft:
8. Anatomy of head and neck
By Amenu Tolera 2010
Tolera,
The Temporal Bone is another paired cranial bone which is difficult to describe due to its various features, and
projections. It consists of two major portions, the Squamous Portion, which is flat or fan-like and projects
superiorly from the other, very thick and rugged portion, the Petrosal Portion.
The squamous portion assists in forming the Squamous Suture which separates the temporal bone from the
adjacent and partially underlaying parietal bone. The petrosal portion contains the cavity of the middle ear and all
the ear ossicles; the Malleus, Incas and Stapes. This portion projects anterior and medialy beneath the skull.
Projecting inferiorly from the petrosal portion is the slender Styloid Process which is of variable length. The styloid
process serves as a muscle attachment for various thin muscles to the tongue and other structures in the throat.
Externaly the petrosal portion possesses the External Auditory Meatus while internally there is an Internal
Auditory Meatus. Anterior to the external meatus the Zygomatic Process has its origin. This process projects
forward toward the face and its articulation with the temporal process of the zygomatic. Just anterior of the external
meatus and inferior of the origin of the zygomatic process is the Glenoid or Mandibular Fossa which assists in
forming the shallow socket of the Tempro-Mandibular Joint. Posterior to the external auditory meatus is the
inferiorly projecting Mastoid Process which serves as an attachment for the sternocleidomasotid muscle. Above the
mastoid process is the Supramastoid Crest to which the posterior portion of the temporal muscle is attached.
The temporals touch, or articulate with, the following bones: Occipital , Sphenoid Parietals , Zygomatics and
Mandible .
The Sphenoid
The Sphenoid is one of the more difficult bones to describe and in vision. It has a number of features and
projections, which allow it to be seen from various views of the skull. It is a single bone that runs through the midsagittal plane and aids to connect the cranial skeleton to the facial skeleton. It consists of a hollow body, which
contains the Sphenoidal Sinus, and three pairs of projections: the more superior Lesser Wings, the intermediate
Greater Wings, and the most inferior projecting Pterygoid Processes. Internally upon the body is the Sella
Turcica where the pituitary gland rests in life. The smaller lesser wings posssesses the Optic Foramen through
which the optic or second cranial nerve passes before giving rise to the eye. The Supra-Orbital Fissure separates
the lesser wing superiorly from the greater wing below and can best be viewed on the posterior wall of each eye
orbit. The left and right greater wings assist in forming the posterior wall of each of the eye orbits where it forms an
Orbital Plate. In addition the external surface of the greater wing can be viewed in the lateral view of the cranium
in an area called the Pterion Region. Just inferior to the supra-orbital fissure near the body of the sphenoid, each of
the greater wings also possess a Foramen Rotundum which in life transmits the maxillary branch of the fifth, or
trigeminal, cranial nerve. Each of these wings also possesses a much larger Foramen Ovale more laterally, which
transmits the mandibular branch of the same nerve. More posteriorly is the smallest of the three pairs of foramena,
the Foramen Spinosum which transmits the middle meningial vessels and nerve to the tissues covering the brain.
Page 8
For medical students “au 2nd batch: many many, hard and soft:
9. Anatomy of head and neck
By Amenu Tolera 2010
Tolera,
The left and right pterygoid processes project inferiorly from near the junction of each of the greater wings with the
body of the sphenoid. These processes run along the posterior portion of the nasal passage toward the palate. Each
process is formed from a Medial and Lateral Pterygoid Plate to which the respective medial and lateral pterygoid
muscle is attached during life. The muscles run from these attachments to the internal, or medial surface, of the
mandible in the area of the gonial angle. In life the muscles assist in creating the grinding motion associated with
chewing.
The sphenoid touches, or articulates with, the following bones: Vomer , Ethmoid , Frontal , Occipital , Parietals ,
Temporals , Zygomatics and Palatines .
The Ethmoid
If the sphenoid is the most difficult cranial bone to describe and in vision, the Ethmoid is the second most difficult.
It has a number of features and projections, but unlike the sphenoid it cannot be seen from various views of the
skull. Like the sphenoid, it is a single bone that runs through the mid-sagittal plane and aids to connect the cranial
skeleton to the facial skeleton. It consists of various plates and paired projections. The most superior projection is
the Crista Galli, or Cocks Comb, found within the cranium. It assists in dividing the left and right frontal lobes of
the brain. Lateral projections from the Crista Galli are the left and right Cribriform Plates which in life cradle the
first cranial nerves i.e., the olfactory nerves. The nerves brachiate through the porosity of these plates into the nasal
cavity below. Directly inferior to the Crista Galli and running in the mid-sagittal plane is the Perpendicular Plate
of the ethmoid which articulates with the vomer more inferiorly and assists in separating the left and right nasal
passages. The Perpendicular Plate can be viewed anteriorly through the nasal cavity.
Descending off each of the Cribriform Plates is a left or right Orbital Plate which aids to form the medial wall of
the respective eye orbit. Each Orbital Plate is rectangular in shape and gives rise to two medial projections, the
Superior and Middle Nasal Concha. These projections, like the separate Inferior Nasal Concha, assist in
increasing the surface area within the nasal cavity and thereby the exposure of the brachiating olfactory nerve to
inhaled odors. The Superor or Supreme Nasal Conche are smaller, and cannot be viewed through the anterior nasal
opening because it is blocked from view by the the more inferior Middle Nasal Conche.
The ethmoid touches, or articulates with, the following bones: Sphenoid , Frontal Maxillae , Palatines , Vomer and
Lacrimals.
Page 9
For medical students “au 2nd batch: many many, hard and soft:
10. Anatomy of head and neck
By Amenu Tolera 2010
Tolera,
Facial bones
The Nasal Bones
Each of the nasal bones is a small rectangular bone which together form the bridge of the nose above the Nasal
Cavity also called the Piriform Aperture. They articulate with each other by way of the Internasal Suture and
with the frontal bone superiorly by way of the Fronto-Nasal Suture just below the glabellar region of the frontal
bone. The intersection of these two sutures marks the anatomical landmark called Nasion. Laterally, each of the
nasal bones articulates with the frontal process of the maxilla. A nasal touches, or articulates, the following bones:
Frontal , Maxilla and Nasal
The Maxillae
The Maxillae are the paired facial bones which contain the upper dention and thus form the upper jaw. Each is
basicly hollow with a large Maxillary Sinus. A superior projection, the Frontal Process, assists in forming the
lateral margin of the nasal aperture and ends by articulating with the frontal bone. An Orbital Plate forms the floor
of the eye orbit, while the Zygomatic Process articuates with the zygomatic bone. On the anteror surface of the
bone, near the maxillo-zygomatic suture, ther is an Infra-Orbital Foramen. The Alveolar Process of the Maxilla
contains the upper dentition and assists in giving rise to the Palatine Portion which forms the anterior half of the
hard palate. The left and right Maxillae articulate with one another by way of the Inter-Maxillary Suture. The
superior end of this suture frequently terminates with the Nasal Spine. A maxilla touches, or articulates with, the
following bones: Frontal , Ethmoid , Zygomatic , Vomer , Lacrimal , Maxilla , Nasal , Palatine , Mandible and
Inferior Nasal Concha .
Page 10
For medical students “au 2nd batch: many many, hard and soft:
11. Anatomy of head and neck
By Amenu Tolera 2010
Tolera,
The Zygomatic Bones
Also called the Malars or Jugals, each cheek or zygomatic bone possesses three major processes which articulate
with the bones which surround it. The Frontal Process of the zygomatic forms the lateral margin and wall of the
eye orbit and projects superiorly to articulate with the zygomatic process of the frontal bone. This portion of the
bone separates the eye orbit from the temporal fossa and possesses a posterior projecting edge called the Marginal
Process. The Temporal Process of the zygomatic runs lateral and posterior toward an articulation with the
zygomatic process of the temporal bone. Together these two processes assist in forming the zygomatic arch which
serves as the attachment for the masseter muscle in life, one of the primary muscles used in mastication. The
temporal muscle runs beneath the arch and is also a primary mover of the mandible in chewing. The Maxillary
Process of the zygomatic articulates with the zygomatic portion of the maxilla by way of the Zygo-Maxillary
Suture. The zygomatics touch, or articulate with, the following bones: Frontal , Sphenoid , Maxillae and
Temporals.
Page 11
For medical students “au 2nd batch: many many, hard and soft:
12. Anatomy of head and neck
By Amenu Tolera 2010
Tolera,
The Vomer Bone
The Vomer is a single relatively flat bone located in the mid-sagittal plane. It articulates with the perpendicular
plate of the ethmoid superiorly and together aid in forming the nasal septum. While it is frequently deflected slightly
to the left or right, in general the septum is aligned perpendicularly and divides the the nasal aperture into the the
left and right nasal passages. In addition to the Perpendicular Portion, superiorly the Vomer mushrooms out into a
pair of Alae which terminate and articulate with the sphenoid in a heart shaped process. Inferiorly the Vomer rests
on both the maxillae and the palatines. The vomer touches, or articulates with, the following bones: Sphenoid ,
Ethmoid Palatines and Maxillae .
The Palatine Bones
The Palatine Bones are paired left and right and articulate with one another in the mid-sagittal plane at the
Interpalatine Suture. Both bones assist in forming the posterior portion of the hard palate as well as a portion of
the nasal cavity. Each bone possesses a Horizontal Part, with an inferior surface which forms the posterior portion
of the hard palate and a superior surface that assists in forming the posterior portion of the floor of the nasal cavity.
The Vertical Part of each contributes to the lateral wall of the nasal cavity. Near the posterior junction of the
Vertical and Horizontal Parts on the palatal surface is a Palatine Foramen. Each bone possesses a number of
processes and articular surfaces which touch the bones that surround it. A palatine touches, or articulates with, the
following bones: Sphenoid , Ethmoid , Maxilla , Vomer and Palatine.
Page 12
For medical students “au 2nd batch: many many, hard and soft:
13. Anatomy of head and neck
By Amenu Tolera 2010
Tolera,
The Inferior Nasal Concha
The Inferior Nasal Concha is a very thin, porous, and fragile, paired bone basically elongated and curled upon
itself. It lays in the horizontal plane and is attached to the lateral wall of the nasal cavity. By way of the Maxillary
Process on the bone's lateral surface, it is attached to the maxilla, and by way of the Lacrimal, Ethmoid and
Palatine Processes to each of the bones which assist in forming the lateral wall of the nasal cavity. By projecting
into the nasal cavity, the medial surface of the Inferior Nasal Concha assists in increasing the surface area within the
cavity and thus increases the amount of mucus membrane and olfactory nerve endings exposed to inhaled odors. An
inferior nasal concha touchs, or articulates with, the following bones: Ethmoid , Lacrimal , Maxilla Palatine .
The Mandible
The Mandible or lower jaw consists to four major portions, a left and right Mandibular Ramus and the left and
right Body. The Alveolar Process of the body is that portion of the mandible which contains the lower dentition.
