Endoscopic diagnosis
•
0 recomendaciones•258 vistas

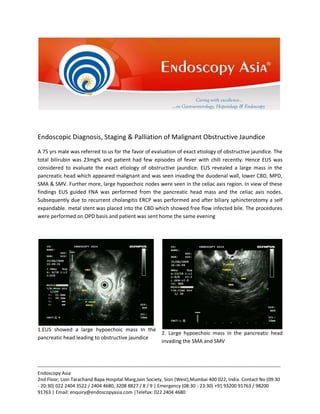
1. EUS showed a large hypoechoic mass in the pancreatic head leading to obstructive jaundice and invading nearby vessels. Hypoechoic nodes in the celiac axis suggested metastasis. 2. EUS-guided FNA of the mass confirmed pancreatic adenocarcinoma. ERCP showed a stricture and placed a metal stent for palliation. 3. The case demonstrates accurate diagnosis, staging and palliative management of advanced pancreatic cancer with obstructive jaundice through EUS and ERCP in a single session.

Recomendados
Recomendados
Más contenido relacionado
La actualidad más candente
La actualidad más candente (20)
Destacado
Destacado (9)
Similar a Endoscopic diagnosis
Similar a Endoscopic diagnosis (20)
Último
Último (20)
Endoscopic diagnosis
- 1. Endoscopic Diagnosis, Staging & Palliation of Malignant Obstructive Jaundice A 75 yrs male was referred to us for the favor of evaluation of exact etiology of obstructive jaundice. The total bilirubin was 23mg% and patient had few episodes of fever with chill recently. Hence EUS was considered to evaluate the exact etiology of obstructive jaundice. EUS revealed a large mass in the pancreatic head which appeared malignant and was seen invading the duodenal wall, lower CBD, MPD, SMA & SMV. Further more, large hypoechoic nodes were seen in the celiac axis region. In view of these findings EUS guided FNA was performed from the pancreatic head mass and the celiac axis nodes. Subsequently due to recurrent cholangitis ERCP was performed and after biliary sphincterotomy a self expandable. metal stent was placed into the CBD which showed free flow infected bile. The procedures were performed on OPD basis and patient was sent home the same evening 1.EUS showed a large hypoechoic mass In the pancreatic head leading to obstructive jaundice 2. Large hypoechoic mass in the pancreatic head invading the SMA and SMV -----------------------------------------------------------------------------------------------------------------------------------------Endoscopy Asia 2nd Floor, Lion Tarachand Bapa Hospital Marg,Jain Society, Sion (West),Mumbai 400 022, India. Contact No (09:30 - 20:30) 022 2404 3522 / 2404 4680, 3208 8827 / 8 / 9 | Emergency (08:30 - 23:30) +91 93200 91763 / 98200 91763 | Email: enquiry@endoscopyasia.com |Telefax: 022 2404 4680
- 2. 3.Hypoechoic nodes were seen in the celiac axis region- suggestive of distant nodal metastasis 4.EUS guided FNA of the pancreatic head mass performed.Needle was passed transduodenally under EUS guidance. 5.ERCP showed dilated upper CBD with a stricture In the region of pancreatic head 6.ERCP and placement of Self expandable Metal biliary stent -----------------------------------------------------------------------------------------------------------------------------------------Endoscopy Asia 2nd Floor, Lion Tarachand Bapa Hospital Marg,Jain Society, Sion (West),Mumbai 400 022, India. Contact No (09:30 - 20:30) 022 2404 3522 / 2404 4680, 3208 8827 / 8 / 9 | Emergency (08:30 - 23:30) +91 93200 91763 / 98200 91763 | Email: enquiry@endoscopyasia.com |Telefax: 022 2404 4680
- 3. Expert Comments: As we can see in this case due to very advanced nature of pancreatic tumor which eventually turned out tobe a poorly differentiated adenocarcinoma on EUS guided FNA of the mass and nodes, a single step detection, diagnosis, staging and palliation of malignant obstructive jaundice was performed in one sedation on an OPD basis. Several studies have shown that whenever there is a patient of obstructive jaundice of uncertain diagnosis, EUS will provide accurate diagnosis in most cases. It is a standard protocol at Endoscopy Asia that if a patient has obstructive jaundice and if the diagnosis is not clear on previous other imaging studies, then patient will be subjected to EUS sos EUS guided FNA if there is a mass lesion followed by ERCP and ductal clearance if stones are seen or stenting if a malignant lesion is encountered. Studies have shown that most patient who are diagnosed with Pancreatic adenocarcinoma who present with obstructive jaundice are advanced in their presentation and hence Surgery should be considered only if there is a chance of cure and R0 resection without nodal involvement, and in most centres across the world role of palliative surgery is now diminishing. Since the advent of EUS / FNA and Metal Biliary stenting / Duodenal stenting, endoscopic palliation is now a preferred approach. If patient has intractable pain due