Case-2
•
1 recomendación•291 vistas

Acute Pancreatitis- Leading Pancreatic Pseudocyst- Endoscopic Treatment performed (EUS Guided Cystogastrostomy )

Recomendados
Recomendados
Más contenido relacionado
La actualidad más candente
La actualidad más candente (20)
Similar a Case-2
Similar a Case-2 (17)
Último
Último (20)
Case-2
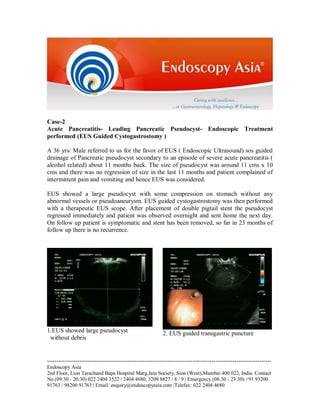
- 1. Case-2 Acute Pancreatitis- Leading Pancreatic Pseudocyst- Endoscopic Treatment performed (EUS Guided Cystogastrostomy ) A 36 yrs/ Male referred to us for the favor of EUS ( Endoscopic Ultrasound) sos guided drainage of Pancreatic pseudocyst secondary to an episode of severe acute pancreatitis ( alcohol related) about 11 months back. The size of pseudocyst was around 11 cms x 10 cms and there was no regression of size in the last 11 months and patient complained of intermittent pain and vomiting and hence EUS was considered. EUS showed a large pseudocyst with some compression on stomach without any abnormal vessels or pseudoaneurysm. EUS guided cystogastrostomy was then performed with a therapeutic EUS scope. After placement of double pigtail stent the pseudocyst regressed immediately and patient was observed overnight and sent home the next day. On follow up patient is symptomatic and stent has been removed, so far in 23 months of follow up there is no recurrence. 1.EUS showed large pseudocyst without debris 2. EUS guided transgastric puncture --------------------------------------------------------------------------------------------------------------------Endoscopy Asia 2nd Floor, Lion Tarachand Bapa Hospital Marg,Jain Society, Sion (West),Mumbai 400 022, India. Contact No (09:30 - 20:30) 022 2404 3522 / 2404 4680, 3208 8827 / 8 / 9 | Emergency (08:30 - 23:30) +91 93200 91763 / 98200 91763 | Email: enquiry@endoscopyasia.com |Telefax: 022 2404 4680
- 2. 3. Puncture tract dilated with cystotome 5. Double pigtail stent draining clear Pseudocyst fluid into the stomach 4. Tract further dilated with a 6 mm balloon 6 Fluoroscopy shows double pigtail stent Placed across the stomach wall into the Pseudocyst. Echoendoscope seen. Expert comments: It is well known that after an episode of acute pancreatitis some patient may develop pseudocyst of pancreas. Almost 2/3rd of them resolve spontaneously over a period of 6-8 months and about 1/3 of them may become symptomatic which requires treatment. Traditionally the treatment of Pancreatic Pseudocyst has been Surgical – either open surgery or Laparoscopic. However, with the advent of EUS guided drainage, in our experience for last 1 decade eversince we pioneered the Interventional EUS in Mumbai and India, almost 95-97% of symptomatic Pseudocysts at Endoscopy Asia can be managed with EUS guided drainage procedure. Published studies have shown similar conclusion that most patients with Pancreatic pseudocyst either secondary to acute or chronic pancreatitis can be managed successfully with EUS guided drainage, hence the role of Surgery is there only if EUS --------------------------------------------------------------------------------------------------------------------Endoscopy Asia 2nd Floor, Lion Tarachand Bapa Hospital Marg,Jain Society, Sion (West),Mumbai 400 022, India. Contact No (09:30 - 20:30) 022 2404 3522 / 2404 4680, 3208 8827 / 8 / 9 | Emergency (08:30 - 23:30) +91 93200 91763 / 98200 91763 | Email: enquiry@endoscopyasia.com |Telefax: 022 2404 4680