The junction of the ramus and the body occurs at the Gonial Angle where externally one of the masseter muscles is
Page 13
For medical students “au 2nd batch: many many, hard and soft:
14. Anatomy of head and neck
By Amenu Tolera 2010
Tolera,
attatched. The left and right masseters make up a set of two sets of muscels used in chewing. At the gonial angle on
the internal surface the Pterygoid Attachements are found. These attachements are for the medial and lateral
pterygoid muscles which assist in the grinding motion of chewing. The external surface of the mandibular body
possesses the Mental Foramen and at the midline, the Mental Protuberance or chin. The internal surface of the
body possesses the Lingual Foramen, the Mandibular Canal, and the longitudinal running Mylo-Hyoid Ridge.
The Genio Tubercle is located in the mid-sagittal plane on the internal surface of the mandible. The superior
margin of each ramus possesses both a Mandibular Condyle or Head, for articulaltion with the temporal bone at
the tempro-mandibular joint, and the Coronoid Process, for the attachement of the temporalis muscle (one in the
set of primary muscles used in mastication). The mandible articulates with each of the Maxillae by way of their
contained respective lower and upper dentition. The mandible touches, or articulates with, the following bones:
Temporals and Maxillae.
The Hyoid Bone
The hyoid is a single small "U" shaped bone in the adult which does not articulate with any other bone. It is
suspended from the styloid process of each temporal bone by means of the stylohyoid ligaments. It is located in the
mid-sagittal plane, at the front of the throat, and beneath the mandible but above the larynx near the level of the
third cervical vertebrae. It is formed from three separate parts (i.e., the Body, and the left and right Greater and
Lesser Cornu) which fuse in early adulthood. The base of the "U" shaped bone is located anteriorly while the Cornu
project posteriorly
Cervical vertebrae
Are five typical or three atypical. The typical cervical vertebrae are 3rd to 6th , has a body, vertebral foramen and
vertebral arch with pedicle, lamina, superior and inferior articular facets,trnaseverse process with foramen
transvesarium and spine. The atypical vertebrae are the 1st or atlas , the 2nd or axis and the 7th or verebra
prominens. The cervical vertebrae are easily distinguished because their spinus process is short and bifid, and the
foramen transeversarium from 6th to 1st transmit the vertebral artery and its sympathetic plexus and the vertebral
veins.
The atlas is atypical because its lacks body and has two lateral masses.the superior articular faces on on the lateral
masses are kidney shaped and articulates with occipital condyles of the skull to form atlantocipital joints. This
joint allows flexion and extension or nodding movements. The inferior articular facet on the lateral masses form
Page 14
For medical students “au 2nd batch: many many, hard and soft:
15. Anatomy of head and neck
By Amenu Tolera 2010
Tolera,
the atlantoaxial joints and This joint allow side or rotatory movements. That is we move our head saying yes by
atlantocipital and no by atlantoaxial joint.It also has anterior and posterior tubercles, articular facet for dens and
groove for 3rd part of vertebral artery.
Axis is atypical because it has a tooth like odontoid process or dens.
The vertebra prominens is so because it has long spinus process which is not bifid.
NO
1
2
3
4
Name of the foramen
In anterior cranial fossa
Cribriform foramina
Foramen cecum
Anterior ethmoidal foramina
Posterior ethmoidal foamina
Middle cranial fossa
Structures which go through it
Olifactory nerves
Occussional emissary veins from nasal mucosa to
superior saggital sinus
Anterior ethimidal VAN
Posterior ethmoidal VAN
Page 15
For medical students “au 2nd batch: many many, hard and soft:
16. Anatomy of head and neck
5
Optic canal
6
Superior orbital fissure
7
8
Foramen rotundum
Foramen ovale
9
Foramen spinosum
10
Foramen lacerum
11
Carotid canal
12
Posterior cranial fossa
Internal acoustic meatus
13
Jugular foramen
14
Hypoglossal canal
15
Foramen magnum
16
17
Condyloid foramen
Mastoid foramen
By Amenu Tolera 2010
Tolera,
1.
2.
3.
1.
Optic nerve with its meningeal sheath
Ophthalmic artery
Central vein of the retina
Occulomotor,trochlear,
ophthalmic
branch of trigeminal ,abducent nerves
2. ophthalmic veins,
3. meningeal branch of lacrimal artery
4. sympathetic nerves from plexus around
ICA.
Maxillary branch of trigeminal nerve
1. Mandibular branch of trigeminal nerve
2. accessory meningeal artery
3. lesser petrosal nerve occasionally
4. emissary veins connecting cavernous
sinus with pterygoid plexus of veins
1. Middle meningeal artery
2. Meningeal branch of mandibular nerve or
nervous spinosum
3. Posterior trunk of middle meningeal vein
1. Meningeal branch of ascending pharyngeal
artery
2. Emissary veins from cavernous sinus
1. ICA
2. Venous and symphatetic plexus around ICA
1.
2.
3.
1.
Facial nerve
Vestibulocochlear nerve
Labrynine artery
Inferior petrosal sinus and meningeal branch
of ascending pharyngeal artery in the anterior
part
2. IJV and meningeal branch of occipital artery
in the posterior part
3. Glossopharyngeal,vagus abd accessory nerves
in the middle part
1. Hypoglossal nerve
2. Meningeal branch of asending pharyngeal
artery
3. Emissary veins
1. Spinal cord with its meninges
2. Spinalaccessory
3. Vertebral arteries
4. Sympathetic plexus around vertebral artery
5. Venous plexus of vertebral canal
6. Anterior and posterior spinal arteries
Condyloid emissary veins
Meningeal branch of occipital artery
Mastoid emissary vein
In base of skull
Page 16
For medical students “au 2nd batch: many many, hard and soft:
17. Anatomy of head and neck
18
Sylomastoid foramen
19
20
Pterygotympanic fissure
Incisive foramen
21
22
Greater palatine foramen
Lesser palatine foramen
In front of the skull
Zygomaticofacial foramen
Supraorbital foramen
Inferior orbital fissure
23
24
25
26
27
28
29
30
Infraorbital foramen
Mental foramen
Nasolacrimal canal
Mandibular foramen
In the calvaria
Parietal foramen
By Amenu Tolera 2010
Tolera,
1. Exit of facial nerve fro facial canal
2. Stylomastoid branch of posterior auricular
artery
Chorda tympani of facial nerve
1. Terminal part of greater palatine vessels from
palate to nose
2. Terminal part of nasopaltine nerve from nose
to palate
Greater palatine VAN
Lesser palatine VAN
Zygomaticofacial VAN
Supraorbital and trochlear VAN
1. Zygomatic nerve
2. Orbital branch of pterygopalatine ganglion
3. Connecting veins between inferior ophthalmic
veins and pterygoid plexus of veins
Infraorbital VAN
Mental VAN
Nasolacrimal duct
Inferior alveolar VAN
Parietal emissary veins from superior saggital sinus to
occipital veins
3. Arthrology of head and neck
The joints of head and neck are either fibrous or synovial types. They include the sutures,
atlantoccipial, atlanoaxial, intervertebral , tempromandibular joints and the joints between
auditory ossicles. Just like elsewhere, this joints are reinforced by ligaments. The ligaments which
stabilize the cervical vertebrae includes anterior and posterior longitudinal, ligamentum flavum,
posterior and anterior altantoocipital membrane, transe verse, and cruciate ligaments.
The scalp and face
The scalp
Scalp is region of head which extends from inion posteriorly to eye brows anterirly and each side
of superior temporal lines laterally. The skin of the scalp continues from t he front and lateral side
of the face into the occipital region of the skull posteriorly. The makeup of the scalp is important
clinically because trauma to the scalp is frequent and it is up to the clinician to determine by
palpation and observation just how serious the trauma is.
Layers of scalp. The scalp is made of 5 layers and they spell scalp: from outer to inner are.
Page 17
For medical students “au 2nd batch: many many, hard and soft:
18. Anatomy of head and neck
By Amenu Tolera 2010
Tolera,
S – skin is with hairs and glands
C -- dense Connective tissue is the superficial fascia
A – aponeurosis or galea aponeurotica is the membraneous tendon of fleshy bellies of
occipicto frontalis muscle
4. L -- loose connective tissue is the danger area of the scalp
P -- periosteum or pericranium is the outer coverning of the bone.
1.
2.
3.
The 1st three layers of the scalp are firmly attached to each other with the dense fibrous tissue
hence in most dissection they are pulled together and commony called scalp proper.
Page 18
For medical students “au 2nd batch: many many, hard and soft:
19. Anatomy of head and neck
By Amenu Tolera 2010
Tolera,
Muscles of the scalp. It is made up of a single muscle occipitofrontalis with two bellies. The
occipital belly arises from occipital bone and insert into epicranial aponeurois. The frontal belly
arises from frontal bone and also insert into epicranial aponeurosis. Innervation is posterior
auricular branch and temporal branch of facial nerve respectively. Their action is to produce the
horizontal wrinkles seen posteriorly and anteriorly on fore head.
Neurovascular bundle of scalp and Temple
NERVE SUPPLY. The scalp has two motor and eight sensory nerves which are distributed in the
in front and behind of the auricle. Hence ten nerves are distributed to the scalp making it more
sensitive.
no
a
1
Nerves In front of auricle
Sensory nerves
Supratrochlear from V1
2
Supraorbital from V1
Zygomaticotemoral from V2
Auriculotemporal from V3
Motor nerve
Temporal branch of VII
4
5
Nerves Behind auricle
Sensory nerves
Posterior division of greater auricular, C2 and
C3 from cervical plexux
Lesser occipital, C2,C3
Greater occipital, C2 from dorsal ramus
3rd occipital C3, from dorsal ramus
Motor nerve
Posterior auricular branch of VII
BLOOD SUPPLY. Five arteries three in front and two behind the auricle supply the scalp.
These arteries form rich anastomosis.
no
Arteries
Source from
a.
in front of auricle
1
supratrochlear
Optlamic artery which comes
from ICA
2
Supra orbital
Optlamic artery which comes
from ICA
3
Superficial temporal
ECA
b.
Behind auricle
4
Posterior auricular
ECA
5
occipital
ECA
VENOUS DRAINAGE. The veins accompanying the arteries will drain as follows.
1. supratrochlear and supraorbital will unite and form anglar vein which becomes the
anterior facial vein.
2. superficial temporal vein unite posterior auricular vein and forms posterior facial vein
which is also called retromandibular vein.
3. occipital veins drain into occipital venous plexus.
Lymphatic drainage. The scalp is devoid of lymph nodes but lymphatics from the scalp will
drain into five neighboring lymph nodes of the face. lymphatics infront of the auricle drain into
submental, submandibular and parotid group of lymph nodes respectively from medial to lateral.
Lymphatics behind the auricle drain into mastoid and occipital groups of lymph nodes
respectively.