to advanced pancreatic cancer then in the same sedation we can also offer EUS guided Coeliac Plexus Neurolysis (EUS-CPN) thus completing the entire spectrum of palliative care. This approach of EUS sos ERCP provides accurate diagnosis and optimal management of obstructive jaundice in most patient without any additional investigations or interventions. This has been our practice for over 13 years since I pioneered Pancreato-biliary EUS in India and we hope that more such centres across the country will incorporate such a protocol in years to come. Case Capsule 7 Management of Obstructive Jaundice of Unknown Etiology Management of Obstructive Jaundice of Unknown Etiology 1. Tubular filling defects seen in a dilated CBD-A live 2. ERCP-After selective cannulation of CBD biliary round worm phincerotomy was performed -----------------------------------------------------------------------------------------------------------------------------------------Endoscopy Asia 2nd Floor, Lion Tarachand Bapa Hospital Marg,Jain Society, Sion (West),Mumbai 400 022, India. Contact No (09:30 - 20:30) 022 2404 3522 / 2404 4680, 3208 8827 / 8 / 9 | Emergency (08:30 - 23:30) +91 93200 91763 / 98200 91763 | Email: enquiry@endoscopyasia.com |Telefax: 022 2404 4680
- 4. 3. ERCP-Cholangiogram showed a tubular filing 4. Live round worm from CBD was removed with a defect in a midly dilated CBD stone extraction balloon catheter 5. To prevent reentry of the round worm a 7Fr stent was placed into the CBD 6. Multiple live roundworms were seen in the third part of the duodenum,one of them managed to enter the bile duct and caused all the symtoms A 25 yrs female was referred to us for the favor of EUS sos ERCP for suspected block in the CBD leading to recurrent epigastric pain with mild LFT abnormality and no stones were seen in Gall bladder on USG abdomen, however, mild dilatation of CBD was seen without any obvious stone or filling defects. EUS at Endoscopy Asia revealed a large tubular structure in the dilated CBD and this was suspected to be a large round worm. There was no other pathology in the pancreato-biliary system apart from this findings and therefore ERCP was considered. ERCP showed a filling defect on cholangiogram and confirmed the EUS findings. Biliary sphincterotomy was performed and the round worm was extracted using a stone extraction balloon catheter. Few more live round worms were also seen in the third part of duodenum and therefore after ductal clearance a 7 fr stent was placed to ensure effective ductal drainage. Patient was treated on an OPD basis and sent home the same day. -----------------------------------------------------------------------------------------------------------------------------------------Endoscopy Asia 2nd Floor, Lion Tarachand Bapa Hospital Marg,Jain Society, Sion (West),Mumbai 400 022, India. Contact No (09:30 - 20:30) 022 2404 3522 / 2404 4680, 3208 8827 / 8 / 9 | Emergency (08:30 - 23:30) +91 93200 91763 / 98200 91763 | Email: enquiry@endoscopyasia.com |Telefax: 022 2404 4680
- 5. Expert Comments: As we have seen in the previous case that patients with obstructive jaundice without a definitive diagnosis of etiology of obstructive jaundice can be diagnosed accurately on EUS. Here we managed to clear the duct of a live round worm which was causing intermittent obstruction of the bile flow leading to mild LFT abnormality and severe epigastric pain. This patient was then given oral antihelminthic medication to take care of rest of the round worms. Since there are still some serious hygienic issues in our society especially in the rural and slum areas that we have to keep such pathology in mind at the time of management of such patients. I would like to share here with our readers that it is a standard protocol at Endoscopy Asia that unless EUS proves that there is a definitive pathology in the bile duct that needs treatment we will not proceed with ERCP. In other words we at Endoscopy Asia do not have negative ERCP so to speak and in the era of such accurate modalities such as EUS & MRCP, diagnostic ERCP has no role in most cases. -----------------------------------------------------------------------------------------------------------------------------------------Endoscopy Asia 2nd Floor, Lion Tarachand Bapa Hospital Marg,Jain Society, Sion (West),Mumbai 400 022, India. Contact No (09:30 - 20:30) 022 2404 3522 / 2404 4680, 3208 8827 / 8 / 9 | Emergency (08:30 - 23:30) +91 93200 91763 / 98200 91763 | Email: enquiry@endoscopyasia.com |Telefax: 022 2404 4680