- 3. infrastructure and expertise are not available, especially if there is a non bulging pseudocyst.. Though large bulging pseudocysts can be drained even endoscopically, whenever possible EUS guided drainage will provide a safer window of puncture across the gut wall and thereby prevent complications such as bleeding and perforation that can occur. Case 3 Bleeding per rectum- Endoscopic diagnosis and treatment A 48yrs/ F was referred to us for the favor of colonoscopy to evaluate the exact etiology of bleeding per rectum off and on for last 6 months leading to drop in Hb. Patient was treated conservatively for colitis and piles by a family physician. However, patient continued to have symptoms despite several months of treatment and hence went to see a Surgeon who asked for a colonoscopic evaluation. Ileo-colonoscopic evaluation revealed a large 4 cms bilobed polyp with a thick stalk at the recto-sigmoid junction. Rest of the colon upto the caecum and also the last 15 cms of terminal ileum was normal. Polypectomy was then performed with a snare and cautery after injection of diluted saline adrenaline into the stalk. Complete resection of the polyp was achieved and was sent for HPE, which revealed tubulovillous adenoma without dysplasia. Patient was sent home the same evening. 1. Large bilobed polyp with thick stalk seen in Recto-sigmoid region. 2. Diluted saline adrenaline injected in the stalk --------------------------------------------------------------------------------------------------------------------Endoscopy Asia 2nd Floor, Lion Tarachand Bapa Hospital Marg,Jain Society, Sion (West),Mumbai 400 022, India. Contact No (09:30 - 20:30) 022 2404 3522 / 2404 4680, 3208 8827 / 8 / 9 | Emergency (08:30 - 23:30) +91 93200 91763 / 98200 91763 | Email: enquiry@endoscopyasia.com |Telefax: 022 2404 4680
- 4. 3. The stalk strangulated with a polypectomy Snare 4. No evidence of bleeding from the resected site 5. Polyp retrieved with a Roth net. 6. Bilobed resected polyp was sent for histopathological examination Expert comments Patient above the age of 45 yrs with h/o bleeding per rectum should be investigated in detail and empirical treatment without a definitive diagnosis should be avoided. In this case patient suffered for almost 6 months before getting the a definitive diagnosis and effective endoscopic treatment in the same sedation and was cured of her symptoms. Pedunculated or even flat sessile colonic lesions can be successfully resected with endoscopic techniques such as polypectomy as in this case or we can employ more sophisticated tools that can perform EMR ( Endosocpic Mucosal Resection ) or ESD ( Endoscopic Submucosal Dissection). It is our policy at Endoscopy Asia to inspect 10-15 cms of terminal ileum in all patients referred to us for Colonoscopy and more so if we are looking for a lesion that could bleed. It is also important to perform these procedures under one sedation at the pilot --------------------------------------------------------------------------------------------------------------------Endoscopy Asia 2nd Floor, Lion Tarachand Bapa Hospital Marg,Jain Society, Sion (West),Mumbai 400 022, India. Contact No (09:30 - 20:30) 022 2404 3522 / 2404 4680, 3208 8827 / 8 / 9 | Emergency (08:30 - 23:30) +91 93200 91763 / 98200 91763 | Email: enquiry@endoscopyasia.com |Telefax: 022 2404 4680
- 5. endoscopy, both the diagnostic and therapeutic aspects when we deal with bleeding per rectum in an infrastructure which is equipped enough with all the methods of endoscopic haemostasis. --------------------------------------------------------------------------------------------------------------------Endoscopy Asia 2nd Floor, Lion Tarachand Bapa Hospital Marg,Jain Society, Sion (West),Mumbai 400 022, India. Contact No (09:30 - 20:30) 022 2404 3522 / 2404 4680, 3208 8827 / 8 / 9 | Emergency (08:30 - 23:30) +91 93200 91763 / 98200 91763 | Email: enquiry@endoscopyasia.com |Telefax: 022 2404 4680