Clinical anatomy
Problem of Gaping of scalp. The blood vessels travel through the dense connective. The
connective tissue has a special relationship with the arteries in this area. When an artery is
severed, the connective tissue fibers around the vessel contract and pull the artery open. This
Page 19
For medical students “au 2nd batch: many many, hard and soft:
20. Anatomy of head and neck
By Amenu Tolera 2010
Tolera,
result is more hemorrhage than in other places. With scalp hemorrhage, compression must be
used to stop the bleeding.
High bleeding Blood vessels and nerves come into the scalp from three different regions: 1)
anterior (supraorbital), 2) lateral (superficial temporal), 3) posterior (occipital). There is free
anastomoses from side to side. With all of this blood supply, lacerations of the scalp are usually
profuse and because of the nerve supply, very sensitive.
Black eye and the Danger area of scalp. The loose connective layer of the scalp will allow
bacteria or fluid to pass freely from the posterior aspect of the scalp into the eyelids in front
causing black eye. Trauma in the back of the head can result in blood showing up in the eyelids
and should make you suspect something going on in the back of the head. Infection in this area
will also distribute to intracranial structures like the brain via parietal emissary veins, which are
valueless veins. They connect the scalp with interior like cavernous sinus passing via parietal
foramina of the skull. In brief, Emissary veins (valveless) may spread infections from the scalp to
the intracranial cavity. Normal blood flow is from inside to outside of the skull.
The face
Definition. Anterior aspect of the head from the forehead to the chin vertically, and from one ear
to the other ear horizontally.
The Skin. Has four basic features
1. Is highly vascular, hence wounds of face bleed profusely but heal rapidly and plastic
surgery is excellent on face
2. Is highly elastic and thick
3. Is rich in sebaceous and sweat glands
4. Act as attachment or insertion for muscles of facial expression
Fascia.. The superficial fascia contains muscles of facial expression, fat and neurovascular
bundles. No deep fascia except over parotid gland.
Facial musculature. Two main groups of muscle are located on the face: muscles of facial
expression innervated by the facial nerve (cranial nerve VII) because they are derived from the
2nd pharyngeal arch, and muscles of mastication supplied by the mandibular division of the
trigeminal nerve (cranial nerve V) because they are derived from the 1st pharyngeal arch.
Muscles of facial expression (innervated by the facial nerve) are superficial muscles which can
move skin and fascia in various directions. They are also dilators and sphincters for the various
orifices in the face region. The 2 major groups are around the eye and the mouth.
Around the eye: The sphincter is the orbicularis oculi which has: a palpebral part in the eye lid
(closes eye gently) and an orbital part which surrounds the orbit and blends in with the anterior
belly of occipitofrontalis (closing the eye forcibly). The orbital part causes radiating skin wrinkles
from the lateral corner of the eye.The dilator is the levator palpebrae superioris, innervated by the
oculomotor nerve (cranial nerve III) and postganglionic sympathetic fibers from the superior
cervical ganglion.
Around the mouth: The sphincter is the orbicularis oris , which closes the lips but can also
protrude the lips as in whistling, or kissing.The dilators are: Levator labii superioris alaeque nasi ,
Levator labii superioris , Levator anguli oris , Zygomaticus minor , Zygomaticus major , Platysma
, Depressor anguli oris , Depressor labii inferioris and Mentalis. The buccinator is the main
Page 20
For medical students “au 2nd batch: many many, hard and soft:
21. Anatomy of head and neck
By Amenu Tolera 2010
Tolera,
muscle of the cheek and it keeps the cheeks in contact with the gums so that food does not
accumulate in the vestibule of the mouth.
Neurovascular bundles of the face
The sensory nerves of the face are the 11 terminal branches of the three divisions of the
trigeminal nerve (cranial nerve V). Motor are facial for all muscles of facial expression and
Motor branches of V3.
no
nerves
Nature and distribution
a
Sensory nerves from V1
Is purely sensory
1
supratrochlear
All are distributed to
2
3
supraorbital
Lacrimal
The area of the face developed
4
infratrochlear
From frontonasal eminence from anterior to
posterior
"
5
external nasal
"
6
7
8
Maxillary division (V2)
zygomaticotemporal
zygomaticofacial
infraorbital
Mandibular division (V3)
Is purely sensory
All are distributed area of the face derived from
maxillay eminence from posterior to anterior
auriculotemporal
bucal
mental
Motor nerve
Facial with five
branches
Temporal branch
Zygomatic branch
Bucal branch
Mandibular branch
Cervical branch
trigeminal
All are distributed area of the face derived from
mandibular eminence from posterior to anterior
9
10
11
12
a
b
C
d
e
13
Is mixed
terminal All mm. of facial expression
Occipitofrontalis and etc.
Zygomaticus and etc.
Baccinator and etc.
Mentalis,derpssor labi inferoris etc.
Platysma in the neck
All mm. of mastication
Blood supply. The face gets blood supply from two major sources . Ophthalmic arteries from
ICA give supraorbital and supratrochlear arteries. Facial artery and superficial temporal arteries
from ECA will also supply the face via their branches.
The facial artery: provides the main blood supply. passes over the lower border of mandible at
the anterior border of the masseter (feel the pulse). has a tortuous course to allow for movement
of the face, first to the angle of the mouth and then up at the side of the nose to the medial angle
Page 21
For medical students “au 2nd batch: many many, hard and soft:
22. Anatomy of head and neck
By Amenu Tolera 2010
Tolera,
of the eye. gives off upper and lower labial branches as well as numerous other branches to the
face. Free anastomoses on the same side as well as across the midline
The superficial temporal artery is a smaller terminal branch of the external carotid artery. Its
pulse can be felt in front of the tragus of the ear. Above the ear it divides into anterior and
posterior branches. It anastomoses with the facial artery.
The facial vein has a straighter path and communicates with deeper veins such as veins of the
orbit (leading to the cavernous sinus within the skull; at the medial angle of the eye and the
pterygoid venous plexus. The central face area is thus a "danger area" for an infection on the face
to travel into the skull or into the deep face.
The retromandibular vein is formed in the parotid gland by the union of the maxillary and
superficial temporal veins, emerges from the gland near the angle of the mandible divides into
twowith the anterior branch or division joining the facial vein and draining into the internal
jugular vein, the posterior branch or division joins with the small posterior auricular vein to
form the external jugular vein.
Lymphatic drainage. Lymphatic from the the five groups of lymph nodes drain into superficial
or deep cervical groups of lymph nodes.
Clinical anatomy
Bell's Palsy: Lesions of the facial nerve (Cranial nerve VII). Drainage of tears and dribbling of saliva due
to paralysis of the two main orbicularis muscles. Paralysis of buccinator will lead to accumulation of food
in the vestibule. Test by asking patients to screw up the eye (loss of muscle tone causes the normal skin folds
to disappear on the side of the lesion), to smile or to whistle. Muscles must be supported during recovery or
they will stretch under gravity and cause a permanent asymmetry of the face.
Unilateral facial muscles paralysis Test:
1) For loss of taste in the anterior 2/3 of tongue for the integrity of the chorda tympani.
2) For hyperacusis to test the integrity of the nerve to stapedius.
3) For lack of lacrimation on one side for the integrity of the greater (superficial) petrosal nerve.
If this is present, it will result in dessication of cornea, ulceration and blindness. Dessication of
cornea will result in pain sensation carried by V1.If all 3 signs are present then the lesion is
between the brainstem and the geniculate ganglion. Bell's palsy usually affects only branches of
the facial nerve (VII) below the stylomastoid foramen.
Danger area or triangle of the face. The facial vein is important clinically because it has a direct
connection to the ophthalmic vein and then to a deep venous sinus within the cranial cavity, the
cavernous sinus causing thromboplebitis of it. Bacteria or infectious agents can enter the facial
vein and gain access to internal cranial structures resulting in infection there. This is probably the
reason why our mothers always said not to squeeze our pimples.
The lacrimal apparatus is an apparatus which drains tears from the galand to inferior meatus of
the nose. It is made up of
1.
2.
3.
4.
The lacrimal gland and its ducts
conjectival sac
lacrimal punctum and lacrimal canaliculi
lacrimal sac
Page 22
For medical students “au 2nd batch: many many, hard and soft:
23. Anatomy of head and neck
By Amenu Tolera 2010
Tolera,
5. nasolacrimal duct
Blood supply. is from ophthalmic artery
Venous drainge. ophthalmic veins
Nerve supply. lacrimal nerve
This nerve has both sensory and secretomotor fibers. Secretomotor fibers begin in lacrimatory
nuclus of CNVII . See pterygopalatine ganglion.
Facial nerve. Is the 7th cranial nerve which arises as four nuclei in the brain stem from
1.
2.
3.
4.
the motor muscles which is branchiomotor
the superior salivatory nucleus which is parasympathetic
lacrimatory nucleus which is also parasympathetic
nucleus of tractus solitarius which is gustatory
This nerve enters the internal acoustic meatus and goes via facial canal by forminging geniculate
ganglion via strylomastoid formaen.
It gives three branches in the facial canal these are the greater petrosal, nerve tostapedius
and chordatympani. It gives also gives three branches as just it exit from stylomastoid
foramen,these are posterior auricular nerve to occipitalis, nerve to sytlohyoid and
posterior belly of digastric. It finally gives five terminal glands in the substance of the
parotid gland. These are top to bottom are temoral, zygomatic, buccal, mandibular and
cervical.
THE TEMPORAL AND INFRATEMPORAL REGIONS
Temporal fossa : Lies on the side of the skull between temporal lines and zygomatic arch. It is
continuous with infratemporal fossa below the arch.
The INFRATEMPORAL TEMPORAL FOSSA
Lies Inferior to the temporal fossa and zygomatic arch and deep to the ramus of the mandible. It
stretches from the parotid fascia posterior to the mandibular ramus to the tuberosity of the
maxilla.
Walls. The lateral wall is formed by the medial aspect of ramus of the mandible. The anterior
wall is formed by the: Body and tuberosity of the maxilla, deep to zygoma and zygomatic process
of the maxilla. The pterygomaxillary fissure may be seen in the medial aspect of this anterior
wall, opening into the more medial pterygopalatine fossa. The inferior orbital fissure may also
be seen. Inferior to the pterygomaxillary fissure is the hamulus serving as attachment point for
the pterygomandibular raphé. It serves as the common site of origin for the buccinator and the
superior constrictor muscle and runs from the hamulus to the upper 1/5 of the mylohyoid line.
The medial wall is formed by the: lateral pterygoid plate, superior constrictor muscle, levator and
tensor palati muscles.
Page 23
For medical students “au 2nd batch: many many, hard and soft:
24. Anatomy of head and neck
By Amenu Tolera 2010
Tolera,
The roof of the infratemporal fossa is formed by: the greater wing of the sphenoid anteriorly
and the squamous portion of the temporal bone posteriorly. The infratemporal crest is on the
anterior aspect of the undersurface of the greater wing of the sphenoid and serves as an
attachment site for the upper head of the lateral pterygoid. Posterior to this infratemporal crest
are:The foramen ovale for transmission of V3 and the lesser petrosal nerve (from IXth) from the
middle cranial fossa to the infratemporal fossa. The foramen spinosum for transmission of the
middle meningeal artery from the infratemporal fossa to the middle cranial fossa.
