Maxillary sinus /certified fixed orthodontic courses by Indian dental academy
•
20 recomendaciones•6,341 vistas

The Indian Dental Academy is the Leader in continuing dental education , training dentists in all aspects of dentistry and offering a wide range of dental certified courses in different formats. Indian dental academy provides dental crown & Bridge,rotary endodontics,fixed orthodontics, Dental implants courses.for details pls visit www.indiandentalacademy.com ,or call 0091-9248678078

Recomendados
Más contenido relacionado
La actualidad más candente
La actualidad más candente (20)
Destacado
Destacado (20)
Similar a Maxillary sinus /certified fixed orthodontic courses by Indian dental academy
Similar a Maxillary sinus /certified fixed orthodontic courses by Indian dental academy (20)
Más de Indian dental academy
Más de Indian dental academy (20)
Último
Último (20)
Maxillary sinus /certified fixed orthodontic courses by Indian dental academy
- 2. CONTENTS • • • • • • • INTRODUCTION. DEVELOPMENT. HISTOLOGY. MAXILLARY SINUSITIS . ORO-ANTRAL FISTULA. CALDWELL -- LUC OPERATION. FESS.CONCLUSION. www.indiandentalacademy.com
- 3. INTRODUCTION • The sinuses are the air spaces within the pneumatic bones situated at the frontobasal region of skull. • 4 in number. Frontal, Maxillary, Sphenoidal and Ethemoidal. • Form the boundaries of nasal cavity. • Open into the nasal cavity . www.indiandentalacademy.com
- 4. • Maxillary sinus is a large pneumatic space present in body of maxilla. • Largest of all sinuses. • Antrum of Highmore –in 1962. www.indiandentalacademy.com
- 5. DEVELOPMENT • Begin their development as evagination of the mucosa of the nasal fossa during the 3rd and 4th fetal months. • Grows rapidly from birth to 3 years of age and 6 to 7 years of age, and then slowly up to 18 years. www.indiandentalacademy.com
- 7. HISTOLOGY • Maxillary sinus lined by three layers: epithelial layer, basal lamina and sub epithelial layer with periostium. • Epithelium is pseudo stratified, columnar and ciliated. • As cilia beats, the mucous on epithelial surface moves from sinus interior towards nasal cavity. www.indiandentalacademy.com
- 8. ANATOMY • Four sided pyramid located in body of the maxilla. • Anterior wall – facial surface of maxillary bone • Posterior wall – infratemporal surface of maxilla. • Medial wall – lateral wall of nasal cavity. • Roof – floor of orbit. • Floor – alveolar process of maxilla. DIMENSIONS: Height – 33 mm Width -23 mm Length – 34 mm (anteroposterior) www.indiandentalacademy.com
- 9. • Osteomeatal complex- space within the middle meatus into which the maxillary, anterior ethmoid, and frontal sinuses drain • Which is collectively constituted by the uncinate process, the maxillary ostium, the infundibulum, and the ethmoid bulla. www.indiandentalacademy.com
- 11. • NERVE SUPPLY – anterior, middle, and posterior superior alveolar nerves, branches of maxillary and infra – orbital nerves. www.indiandentalacademy.com
- 14. Applied Anatomy: • In adults, there is a distance of approximately, 1-1.25cms between the floor of the sinus and the root apices of maxillary posterior teeth. • Von Bornsdorff (1925) found in his series that the roots of second molar were closest to the floor. • Paatero (1939) also confirmed this finding ; with the next the order of frequency were; the first molar, third molar, second pre molar, first premolar and canine. www.indiandentalacademy.com
- 15. • Maxillary sinus reaches its normal adult size by the age of 18 -26 years. Hence the risk of creating oroantral fistula is less in children and young adults. • Guven in 1998 indicated that oroantral fistula most frequently occurs after the third decade of life which agrees with the results of other authors such as Lin in 1991 and Punwutikorn and co-workers in 1994. • Lin et al. in 1991 reported that the maxillary sinus is more developed in women and that there is therefore greater possibility of the occurrence of oroantral communication and fistula in women . • Periapical involvement, in the form of acute or chronic abscess in teeth related to floor of sinus, may secondarily involve maxillary sinus. www.indiandentalacademy.com
- 16. • Whenever antral puncture is carried out, should be made through the middle meatus in children and through inferior meatus in adults. • The antral puncture the inferior meatus is not a point of dependent drainage for maxillary sinus. • The floor of the sinus can have three basic positions: beneath the level of the floor of the nasal cavity, on its level or above its level. • The floor of maxillary sinus is about 1.25cms below the floor of the nose. www.indiandentalacademy.com