Contents of the infratemporal fossa
1. Four Muscles of Mastication
Action
Nerve
Supply
closes mouth
muscular
branch (V3)
Muscle
Origin
Insertion
masseter
zygomatic arch
ramus &
mandible
medial
pterygoid
medial surface of lateral medial
surface
of
closes mouth and helps muscular
pterygoid plate and maxillary ramus and angle of
protrude mandible
branch (V3)
tuberosity
mandible
lateral
pterygoid
upper head: greater wing of upper head: articular
open
and
protrudes
sphenoid
disc
muscular
mandible, moves mandible
lower head: lateral surface of lower head: neck of
branch (V3)
side to side
lateral pterygoid plate
condyle
angle
of
Page 24
For medical students “au 2nd batch: many many, hard and soft:
25. Anatomy of head and neck
temporalis
temporal fossa
By Amenu Tolera 2010
Tolera,
coronoid process and
muscular
anterior border of closes and retracts mandible
branch
ramus
Note. All muscles of mastication are innervated by mandibular division of trigeminal nerve,
why?
2. Maxillary artery and its branches
The maxillary artery lies lateral to the lateral pterygoid muscle. Arise from from the external
carotid artery as a larger terminal branch in the parotid gland, the artery enters the posterior
aspect of the infratemporal fossa by passing deep to the neck of the mandibular condyle. It
crosses the lateral side of the lateral pterygoid muscle and enters the pterygomaxillary fissure. It
is divided into a first or mandibular part, second or pterygoid part and third or
pterygopalatine part. The mandibular and pterygoid parts are associated with the infratemporal
fossa and the pterygopalatine part is associated with the deep face and the nasal region that is
pterygopaltine fossa
The mandibular portion of the maxillary artery has 5 branches, all entering a canal:
The middle meningeal artery is the principal artery to periosteal dura of the cranial cavity. It is
clinically important artery of epidural heamatoma. It has two divisions.
Page 25
For medical students “au 2nd batch: many many, hard and soft:
26. Anatomy of head and neck
By Amenu Tolera 2010
Tolera,
The inferior alveolar artery runs into the mandibular foramen and supplies the teeth and the
mandible. The angle of the mandible is poorly supplied and may suffer from alveolar osteitis (dry
socket). The deep auricular artery supplies the auditory meatus .The anterior tympanic artery
accompanies the chorda tympani through the petrotympanic fissure to reach the middle ear. The
accessory meningeal branch (inconsistent) enters the foramen ovale and supplies the trigeminal
ganglion and the surrounding dura.
The pterygoid portion of the maxillary artery has 4 branches supplying muscles of mastication
in the infratemporal fossa: 2 deep temporal branches, a masseteric branch, a pterygoid branch,
and a buccal branch.
The pterygopalatine portion of maxillary artery has 6 branches supplying the deep face, teeth
and nasal region. Posterior superior alveolar, infraorbital, greater palatine, pharyngeal artery of
pterygoid canal, Sphenopaltine arteries, which is the terminal branch of maxillary artery.
3. The pterygoid plexus of veins follows the maxillary artery in the infratemporal fossa, lying
mostly lateral to the artery. This is a route for infection: the veins have connections with the
cavernous sinus via the deep facial, inferior ophthalmic and emissary veins in the sphenoid bone.
Veins of the head have NO valves. That is pterygoid plexus communicates with :
Page 26
For medical students “au 2nd batch: many many, hard and soft:
27. Anatomy of head and neck
By Amenu Tolera 2010
Tolera,
a. inferior ophalmic vein via inferior orbital fissure
b. cavernous sinus via emissary veins
c. facial vein via deep facial vein
4. Mandibular division of the trigeminal nerve with its branches
The trigeminal nerve (CN V)
The trigeminal nerve lies in the floor of the middle cranial fossa, on the petrous temporal bone. It
forms the trigeminal ganglion from which its three branches diverge. The mandibular nerve
passes out of the skull through the foramen ovale. It is a sensory nerve to the skin over the
mandible, the mandibular teeth, tongue and floor of the mouth, and motor to the muscles of
mastication, the mylohyoid, tensor tympani and palati and the anterior belly of digastric. The
lingual branch of the mandibular carries taste fibres for the anterior two-thirds of the tonge. These
taste fibres originate in the facial nerve as the chorda tympani. The maxillary nerve passes along
the lateral wall of the cavernous sinus to leave the skull through the foramen rotundum in the
sphenoid bone. The nerve is entirely sensory and innervates the skin over the maxilla, the
maxillary teeth, the mucous membrane of the nose and maxillary sinus, and the palate. The
ophthalmic nerve passes along the side of the cavernous sinus to pass into the orbit through the
superior orbital fissure. The nerve supplies sensory fibres to the cornea, eyelids, mucous
membrane of the air sinuses and nasal cavity, and the skin on the nose. Direct injuries due to
fractures of the base of the skull and penetrating objects are the two main causes of injury to the
trigeminal ganglion. The ophthalmic and infraorbital nerves may be injured in trauma to the face.
The mandibular division is rarely injured except for its inferior alveolar nerve in cases of
mandibular fracture.
Page 27
For medical students “au 2nd batch: many many, hard and soft:
28. Anatomy of head and neck
By Amenu Tolera 2010
Tolera,
Mandibular nerve is the only mixed modality of trigeminal nerve which goes via foramen
ovale. It is organized into main trunk, a larger posterior and a smaller anterior divisions.
From the common main trunk: It gives one sensory branch is meningeal branch called nervous
spinosum and one motor to medial pterygoid muscle. The branch to this muscle also supplies
tensor veli paltini and tensor tympani.
From the smaller Anterior Trunk it gives one sensory, The buccal nerve and three motor ,
Masseteric branches , Posterior and anterior temporal branches to the temporalis muscle and The
nerve to the lateral pterygoid.
The buccal nerve of V3: passes between the 2 heads of the lateral pterygoid muscle. Continues
into the cheek on the lateral surface of the buccinator muscle. Is the terminal branch of the
anterior division is sensory to the mucosa of the inside of the cheek and the lower gums around
the molar teeth. Does not supply the motor innervation of the buccinator.
From the larger Posterior trunk: it gives three sensory, the Auriculotemporal nerve, lingual ,
Inferior alveolar (dental) nerve and one motor branches nerve to mylohyoid which also supplies
the anterior belly of digastric as well..
Auriculotemporal nerve: Arise as two roots and leaves V3 just inferior to the foramen ovale and
projects posteriorly in the infratemporal fossa parallel to the roof. The initial segment encircles
the middle meningeal artery as the artery ascends to enter the foramen spinosum and receives
postganglionic parasympathetic fibers from the otic ganglion which are secretomotor to the
parotid gland. Passes medial to the head of the mandibular condyle and sends a sensory branch to
the TMJ. Enters the deep portion of the parotid gland giving sensory branches as well as
parasympathetic postganglionic fibers from the otic ganglion. Its terminal portion accompanies
the superficial temporal artery and innervates the upper half of pinna of the ear and part of the
temporal region (Pain and general sensation).
Inferior alveolar (dental) nerve. From the foramen ovale to the mandibular foramen on the
medial aspect of the ramus of the mandible, lying between the medial and lateral pterygoid
muscles and just posterior to the lingual nerve . The branch to mylohyoid and to the anterior belly
of the digastric is the only branch in the infratemporal fossa. It first lies in the mylohyoid
groove, and then on the inferior aspect of the mylohyoid to reach the digastric muscle . The
portion of the inferior alveolar nerve in the ramus of the mandible is entirely sensory to lower
teeth, lower gums and the mucosa of the lower lips. It exits the mandible as the mental nerve to
innervate the mucosa and gum adjacent to the lower lip.
Lingual nerve. Lies anterior to the inferior alveolar nerve and remains medial to mandible.
Receives the chorda tympani in the infratemporal fossa. The chorda tympani reaches the
infratemporal fossa via the petrotympanic fissure . The chorda tympani contain preganglionic
parasympathetic secretomotor fibers of VII from the tympanic plexus and special sensory fibers
for taste from the anterior 2/3 of the tongue. The taste fibers have their cell bodies in the
geniculate ganglion of VII. Terminal distribution of the lingual nerve and associated fibers which
mediate general sensation (pain, touch temperature and pressure) is to the floor of the mouth and
the anterior 2/3 of the tongue.
Clinical Anatomy. Mandibular nerve block technique: Injection of anesthetic is performed in
the fascial compartment defined by the fascial covering of the medial pterygoid and the medial
Page 28
For medical students “au 2nd batch: many many, hard and soft:
29. Anatomy of head and neck
By Amenu Tolera 2010
Tolera,
aspect of the ramus of the mandible. The anesthetic diffuses to the lingual and inferior alveolar
nerves.
5. Temporomandibular joint (TMJ; is an articulation between head of mandible and
Mandibular fossa and articular tubercle of the temporal bone Synovial joint with intraarticular
disc dividing joint into a lower compartment (hinge rotation for mandibular head) and upper
compartment (sliding joint for protrusion). Minor supportive elements of the TMJ are : Lateral
temporomandibular ligament (thickening of the joint capsule , Stylomandibular ligament
(between parotid and submandibular glands; Sphenomandibular ligament. Movements of the
mandible: Elevation, Depression, Protrusion and Retraction and side to side movements.
Which muscle does these movements?
Pterygopalatine or sphenopalatine fossa
Is the fossa which lies between pterygoid plate, body of sphenoid bone and maxilla. It has five
communications
1. Anteriorly: with orbit via inferior orbital fissure
2. posteriorly: with middle cranial fossa via foramen, pterygoid canal via foramen lacerum
and pharynx with via palatovaginal canal
3. Medially: with nose via sphenopalatine foramen
4. Laterally: with infratemporal fossa via pterygomaxillary fissure
5. Inferiorly: with the oral cavity via greater and lesser palatine nerves.
The major contents of pterygopalatine fossa are
1. 3rd part of maxillary artery with its six branches
2. Maxillary nerve with its eight branches. This include zygomztic with its
zygomaticotemporal and zygomaticotemporal nerves, posterior superior alveeolar,
anterior superior alveolar, middle superior alveolar, infraorbital and the three terminal
branches palpebral, nasal and labial branches.
3. Pterygopalatine ganglion: is a parasympathetic ganglion supplies the lacrimal gland and
gland of nose, palate and pharynx. Its preganglionic fibers arise from superior salivatory
nucleus of lacrimation of CN VII via greater petrossal nerve with nerve of the
pterygoid canal forms pterygopalatine ganglion. Postganglionic fibers supply
secretomotor nerves to lacrimal gland and mucous gland of the nose, paranasal sinuses,
palate and nasopharynx. The sympathetic are from superior cervical ganglion around
internal carotid plexus as deep petrosal forms nerve of the pterygoid canal as
pterygopaltine ganglion .This fibers does not synapse in the ganglion but pass to supply
vasomotor innervation to mucus membrane of nose, paranasal sinus, palate and
nasophynx. The sensory root comes from maxillary nerve and pass via the ganglion
without synapse.
Page 29
For medical students “au 2nd batch: many many, hard and soft:
30. Anatomy of head and neck
By Amenu Tolera 2010
Tolera,
ANATOMY OF THE NECK
Definition: it part of a body that lies between the head superiorly and the thorax inferiorly. It
is bounded by: superior nuchal line, posterior and anterior mid saggital plane, mandibular
margin and superior border of the clavicle.
.
Skin: is just like other parts of the body unlike that of the skin of the face
Superficial fascia: Contains platysma and sternocliedomastoid muscles, neurovascular bundles
and lymph nodes.
Deep fascia: (see cross section of neck):Is portioned into six fascia to ensheath structures of the
neck. It includes:
1. Superficial (investing) layer of deep cervical fascia-surrounds all of the deeper parts of the
neck and splits to enclose the platysma and SCM muscles. Is attached superiorly along the
mandible ,mastoid process, EOP, and superior nuchal line of the occipital bone. Is attached
inferiorly along the acromion of sacpula, clavicle and manubrium of sternum
2. prevertebral layer of deep cervical fascia: Is cylinderical and encloses the vertebral column
and its associated muscles. Covers the scalene muscles and deep muscles of the back. Attached
to EOP and basilar part of the occipital bone and becomes continous with the endothoracic fasica
and anterior longitudinal ligament of the bodies of vertebra in the thorax
3. Carotid sheath: is formed by thickening of deep fascia to enclose the common carotid
arteries, vagus nerve , internal jugular vein, deep cervical lymph nodes and some times ansa
cervicalis. It doesn't contain the sympathetic trunk which lies posterior to carotid sheath and
anterior to prevertebral fascia.
Blends with the prevertebral,pretracheal,and investing layers and also to the base of the skull.
4. Pretracheral layer of deep cervical fascia
Invests larynx and trachea,enclosingthe tyroid gland,and contributing to the formation of carotid
sheath.
Attaches superiorly to the thyroid andcricoid cartilagesand inferiorly to pericardium
5. Buccopharyngngeal fascia
Page 30
For medical students “au 2nd batch: many many, hard and soft:
31. Anatomy of head and neck
By Amenu Tolera 2010
Tolera,
Covers the buccinator muscles and the pharynx. Is attached to pharyngeal tubercle and
pterygomandibular raphe.
6. Pharyngobasilar fascia
Is fibrous coat in the wall of the pharynx , situated between the mucus membrane and the
pharyngeal constrictor muscles.
Muscles of the neck
In the anterolateral aspect of the neck there are ten muscles: two superficial, four suprahyoid and
four infrahyoid
The two superficial muscles
muscle
origin
insertion
action
innervations
Page 31
For medical students “au 2nd batch: many many, hard and soft:
32. Anatomy of head and neck
Platysma:
By Amenu Tolera 2010
Tolera,
fascia or skin inferior border tenses the skin of the neck & draws facial nerve
over
of mandible or corner of mouth
skin of lower
pectoralis
face
majoror
deltoid
muscles
Sternocleidomastoid sternum and mastoid
flex forward the neck when both accessory nerve
clavicle.
process of the sides contract
(CNIX)
skull
The four suprahyoid muscles
muscle
origin
Digastric
inferior
border
mandible
insertion
action
hyoid bone
open mouth and elevate trigeminal (anterior belly) &
hyoid bone
facial nerves (posterior belly)
of
innervation
body
of elevate hyoid bone and trigeminal nerve
of hyoid bone floor of mouth
Mylohyoid
inferior
border
mandible
Stylohyoid
Styloid process body
of elevate & retracts tongue
of
the hyoid bone
temporal bone
facial nerve
geniohyoid
genial tubercle body
hyoid
1st cervical nerve
of depresses mandibel
The four infrahyoid muscles
Page 32
For medical students “au 2nd batch: many many, hard and soft:
33. Anatomy of head and neck
By Amenu Tolera 2010
Tolera,
Strenohyoid:-
manubrium body
bone
of
hyoid : depress hyoid bone
Sternothyroid:
manubrium thyroid cartilage depress thyroid cartilage
Thyrohyoid
thyroid
cartilage
Omohyoid
superior
border
scapula
great cornu
hyoid bone
ansa cevicalis
ansa cevicalis
of depress hyoid bone & elevate C1 nerve
thyroid
inferior border of depress hyoid bone
of hyoid bone
ansa cevicalis
Approaches to the neck anatomy
Is best described by dividing into 2 major and 6 minor triangular regions using
sternocliedomastoid, omohyoid and digastric muscles on the anterolateral aspect. Posteriorly
there is also suboccipital triange.
Two major are one infront and the other behind SCM.
Triangles of neck
Page 33
For medical students “au 2nd batch: many many, hard and soft:
34. Anatomy of head and neck
By Amenu Tolera 2010
Tolera,
Six minor triangles are: occipital and subclavian triangles of posterior triangles separated by
omohyoid posterior belly. Submandibular, submental,carotid and muscular triangles of anterior
triangle separated by omohyoid anterior belly,digastric anterior and posterior bellies and hyoid
bone.
Define the boundary, roof, floor, main contents of each triangle and description of each
content
as well as applied anatomy of each triangle.
What are the boundaries the anterior and posterior triangles of the neck and the boundaries of
minor triangles of the neck?
The borders of posterior triangle are:
1. Posterior border of sternocliedomastoid: anterior border
2. Anterior border of trapezius: posterior border
3. Intermediate third of clavicle: inferior border
The borders of anterior triangle are:
1. Anterior border of sternocliedomastoid: posterior border
2. Base of mandible: superior border
3. Midline of the neck: anterior border
The borders of SUBMANDIBULAR TRIANGLE are
1. Posterior belly of Digastric: Lateral border
2. Anterior belly of Digastric: Medial border
3. Mandible: Superior borderBorders:
The borders of CAROTID TRIANGLE are
1. Superior Belly of the Omohyoid: Medial Border
2. Posterior Belly of the Digastric: Superior Border
3. Sternocleidomastoid: Lateral Border
The borders of MUSCULAR TRIANGLE:
1. Superior Bellies of the Omohyoid: Lateral borders
2. Midline of the neck: Medial borders
The borders of SUBMENTAL triangle are:
1. Anterior belly of digastric: right border
2. Posterior belly of digastric: left border
3. Hyoid bone : inferior border
The roof of every triangle of the neck are
1. The skin
2. The superficial fascia with its contents.
The floor every triangle of the neck is made up of muscles
1. The floor of posterior triangle is made of above downwards: semispinalis capitis, splenius
captis, lavator scapula and scalenus medius.
2. The floor of carotid triangle is made of hyoglossus, thyrohyoid, and middle and inferior
constrictor of the pharynx.
3. The floor of submental triangle is made of mylohyoid muscle
Page 34
For medical students “au 2nd batch: many many, hard and soft:
35. Anatomy of head and neck
By Amenu Tolera 2010
Tolera,
4. The floor of digasric triangle is made up of mylohyoid and hyoglossus
5. The floor of muscular triangle is made of sternohyoid, sternothyroid and thyrohyoid.
The contents of the triangle are mainly neurovascular structures, glands and muscles.
The contents of posterior triangle are:
1. vessels like the 3rd part of subclavian artery, transeverse cervical and suprascapular
vessels and external jugular vein.
2. nerves like the three trunks of brachial plexus, branches of cervical plexus and the spinal
accessory nerve.
3. lymph nodes like deep and superficial cervical lymph nodes.
The contents of carotid triangle are:
1. vessels like common carotid artery and its branches and internal jugular vein
2. nerves like vagus , sympathetic trunk , ansa cervicalis and part of hypoglossal nerve
3. lymph nodes like deep cervical lymph nodes accompanying internal jugular vein
The contents of digastric triangle are:
1. vessels like a part of facial artery and anterior facial vein
2. nerves like a part of hypoglossal nerve
3. lymph nodes like submandibular lymph nodes
4. gland like submandibular gland.
The submental triangle are:
1. vessels like submental artery and vein
2. lymph nodes like submental lymph nodes
The contents of muscular triangle are>
1. muscles like infrahyoid muscles
Clinical Anatomy: DANGER triangle of the neck : That part of the posterior triangle inferior
to the Spinal Accessory Nerve. It contains: The Spinal Accessory Nerve (XI) and Brachial
Plexus. Hence injury to this nerves cause a lot of syndromes.
Give a short account on the major contents of each of the triangles?
1. The Cervical plexus
Formation: The ventral primary rami of upper four spinal nerves ( C1, C2, C3, and C4) form a
network of nerves known as the cervical plexus. There is some contribution to the plexus from
C5. This plexus just like any other plexus gives branches.
Branches: It has four cuntanous and five muscular branches. The cutanous branches are:
1. lesser occipital nerve (C2)
2. Greater auricular nerve (C2 and C3)
3. transeverse cervical nerve(C2 and C3)
4. supraclavicular nerves( C3 and C4).
The muscular branches are:
1. nerve to sternocliedomastoid (C2)
2. nerve to trapezius (C3 and C4)
3. nerve to levator scapula (C3 and C4)
4. nerve to diaphragm, the phrenic nerve(C3,C4 and C5)
5. nerve to infrahyoid muscles, the ansa cervicalis ( C1, C2 and C3)
Page 35
For medical students “au 2nd batch: many many, hard and soft:
36. Anatomy of head and neck
By Amenu Tolera 2010
Tolera,
2. The ansa cervicalis
Formation: is a nerve loop formed in the neck by union descendsens hypoglossi or the superior
root (C1) and descendens cervicalis or the inferior root(C2 and C3).
Distribution: It lies inside or infront of the carotid sheath and supplies all infrahyoid muscles
except thyohyoid, which is supplied by C1 via hypoglossal fibers. Draw the ansa cervicalis ?
3. The Accessory nerve
The spinal accessory nerve is the motor nerve to the sternocleidomastoid and trapezius muscles .
It arise by two roots. The cranial root arises from nucleus ambigus in the medulla and the spinal
root from the upper five cervical spinal segments of the spinal cord. The spinal root ascends in the
vertebral canal reaching the cranial cavity via foramen magnum. The two roots merge in the
jugular foramen and again split below the jugular foramen. The cranial accessory joins vagus
nerve and distribute with its pharyngeal and laryngeal branches. This tells you why it is so named.
The spinal accessory descends in the neck in the neck crossing internal jugular vein , passes deep
to styloid process,posterior belly of digastric and occipital artery. Then passes deep to
sternocliedomastoid supplying it and crosses the posterior triangle and then passes deep to
trapezius supplying it. NERVE GRAFTS: The function of Spinal Accessory is somewhat
redundant.