- 17. FUNCTIONS: • Reduces the weight of the skull. • Adds resonance to the voice. • Humidifies and warms the inspired air and thus protects the internal structures, especially the brain against cold and dry air. • Moistened the nasal cavity and probably contribute to olfaction. • Enhances the facio cranial resistance to mechanical shock. • Produces bactericidal lysozyme and discharges them to the nasal cavity. www.indiandentalacademy.com
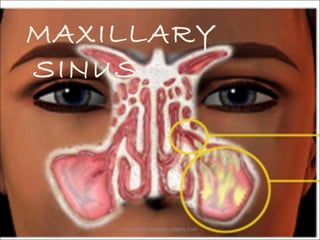
- 18. MAXILLARY SINUSITIS • Definition: Inflammation of the mucosa of the maxillary sinus. • Pansinusitis: Inflammation of most or all of Para nasal sinuses simultaneously. www.indiandentalacademy.com
- 19. Classification: • • • • Acute. Sub acute. Recurrent acute. Chronic. • A diagnosis of acute sinusitis requires that criteria satisfying a strong history for sinusitis are present for 1 to 4 weeks. • Sub acute sinusitis requires that these criteria have existed for 4 to 12 weeks. • Chronic sinusitis the criteria are present for at least 12 weeks. • In recurrent acute sinusitis, episodes last < 4 weeks, but the patient is asymptomatic between episodes. www.indiandentalacademy.com
- 20. ETIOLOGY • • • • • • • Infection Trauma Allergy Neoplasm. Infected cysts. Oroantral communication. Displaced tooth or root. www.indiandentalacademy.com
- 21. CLINICAL PRESENTATION MAJOR FACTORS: • • • • • • • Facial pain/pressure . Facial congestion/fullness. Nasal drainage/discharge . Nasal obstruction/blockage Fatigue Hyposmia/anosmia (decreased or absent sense of smell) Fever (acute sinusitis only) Purulence on nasal endoscopy (diagnostic by itself) www.indiandentalacademy.com
- 22. MINOR FACTOR: • • • • • • • Headache Maxillary dental pain Cough Halitosis (bad breath) Fatigue Ear pain, pressure, or fullness Fever *Either two major factors, or one major and two minor, are required for a diagnosis of rhinosinusitis. Purulence on nasal endoscopy is diagnostic. Fever is a major factor in only acute sinusitis.* www.indiandentalacademy.com
- 23. Microbiology: • Normal flora of maxillary sinus: Streptococci, Porphyromonas, Prevotella, Fusobacterium. • Maxillary sinusitis of non odontogenic origin: The important aerobes are Streptococcus pneumoniae, Haemophilus influenza, Staphylococcus aureous.Anaerobes are: Porphyromonas, Prevotella, Peptococcus, Fusobacterium. • Maxillary sinusitis of odontogenic origin: The predominant organisms are aerobic Streptococci, and anaerobic Peptococcus, Peptostreptococcus, Porphyromonas, Prevotella, Eubacterium sps. www.indiandentalacademy.com
- 24. ROLE OF VIRUSES: • Influenza virus, rhinovirus, respiratory syncytial virus, parainfluenza virus, corona virus may be implicated. ROLE OF FUNGI: • Allergic fungal sinusitis- Dematiaceae family, Aspergillus species. • Mucoraceae family- diabetics. www.indiandentalacademy.com
- 25. Pathophysiology PREDISPOSING FACTORS: • Mechanical obstruction of mucociliary flow, particularly in the OMC region. • Defects in ciliary capability to propel the mucous blanket. • Abnormal quantity or quality of secretions. www.indiandentalacademy.com
- 27. • Inflammation of mucus membrane of maxillary sinuses. • Hyperplasia and hypertrophy of mucous membrane. • Edematous ostium. www.indiandentalacademy.com
- 28. •Drainage of sinus blocked. •Accumulation of the secretions. •Bacterial growth. www.indiandentalacademy.com
- 29. DIAGNOSIS: Radiology: The abnormalities to be looked for include: • Evidence of thickening of the mucosa and the boney walls ( caused by chronic sinus diseases). • Air - fluid level ( caused by accumulation of mucous, pus and blood). • Foreign bodies. www.indiandentalacademy.com
- 30. • Acute sinusitis :Affected antrum shows uniform opacity. Sometimes a fluid level indiscernable. • Chronic sinusitis: The radiograph shows pansinusitis, fluid level, thickened lining is also seen www.indiandentalacademy.com
- 31. Trans illumination: • Carried out by placing a strong light in the centre of the mouth of the patient with the lips closed. • The results of the normal sinus will be a definite infra orbital crescent of light, a brightly lit eye and glowing pupil. • In case, the antral cavity contains pus, mucous, polyps, blood and a lining thickened membrane and a fibro-osseous lesions or a tumor, it will not light up as it was in normal circumstances. www.indiandentalacademy.com