Clinical anatomy: accessory nerve can be used to replace innervation lost by other muscles. The
nerve can be redirected to the muscles of facial expression, e.g., and patients can learn to use the
new pathway with physical therapy.
Page 36
For medical students “au 2nd batch: many many, hard and soft:
37. Anatomy of head and neck
By Amenu Tolera 2010
Tolera,
4. Carotid sheath
A protective deep fascia which encloses larger neurovascular structures of the neck in the carotid
triange. It contains common carotid artery and its branches more medially, internal jugular vein
more laterally with its accompanying lymph nodes, and vagus nerve in the middle between the
two. Some times it also contains ansa cervicalis. The sympathetic trunk lies posterior to the
sheath.
5. The Common carotid arteries.
Page 37
For medical students “au 2nd batch: many many, hard and soft:
38. Anatomy of head and neck
By Amenu Tolera 2010
Tolera,
They arise from arch of aorta on the left and from brachiocephalic trunk on the right. Each
carotid artery ascends the neck in a connective tissue sheath which encloses the vagus nerve and
the internal jugular vein. The internal jugular vein lies lateral to the common carotid artery with
the vagus nerve in between. At the upper border of the thyroid cartilage the common carotid
arteries divide to form the internal and external carotid arteries . Just at bifurcation point there is
carotid body, which is a chemoreceptor, innervated by nerve to carotid body and sinus from
CNIX and CNX. At the beginning of the internal carotid there is a dilation called carotid sinus,
which is a baroreceptor, innervated by branches of vagus and glossopharyngeal nerves.
The external caroid artery: Have six side and two terminal branches in the neck. This are
ascending pharyngeal, superior thyroid, facial, lingual, posterior auricular and occipital arteries as
side branches and superficial temporal and maxillary as terminal branches. The external carotid
arteries supply the muscles of the neck, the pharynx, larynx, thyroid, ears, mouth, nose, face and
scalp. The named side branches are:
3 anterior branches
1. Superior Thyroid Artery -- Thyroid gland and part of anterior neck
2. Lingual Artery -- to tongue
3. Facial Artery---to face
1 medial branch
4. Ascending Pharyngeal Artery -- to pharynx
2 posterior branches
5. Occipital Artery -- back of neck and behind ear
6. Posterior Auricular Artery -- behind and around ear
SUPERFICIAL TEMPORAL ARTERY: IS the smaller terminal branch of the External Carotid
artery .Goes straight up the temporal region of the skull. Has three named branches:
Anesthesiologists use it to take a pulse. It is found just anterior to the ear, superficial to the
zygomatic arch.
1. Frontal Branch
2. Parietal Branch.
3. Transverse Facial Artery crosses Masseter muscle
Page 38
For medical students “au 2nd batch: many many, hard and soft:
39. Anatomy of head and neck
By Amenu Tolera 2010
Tolera,
The internal carotid artery: has no branch in the neck. It vertically ascends and enters into the
skull via carotid canal. Then it has tortous course and gives numerous branches as well. The
internal carotid artery ascends to the base of the skull which it enters through the carotid canal.
Entering the skull the artery passes anteriorly across the foramen lacerum and through the
cavernous sinus. Emerging from the cavernous sinus the artery terminates by dividing into the
anterior and middle cerebral arteries. There are no branches from the cervical part of the internal
carotid. The ophthalmic artery is the largest of its intracranial branches leaving at the emergence
from the cavernous sinus and entering the orbit by the optic canal to supply all of the structures of
the orbit. Smaller branches also arise fro the internal carotid arery as it passes through the skull.
These branches supply the meninges, the trigeminal ganglion, the pituitary gland, and the
tympanic cavity.
Page 39
For medical students “au 2nd batch: many many, hard and soft:
40. Anatomy of head and neck
By Amenu Tolera 2010
Tolera,
7. The jugular veins
The internal jugular vein: is a continuation of sigmoid sinus at jugular foramen. It has two
bulbs, the superior bulb and the inferior bulb. Between the bulbs it has tributaries like inferior
petrosal sinus, superior and middle thyroid veins, common facial vein, and anterior jugular vein.
It descends in the neck and joins its corresponging subclavian vein forms the corresponding
brachiocephalic veins.
External jugular vein: is formed by union of posterior auricular vein and posterior division of
retromndibular vein. It has tributaries like suprsacpularveins, transeverse cervical vein and
anterior jugular vein. It descends in the neck anterior to SCM muscle and drain into its
corresponding subclavian vein. Sometimes it may drain into internal jugular vein.
Submandibular region
Position : area between mandible and hyoid bone
Contents: muscles like, stylohyoid, myleohyoid, geniohyoid, styloglosus, genioglossus,
hyoglossus and digastric. Glands like sumandibular and sublingual salivary glands which are
innervated by parasympathetic-chorda tympani from facial nerve and sympathetic –from superior
cervical ganglion via plexus on facial artery. General sensory from lingual from mandibular
division of trigeminal nerve. vessels like facial and Submandibular ganglion on hyoglossus
muscle. Lymph nodes like submandibular lymph nodes which receive from submental lymph
nodes and lymph from anterior 2/3 of the tongue, ½ of nasal wall, Lips and Paransal sinus
The Salivary glands
Page 40
For medical students “au 2nd batch: many many, hard and soft:
41. Anatomy of head and neck
By Amenu Tolera 2010
Tolera,
1. Submandibular gland
Is ensheathed by investing layer of the deep cervical fascia . Lies in submandibular triangle
Its supericial portion is located superficial to mylohyoid muscle. Its deep portionis located
betweenthe hyoglossus and styloglossus muscles medially and mylohyoid muscle laterally and
between lingual nerve above and hypoglossal nerve below. Whartons duct arise from the deeper
portion and runs foreward between the mylohyoid laterally and and hyoglossus laterlly , where it
is crossed laterally by the lingual nerve.then it runsbetween sublingual gland and and the
genioglossus andempties at the summit of sublingual papilla(caruncle) at the side of frenulum of
the tongue. Is innervated by parasympathetic secretomotor fibers from facial, which runs in
chorda tympani and in lingual nerve and synapse in submandibular ganglion.
2. Sublingual gland
Is located in the floor of the mouthbetween mucous membrane above and mylohyoid muscle
below.
Surround terminal portion of submandibular duct. Empties mostly into the floor of the mouth
along sublingual fold by 12 short ducts,some of which enter the submandibular duct. Innervation
is similar to submandibular gland
3. parotid gland (see back )
Midline and deep structures of the neck
It includes: Cervical part of trachea and esophagus, Thryroid gland, Parathyroid glands,
Cervical sympathetic trunk , larynx and hyoid bone.
Trachea
Begins at inferior border of the cricoid cartilage(C6 vertebrae )
Has 16-20 C-shaped cartilages, preventing trachea from collapse.
Bifurcates at opposite lower border of T4 vertebrae (sternalangle).
Its bifurcation lies slightly to the right of median plane.
Esophagus: Is covered with pretacheal fascia and lies posterior to trachea and anterior to
prevertebral fascia
Thyroid gland: Is and endocrine gland that produces tyroxine and thryocalcitonin. Consist of
right and left lobes connected by the isthmus, which lies in front to 2-4th tracheal rings.
Sometimes muscular band descending from body of hyoid bone to the pramidal lobe of the
Page 41
For medical students “au 2nd batch: many many, hard and soft:
42. Anatomy of head and neck
By Amenu Tolera 2010
Tolera,
isthmus is levator glandulae thyroidae. The isthmus is coverd anteriorlyby the skin,superficial
fascia containing anterior jugular veins,deep fascia and sternothyroid and tyrohyoid.
Thryoid gland is supplied 3 arteries and drained by 3 veins.
Superior thyroid artery from ECA
Inferior thyroid artery from thyrocevical trunk
Thyroidae ima artery,an inconsistent branch from the brachiocephalic trunk
These arteries form anastomosis especially the two superior thyroid arteries.
Superior thyroid vein drain to internal jugular vein
Middle tyroid vein drain to internal jugular vein
Inferior thryroid vein drain to the left brachiocephalic vein.
Lymphatics from thyroid drain into lower deep cervical, prelaryngeal, pretracheal and
paratracheal lymph nodes.
Innervated by ANS,
sympathetic via thyoid branches along inferior thyroid artery from middle cervical ganglion
Parasympathetic from vagus
Why thyroid gland moves up and down with deglution?
It is enclosed in the pretracheal fascia which fixes the gland to the larynx and trachea.
Clinical anatomy
Goiter: is a pathologic enlargement of the thyroid gland,causing a swelling in the front of the
neck.
Tracheotomy: is opening into trachea by incising the third and fourth rings of trachea, after
making a vertical midline skin incision from jugular notch of manubrium sterni to the thyroid
notch of the thyroid cartilage.
Cricothyrotomy: is incision via the skin and cricothyroid membrane for relief acuterespiratory
obstruction.Is preferable to tracheostomy for nonsurgeons in emergency respiratory obstructions
Page 42
For medical students “au 2nd batch: many many, hard and soft:
43. Anatomy of head and neck
By Amenu Tolera 2010
Tolera,
Parathyroidectomy: may occur during total thyroidectomy,and cause death if PTH,calcium or
Vitamin D is not provided. Decrease plasma caclium level,causing increasedneuromuscular
activity such as muscular spasmsand nervous hyperexcitability,called tetany.
Parathyroid glands: are endocrine glands that produce PTH, which plays vital role in
regulation of calcium and phosphorus metabolism. Consist usually of four 2 superior and 2
inferior parathyroids (can vary from 2-6) small ovoid bodies( that lie againstthe dorsum of the
thyroid under its sheath but with their own capsule. Arterial supply,venous and lymphatic drainge
and innervation almost similar to thryroid gland.
Sympathetic system
Arise from intermediolateral grey columnfrom T1-L2 or L3. Enter ganglion as white rami
communicantes. Leave ganglion as grey rami communicantes
Three Fates of white rami
May terminate in the ganglion of the sympathetic chain they enter by synapsing with
excitor neuron.
May enter a sympathetic ganglion and asend or desend to a higher or lower levels of
respectively(of a ganglion)where it terminates.
May pass through sympathetic ganglion at the level of origin without synapsing and
form splanchnic nerve which synapse at a peripheral ganglion near the organ they
innervate
Cranial part of sympathetic system
Originate as internal carotid nerve,postganglionic branch from the upper end of superior
cevical ganglion.
Enters cranial cavity through carotid canal and divides into medial and lateral branches
which unite and form internal carotid plexus.
Cervical sympathetic system has three cervical ganglia and has no white rami communicants
1. The superior cervical ganglia
is the largest, lies at the level opposite C2 or C3
Medial (visceral)branches
o laryngopharyngeal branch to carotid body andpharyngeal plexus
o cardiac branches to left and right superficial and deep cardiac plexus respectively
Page 43
For medical students “au 2nd batch: many many, hard and soft:
44. Anatomy of head and neck
By Amenu Tolera 2010
Tolera,
Anterior( vascular) branches to
o Arterial branches to common carotid and external carotid via branches of trigeminal to
parasympathetic ganglia.
o Lateral (somatic)branches to cranial nerves,superior jugular bulb,and meninges of
posterior cranial fossa. Give rise to internal and external carotid nerves and superior
cervical cardiac nerve to the heart.
2. Middle cervical ganglion
o Lie at level of C6,branches to thyroid, heart, esophagus and trachea
o Give rise to cervical cardiac nerve
3. Inferior (cervicothoracic) ganglia
o Lies between transverse process of C7and neck of 1st rib, branches to
subclavian,vertebraland heart (inferior cardiac plexus)
o Give rise to inferior cervical cardiac nerve
What is ansa subclavia?
o Is the cord connecting the middle and inferior cervical sympathetic ganglia forming loop
around the 1st part of subclavian artery.
SYMPATHETIC INNERVATION HEAD AND NECK
Vasoconstrictor to blood vessels of skin and viscera
Secretomotor to sweat glands
Dilator to the pupil
Motor to dilator pupilae of the iris and smooth muscle fibers of levatorpalpebra
superioris
Sympathetic dennervation (Horner’s syndrome)
Is caused by injury to cervical sympathetic fibers.
Is characterized by five symptoms
1. Miosis, pupillay constriction resulting from paralysis of the associated dilator
muscle of the pupil
2. Ptosis, drooping of un upper eyelid from paralysis of smooth muscle
component of the levator palpebrae superioris
3. Enophthalmos, retraction of an eye ballfrom paralysis of the superior tarsal
muscle
4. Anhydrosis, absence of sweating,due to loss of secretomor fibers to sweat
glands
5. Vasodilation, leading to increased blood flow in the facial and cervical
region(loss of vasoconstriction)
PARASYMPATHETIC INNERVATION HEAD AND NECK
All Parasympathetic motor innervation to the head synapses exactly once, in one of the
four cranial parasympathetic peripheral ganglia listed below. All of these ganglia are distributed
along branches of the Trigeminal Nerve (V).
1. CILIARY GANGLION: Carries parasympathetics from Oculomotor Nerve (III)
Located in the posterior of the orbit.
GVE (Parasympathetic) innervation is to:
1. Ciliary Muscles (for Accommodation)
2. Sphincter of the Pupil (constriction, or miosis).
It hangs off of the Ophthalmic Branch of the Trigeminal Nerve (V 1 )
2. PTERYGOPALATINE GANGLION: Carries parasympathetics from Facial Nerve (VII)
Located in the Pterygopalatine Fossa in the posterior part of sphenoid bone.
Page 44
For medical students “au 2nd batch: many many, hard and soft:
45. Anatomy of head and neck
By Amenu Tolera 2010
Tolera,
GVE (Parasympathetic) innervation is to:
1. Nose
2. Palate
3. Lacrimal Glands
It hangs off of the Maxillary Branch of the Trigeminal Nerve (V 2 ).
3. SUBMANDIBULAR GANGLION: Carries parasympathetics from Facial Nerve (VII)
Located below and lateral to the tongue.
GVE (Parasympathetic) innervation is to:
1. Submandibular Gland
2. Sublingual Gland
It hangs off of the Mandibular Branch of the Trigeminal Nerve (V 3 ).
4. OTIC GANGLION: Carries parasympathetics from Glossopharyngeal Nerve (IX)
Located in Intratemporal Fossa, just below Foramen Ovale.
GVE (Parasympathetic) innervation is to the Parotid Salivary Gland.
It hangs off of the Mandibular Branch of the Trigeminal Nerve (V 3 )
Don’t forget: VAGUS NERVE (CN X) has no parasympathetic ganglion in the head. But it
sends parasympathetic innervation to the thoracic and abdominal viscera.
THE MINOR BODY CAVITIES, TONSILS AND PARANASAL SINUSES.
The oral cavity:
Definition: The minor body cavity of head via which food is ingested
Extent: from lips to oropharynx
Divisions: two major parts the vestibule(between outer fleshy wall made of cheeks and lips and inner bony wall
made of teeth and gums) the oral cavity proper (area inside teeth and gums).
Roof: by hard palate anteriorly and soft palate posteriorly
Floor: by tongue and the mucosa supported by the geniohyoid and mylohyoid muscles
Teeth
Definitions: is the hardest substance in the body.
Sets: the 1st teeth is milky which replaced by permanent tooth starting from six months.
Page 45
For medical students “au 2nd batch: many many, hard and soft:
46. Anatomy of head and neck
By Amenu Tolera 2010
Tolera,
Parts: crown and root separated by neck
Type: human beings have hetrodont dention in which there are incisors, canines, premolars and molars on each
quadrant from anterior to posterior
Structure: tooth is composed of three hard tissues and three soft tissues
Foramen: neurovascular structures enter into pulp chamber via apical foramen
Neurovascular structures of teeth
Page 46
For medical students “au 2nd batch: many many, hard and soft:
47. Anatomy of head and neck
By Amenu Tolera 2010
Tolera,
Nerve supply: 1. V3 supplies teeth and gums of mandibular arch. The inferior alveolar (dental) nerve
innervates all the teeth in the mandible. The gums of the molars and bicuspids are innervated by the long buccal
nerve .The gums of the incisors are innervated by the mental nerve. The lingual gums are innervated by the
lingual nerve.The inferior alveolar nerve enters the mandibular foramen and passes via the mandibular canal
forming the inferior dental plexus, which sends branches to all mandibular teeth on that side. The nerve to the
myohyloid muscle, a small branch of the inferior alveolar nerve, is given off just before the nerve enters the
mandibular foramen. A branch of the inferior dental plexus, the mental nerve, passes thru the mental foramen and
supplies the skin and mucous membrane of the lower lip, skin of the chin, and vestibular gingival of the
mandibular incisor teeth.
2. V2 supplies the teeth and gums of the maxillary arch.
The molar teeth are supplied by the posterior superior alveolar nerve from the pterygopalatine fossa. The
bicuspids (premolars) are innervated by the middle superior alveolar nerve from the infraorbital nerve. The
canines and incisors are innervated by the anterior superior alveolar nerve from the infraorbital nerve The gums
on the palatal surface are innervated by the nasopalatine nerve (incisors) and greater palatine nerve (bicuspids and
molars).
The blood supply to both jaws comes from superior alveolar artery from (1st part of maxillary artery) and inferior
alveolar artery (from the 3rd part of maxillary artery) for the upper and lower jaws respectively.
Venous drainage: The veins accompanying the arteries drain into maxillary vein
Lymphatic drainge: Lymphatics from teeth drain into submental or submandibular lymph nodes.
Tongue (2, 3,5,8 best )
Definition: is a muscular organ located in floor of the mouth
Attachement: is attached by muscles to the hyoid bone , mandible,styloid process,palate and pharynxFunction:
associated with functions like taste,mastication,speech, and deglution(swallowing)
Parts: has two oral (anterior 2/3) and pharyngeal (posterior 1/3) by a V-shaped sulcus ,the sulcus
terminalis.which differ developmentally, structurally and in innervation. foramen ceacum is located at apex of the
V and indicates the site of origin of embryonic thyroglossal duct. Root of tongue is attached to mandible above
and hyoid bone below. Tip of tongue is the anterior free end of the tongue,which at rest lies behind the upper
incissor teeth.
Surfaces: it has an upper (dorsal )rough and a lower(ventral) smooth surfaces.
Page 47
For medical students “au 2nd batch: many many, hard and soft:
48. Anatomy of head and neck
By Amenu Tolera 2010
Tolera,
The dorsal surface of the tongue is convex in all directions. Is rough due to projections of mucus membrane
forming four papillae (see histology). Ventral surface of the tongueis smooth. Has pelica fimbriata,deep lingual
vein,sublingual paillae, lingual fold, and frenulum
Muscles: a midline septum divide the tongue into right and left haves. Each half consist of 4 intrinsic and 4
extrinsic muscles:Muscles of tongue only eight pairs
The four intrinsic muscles originate and end in the tongue it self and change the shape of the tongue. Includes four
longitudinals
1.
Superior longitudinal-shortens
2.
Inferior longitudinal-shortens
3.
Vertical longitudinal-flatens and broadens it
4.
Transeverse longitudinal-narrows and elongate it
The four extrinsic muscles of the tongue originate outside the tongue and end in the tongue (hence all have the
suffix---glossus) and change the position of the tongue (protrude or retract, elevate or depress),includes the four
glossus muscles differing in their origin
1.
Genioglossus-protrude
2.
Hyoglossus-depress
3.
Palatoglossus-elevates
4.
Styloglossus-retracts
Nerurovascular structures of the tongue
Five (2 motor and 3 sensory) Nerves go to the tongue
A. Motor: one exception. All muscles of the tongue are innervated by hypoglossal nerve (CN XII) except
palatoglossus which is innervated by vagus (CN X).
B. Sensory: is it general or special and to anterior 2/3 or posterior 1/3 ?
1.
Glossopharngeal nerve (CN IX) is both general special sensory to the posteior 1/3 of the tongue.
2.
Facial nerve(CN VII) via chorda tympani branch is special sensory (taste) to anterior 2/3 of the
tongue.
3.
Trigeminal(CN V) via lingual nerve is general sensory to the tongue.
CN 12+10+9+7+5=higher one, s motor and lower ones sensory to tongue.
Page 48
For medical students “au 2nd batch: many many, hard and soft:
49. Anatomy of head and neck
By Amenu Tolera 2010
Tolera,
The lingual nerve: lies anterior to inferior alveolar nerve. It is sensory to the anterior two thirds of the tongue,
the floor of the mouth, and the lingual gingivae. It enters the mouth between the medial pterygoid and the ramus
of the mandible and passes anteriorly under cover of the oral mucosal, just inferior to the third moral tooth.
The chorda tympani nerve: a branch of CN VII, carries taste fibers from the anterior two thirds of the tongue
and presyn para secretomotor fibers for the submandibular and sublingual salivary glands. The chorda tympani
joins the lingual nerve in the infratemporal fossa.
The Hypoglossal nerve: Originates from medulla oblongata from its anterior aspect. Exits through hypoglossal
canal. The hypoglossal nerve enters the floor of the mouth on the lateral aspect of the hyoglossus muscle, above
the hyoid bone and the mylohyoid muscle .is a content of superior part of caroid triangle. Cranial nerve XII lies
inferior to the lingual nerve and is purely motor to the muscles of the tongue except palatoglossus.(Somatic
motor).
Three Blood supply to tongue
Three main arteries but lingual artery does the most
a. lingual artery-from ECA
b. Tonsilar artery –from facial-from ECA
c. asending pharyngeal artery- from facial-from ECA.
d. Three Venous drainage of the tongue
Three veins drain it but deep lingual vein does the most. The veins accompany the arteries (venae commtantes)
drain into their coorsponding veins.