- 33. MEDICAL MANAGEMENT ANTIBIOTICS: • Amoxicillin 250-500mgs 8 hrly for 10-14 days. • Erythromycin 250-500mgs 6 hrly for 10-14 days. • It has been further recommended that cephalosporins, macrolides, penicillinase-resistant penicillins, and should be reserved for failures of first-line therapy or for complications. DECONGESTANTS: • Ephedrine sulphate 0.5 -1 % • Phenylephrine 2% • Topical decongestants must be used judiciously, however, as continuance of these medications beyond 3 to 5 days is associated with reduced duration of action and rebound vasodilation, a condition known as rhinitis medicamentosa. www.indiandentalacademy.com
- 34. • STEROID THERAPY: Prednisone or methylprednisolone - begin at 30 mg daily and are tapered over 2 to 3 weeks. • ANTIFUNGAL AGENTS: Itraconazole 200 mg bid. • ANTIHISTAMINES: Should be limited to allergic sinusitis. Antihistamines may cause drying and thickening of nasal secretions resulting in impaired mucociliary flow. www.indiandentalacademy.com
- 35. SURGICAL MANAGEMENT INDICATIONS: • Acute sinusitis with evolving complication. • Chronic sinusitis that has failed maximum medical management including at least 3 weeks of broad spectrum antibiotics. • Most forms of fungal sinusitis. • In cases of complicated acute sinusitis and invasive fungal disease, surgery should be performed on an emergent basis. www.indiandentalacademy.com
- 36. • • • • • GOALS OF SURGERY: To remove chronically inflamed tissue. To restore sinus ventilation. To drainage. To provide mucociliary clearance. Evidence exists that in chronic sinusitis the inflammatory process involves the underlying bone. Thus, it is especially important to resect the bony ethmoid partitions underlying chronically inflamed mucosa. www.indiandentalacademy.com
- 37. • Oroantral communication and fistula Definition: An oroantral fistula is an epithelialised, pathological, unnatural communication between oral cavity and maxillary sinus. • • • • • • • • Etiology: Extraction of teeth. Periapical lesions. Injudicious use of instruments Facial trauma. Surgical procedures. Osteomyelitis. Syphilis. Infected implant dentures. www.indiandentalacademy.com
- 38. Symptoms of fresh oroantral communication: • Escape of fluids • Epistaxis • Escape of air • Enhanced column of air. • Excruciating pain www.indiandentalacademy.com
- 39. Symptoms of established oroantral fistula: • Pain. • Persistent purulent or mucoprulent foul unilateral nasal discharge. • Post nasal drip. • Popping out of antral polyp. www.indiandentalacademy.com
- 40. AIMS OF MANAGEMENT: • To protect the sinus from oral microbial flora. • To prevent escape of fluids and other contents across the communication. • To eliminate existent antral pathology. • To establish drainage through inferior meatus. • Hanazawe - oroantral fistula of less than 2 mm diameter has the possibility of spontaneous healing. Diameter of more than 3 mm spontaneous healing is hampered because of the possibility of inflammation of the sinus. • In 1957 Martensson -- less possibility of spontaneous healing when the oroantral fistula has been present for 3 to 4 weeks, or when its diameter is greater than 5 mm. • The choice of these procedures is influenced not only by the amount and condition of the tissue available for repair but also by the size and location of the defect. The palatal rotation flap (PRF), first described by Ashley in 1939, is a popular method for the closure of OACs. www.indiandentalacademy.com
- 41. A review of operative techniques • In 1936 Rehrmann -- buccal flap. • In 1939 Ashley -- palatinal flap. • In 1961 Goldman et al. -- applied gold foil to ensure stability of the flap. • In 1974 Takahashi and Henderson, and in 1980 James -mucosal palatinal island flap. www.indiandentalacademy.com
- 42. • In 1974 -- palatinal flap which is carried under the bridge of the palatinal gingiva along the alveola of the extracted tooth. • In 1980 Ito et al. isolated the mucosal upper layer and connective tissue layer of submucosa on a palatinal flap, so that the submucosal part of the flap covered the fistula, and the mucosal part of the flap the denuded palatal surface. This is a so-called palatinal submucosal flap. • In 1985 Yamazaki et al. described a method of submucosal palatinal island flap, in which the submucosal layer of the anterior part of the palatinal flap covers the fistula, and the mucosal part covers the defect of the palatinal surface in the frontal part, and with a much thicker flap in the posterior part. www.indiandentalacademy.com
- 43. • In 1992 Zide and Karas used blocks of hidroxyappatite during plastics of an oroantral fistula. • The technique of interseptal-interradicular alveolectomy is one of the possibilities for treatment of oroantral fistula, described by Hori et. al in 1995. • In 1995 Hanazawa et al. closed an oroantral communication by applying a BFP-buccal fat pad graft www.indiandentalacademy.com
- 44. SURGICAL TECHNIQUES • Local flaps. • Distant flaps. • Grafts. www.indiandentalacademy.com
- 45. Buccal flap advancement operation • Von Rehermann - 1936. www.indiandentalacademy.com
- 47. ADVANTAGES: • simple and efficient method . • Having a broad base --adequate blood supply to the flap. • Denture may be worn immediately since the palatal mucosa is intact. • The donor site closes exactly with no raw area left behind for granulation. • The flap mobility is improved by making parallel incisions in the periosteum at the base of the flap. • In 1975 Killey and Kay reported success with this method in 93% of cases. DISADVANTAGES: • In 1981 Obradovie et al -- significant lowering of the depth of vestibule. • cheek oedema . www.indiandentalacademy.com
- 48. • • • • • MOCZAIR BUCCAL SLIDING FLAP: Trapezoidal flap WOWERN -- change in the vestibular sulcus is negligible by shifting the flap one tooth distally. Disadvantages -- greater amount of dentogingival detachment . May result in variable degree of periodontal diseases. Leaves a raw area -- increased scar formation. www.indiandentalacademy.com
- 49. TRANSVERSAL FLAP: • • • • Schuchardt described this procedure. Buccal vestibular height was not affected. Does not offer greater mobility. Raw area over the donor site following the closure. www.indiandentalacademy.com
- 52. ADVANTAGES: • Adequate blood supply. • Adequate thickness of the flap. • Preservation of the vestibular height. DISADVANTAGES: • Leaves a raw area on the palate . • Bulge of soft tissue is created at the axis of rotation. www.indiandentalacademy.com
- 53. ANTERIORLY BASED PALATAL FLAP www.indiandentalacademy.com
- 54. STRIGHT – AVANCEMENT FLAP: www.indiandentalacademy.com
- 55. SUBMUCOUS CONNECTIVE TISSUE FLAP www.indiandentalacademy.com
- 59. TONGUE FLAPS ANTERIORLY BASED PARTIAL THICKNESS DORSAL TONGUE FLAP POSTERIORLY BASED FULL THICKNESS LATERAL TONGUE FLAP www.indiandentalacademy.com
- 60. Caldwell Luc Operation: History: • George Caldwell in 1893 from Newyork described a method of gaining entry into the maxillary sinus via canine fossa. • Henry Luc in 1897, from Paris also reported the same procedure as his own later the procedure was accepted as Caldwell Luc operation. www.indiandentalacademy.com
- 61. Indications: • For removal of root fragments, teeth, or foreign body, form maxillary sinus. • To treat chronic maxillary sinusitis. • Removal of cysts and growths. • Management of hematoma. • Removal of impacted canine and impacted third molar • Along with closure of chronic oroantral fistula associated with chornic maxillary sinusitis. www.indiandentalacademy.com
- 63. Functional Endoscopic sinus surgery: • To restore the mucociliary function. History • Hirschmann has been credited as the first surgeon to have attempeted nasal and sinus endoscopy with a modified cytoscope in 1901. • The first discription of endoscopical examining nasal cavity and the antrum of Highmore were published by Maxwell and Malt 1925. www.indiandentalacademy.com
- 64. INDICATIONS: • Recurrent sinusitis. • Chronic hyperplastic sinusitis. • Chronic sinusitis with mucocele formation. • Fungal sinusitis inpatients with diabetes. • Neoplasms. www.indiandentalacademy.com
- 65. TYPES: Anand and Panje’s classification• Type 1- nasal endoscopy and uncinectomy . • Type 2- Nasal endoscopy, uncinectomy, bulla ethmoidectomy, removal of sinus lateralis mucous membrane and exposure of frontal recess or frontal sinus. • Type 3- Type 2 plus maxillary sinus antrostomy through the natural sinus ostium. • Type 4- Type 3 surgical technique with complete posterior ethmoidectomy. • Type 5- Type 4 surgical technique with sphenoidectomy and stripping of mucous membrane. www.indiandentalacademy.com
- 66. CONCLUSION Depending upon careful clinical and radiographic examination, proper assessment of findings the nature of the disease should be understood and proper treatment should be planned. The patient should be called regularly for follow up. www.indiandentalacademy.com
- 67. References • Principles of Oral & Maxillofacial Surgery –Peterson • Treatment of oroantral fistula – Acta Stomatol vol. 36, 2002 • Use of buccal pad of fat for intraoral reconstruction BJOMS: 35; 1997 • Repair of oroantral communications in the 3rd molar region by random palatal flap: IJOMS; 2001 • Grays anatomy – 3rd volume • Closure of oroantral fistula – IJOMS ; 1998: 17 • Oral histology - Tencates www.indiandentalacademy.com
- 78. Thank you For more details please visit www.indiandentalacademy.com www.indiandentalacademy.com