Three Lymphatic drainage
Lymphatics from the different parts of the tongue form afferents to three lymph nodes
a. From tip of tongue –to submental LN
b. From right and left haves of rest lateral side of anterior 2/3 of the tongue-to submandibular LN
c. From posterior 1/3 of the tongue-to jugulo-omohyoid LN
Clinical anatomy
Unilateral injury of hypoglossal nerve: Have three effects
a. On protrusion of tongue-deviation is ipsilateral
b. On retraction of the tongue-paralised side higher than unparalysed side
c. On swallowing –larynx deviates towards normal side.
Bilateral injury of hypoglossal nerve:
Page 49
For medical students “au 2nd batch: many many, hard and soft:
50. Anatomy of head and neck
By Amenu Tolera 2010
Tolera,
Results in
a. motionless tongue
b. low articulation of sound
c. difficulty of swallowing (patient need to push bolus of food with fingure or throw head back)
Tongue tie (anklogossia): is abnormalshortness offrenulum lingulae, resulting in limitation of its movement and
thus severe speech impaidment can be corrected by surgical innterventions cutting the frenulum.
Palates
Definition: a partion between oral and nasal cavity forming the roof and floor them respectively.
Parts: two, soft vs. Hard palates
Hard palate: is the anterior 4/5 of the palate, and forms a bony frame work covered with mucous membrane.
formed by palatine process of maxillae and horizontal plate of palatine bone. Contains incisive foramen in median
plane anteriorly and the grater and lesser palatine foramina posteriorly. Get sensory innervation from greater
palatine and nasoplatine nerves. Get blood supply from greater and lesser palatine arteries. Get drained by veins
accompanying the arteries
Soft palate: Is the posterior 1/5 of palate extending from posterior border of hard palate.Is moveable and
separates nasopharynx from oropharynx. Moves posteriorly against the pharyngeal wall to close the
oropharyngeal (faucial) isthmus when swallowing or speaking. Has conical projection that hangs at middle of its
inferior border,the uvula.Is a muscular fold continuous with The anterior fold-palatoglossal arch(fold) which
contains palatoglossus muscle. The posterior fold palatopharyngeal arch(fold)which contains palatopharyngeus
muscle.in between the two folds is palatine tonsil. Is made up of five muscles:
5 Muscles of soft palate
1.
Tensor veli palatini-tenses soft palate and opens auditory tube
2.
Levator veli paltini-elevates soft palate and closes orophryngeal tsthmus as well as opens auditory tube.
3.
Palatoglossus-pulls up root of the tongue(elevates)and closes oropharyngeal isthmus
4.
Palatopharyngeus-pulls up the wall of pharynxand shortens it during swallowing (elevatespharynx and
close nasopharynx)
5.
Musculus uvulae-pulls up (elevates uvula)
Neurovascular structures of soft palate
Four (2 motor and 2 sensory) nerves go to the soft palate
A. Motor: one exception
All muscles of the palate are innervated by vagus via pharyngeal plexus except tensor veli paltini which is
innervated by mandibular branch of trigeminal nerve
B. Sensory: lesser platine nerve a branch from maxillary nerve glossophrengeal nerve (lateral part).
Three Blood supply to soft palate
Three arteries from different sources are distributed to soft palate
1.
Greater and lesser palatine arteries from descending palatine artery of maxillary artery
2.
Asending palatine artery of facial artery
3.
Palatine branch of ascending pharyngeal artery
Venous drainage of soft palate
Veins accompanying the arteries from soft palate drain to into either pterygoid plexusof veins or tonsillar plexus
of veins.
Lymphatic drainage of soft palate
Lymphatics from soft palate drain into upper deep cervical or retopharyngeal LN.
Tonsils
Definition: aggregation of lymphoid tissues that form a ring around oropharyngeal isthmus for immune purpose.
Page 50
For medical students “au 2nd batch: many many, hard and soft:
51. Anatomy of head and neck
By Amenu Tolera 2010
Tolera,
.
Types: four types forming one tonsilar (waldeyer,s) ring.
Pharyngeal tonosil-is found in the
posterior wall and roof of nasopharynx. Lingual tonsil-is found root of the tongue Tubal tonsil-found neat the
pharyngeal opening of the auditory tube.Palatine tonsil-lies in tonsillar fossa bounded by palatoglossal and
platophryngeal folds,and is pyramidal in shape. Has lateral and medial surfaces,superior constrictor of the
pharynx is related just deep to paltine tonsil next to paratonsillar vein. thirdly is the styloglosus muscle.
Neurovascular structures of tonsil
2 nerves go to tonsil
1. Get sensory innervations from tonsillar branch of glossophayngeal nerve
2. lesser palatine branch of maxillary nerve
Tonsil has rich blood supply
Eight arteries supply tonsil but tonsillar branch of facial does the most.
a. Inferior pharyngeal –from inferior thyroid
b. Superior laryngeal-from superior thyroid
c. Dorsal lingual-from lingual artery
d. Asending palatine –from facial
e. Tonsilar –from facial
f. Desending palatine –from maxillary
g. Artery of pterygoid canal-from maxillary
h. Greater palatine-from descending palatine
Venous drainage of tonsil
Tonsillar veins drain into lingual or pterygoid plexus of veins and facial vein
Lymphatic drainage of tonsil
Tonsillar lymph nodes drain into jugulodigastric or other cervical lymph n odes.
Clinical anatomy
Waldeyer,s lymphatic ring: surround the opening into respiratory and digestive tube includes:
a. Anterior and lower par of the ring is formed by-lingual tonsil
b. Lateral portion by-paltine and tubal tonil
c. Behind and above by-pharyngeal tonsil
Adenoid:is hypertrophy or enlargement of phayngeal tonsilobstructing passage of air from the nasal cavity
though choanae into nasophaynx, resulting in impariment of hearing and deafness (ottitis media).
Tonsillectomy: surgical removal of tonsil,may cause much bleeding because of their rich vascularity and
related to internal carotid artery. may injure lingual branch of glossopharngeal and lingual nerve of
mandibular.
Page 51
For medical students “au 2nd batch: many many, hard and soft:
52. Anatomy of head and neck
By Amenu Tolera 2010
Tolera,
Nasal cavity and paranasal sinses
The nasal cavity opens on the face through the anterior nasal aperture (nares or nostrils and communicates with
the nasopharynx through a posterior opening, the choanae
Page 52
For medical students “au 2nd batch: many many, hard and soft:
53. Anatomy of head and neck
By Amenu Tolera 2010
Tolera,
Roof : is formed by the nasal,frontal, ethmoid,(cribriform plate),and sphenoid (body) bones .the cribriform plate
transmits the olifactory nerves.
Floor: is formed by palatine process of maxilla and the horizontal plate of the palatine bone.incisive formamen
transmits the nasopalatine nerve and terminal branch of sphenopaltine artery.
Medial wall (nasal septum): formed primarly by perpendicular plate of the ethmoid bone,vomerand septal
cartilage,is also formed by processes of palatine, maxillary,frontal ,sphenoid and nasal bones.
Lateral wall: is formed by the superior and middle conchae of the ethmoid bone and the inferior conchae. Is also
formed by the nasal bone, frontal proceses and nasal surface of maxilla,lacrimal bone, perpendicular plate of
palatine bone, and medial pterygoid plate of of the sphenoid bone. Contains the following structures and
openings:
Which wall is this one?
Nasal chonca
Definition: are shelf like or scroll-likebony projectionsdirected downwards and medially
1. Inferior concha-is an independent bone
2. Middle concha is a projection from medial surface of ethmoidal labrynith
3. Superior concha –is a projection frommedial surface of ethmoidal labyrnith(smallest )
Function: increase surface area of the nose for effective conditioning of inspired air (turbines of the nose)
Meatuses of the nose
Definition: are passages beneath the overhanging conchae
Types; three only why?
Inferior meatus: lies beanth the inferior concha and is the largest turbinate.
nasolacrimal duct opens into it at the junctionof anterior 1/3 and posterior 2/3.
Middle meatus; lies underneath the middle chonae. It presents three features:
1. opening of frontal air sinus into the infundibulum
2. openings of the middle ethmoidal air cells on the ethmoidal bulla.
3. openings of the anterior ethmoidal air cells and maxillary sinus in the hiatus semilunaris
Superior meatus: underneath the superior conhae. Shortest and shallowest. receives openings of
posterior ethmodal air cells
Note: all paranasal sinuses open into meatuses of nasal cavity except sphenoidal air sinus which opens into
spheno-ethmoidal recess, a triangular fossa above superior concha.
Three Sub-divisions and mucous membranes
Page 53
For medical students “au 2nd batch: many many, hard and soft:
54. Anatomy of head and neck
By Amenu Tolera 2010
Tolera,
1. Vestibule: is the dilated part inside the nostril that is bounded by the alar cartilages and lined by skin with
hairs.
2. Respiratory region: consists of the lower 2/3 of the nasal cavity. Its mucous membrane
warms,moistens,and cleans incoming air
3. Olifactory region: consist of superior nasal conchaand upper 1/3 of the nasal septum.Is innervated by
olifactory nerves,which convey sense of smell from the olifactory cells and enter cranial cavity through
cribriform plate of ethmoid bone to olfactory bulb
The Olfactory Nerve (CN I): This is the nerve of smell. Is a purely sensory nerve. The fibers
that comprise this nerve are unmyelinated axons of olfactory cells that are located in the nasal
mucosa.The axons of these cells unite to form 18 to 20 small nerve bundles that are known
collectively as the olfactory nerve. Each of these nerves is covered by the three layers of
meninges and pass through foramina in the cribriform plate of ethmoid bone and enter the
olfactory bulbs in anterior cranial fossa and project to olifactory area of the cerbrum.
Neurovascular bundles of the nasal cavity
Six nerves (1 special sensory and five genral sensory goes to the nasal cavity
1. Special sensory(smell) is by olifactory nerve for the olifactory area
2. Genreal sensation: is by
3. anterior ethmoidal branch of V1
4. Nasopalatine,posterior-superior,and anterior inferiorlateral nasal branches of V2 viathe pterygopaltine
ganglion
5. Anterior superior alveolar branch of the infraorbital nerve.
Nasal cavity has rich blood supply
Three major arteries supply the nasal cavity though their branches but spenopalatine artery of maxillary artery
is clinically more important. why?
Opthalmic artey via lateral nasal branches of anterior and posterior ethmoidal aa
Maxillary artery via Posterior lateral nasal and posterior septal branches of sphenopalatine artery and via
greater palatine artery
Facial artery via septal branch of superior labial and lateral nasal branches
Venous drainage of nasal Cavity
Veins of nasl cavity form submucous plexus which empties into sphenopaltine vein,facial vein,opthalmic veins
and superior saggital sinus via foramen ceaum.
Lymphatic drainage
Page 54
For medical students “au 2nd batch: many many, hard and soft: