Restorative Materials in Pediatric Dentistry: Recent Advancements
•
196 recomendaciones•36,679 vistas

This document provides an overview of restorative materials used in pediatric dentistry, including recent advancements. It discusses the need for restoration in deciduous teeth and the requirements of ideal restorative materials. The main materials covered are glass ionomer cement, composite resins, and amalgam. For glass ionomer cement, it describes the composition, setting reaction, properties, classifications, and recent modifications like resin-modified, nano, and compomer versions. Recent advancements discussed include alternatives to amalgam and improvements to composites and glass ionomer cement.

Recomendados
Más contenido relacionado
La actualidad más candente
La actualidad más candente (20)
Similar a Restorative Materials in Pediatric Dentistry: Recent Advancements
Similar a Restorative Materials in Pediatric Dentistry: Recent Advancements (20)
Último
Último (20)
Restorative Materials in Pediatric Dentistry: Recent Advancements
- 1. RESTORATIVE MATERIALS USED IN PAEDIATRIC DENTISTRY (Along with Recent Advancements) GUIDED BY - PRESENTED BY - Dr. Jitendra Kamini Singh B.D.S. 3rd year
- 2. CONTENTS INTRODUCTION: NEED FOR DECIDUOS DENTITION IN CHILDREN NATURE OF RESTORATIVE MATERIALS USED IN PAEDIATRIC DENTISTRY REQUIREMENT OF AN IDEAL RESTORATIVE MATERIAL VARIOUS RESTORATIVE MATERIALS USED IN PAEDIATRIC DENTISTRY: GLASS IONOMER CEMENT COMPOSITE RESINS AMALGAM LINING MATERIALS
- 3. CONTENTS RECENT ADVANCEMENTS IN RESTORATIVE MATERIALS USED IN PAEDIATRIC DENTISTRY • ALTERNATIVE TO AMALGAM • RECENT ADVANCEMENTS IN FIELD OF COMPOSITE RESIN RESTORATIVE MATERIAL • RECENT ADDITIONS TO G.I.C. • SMART MATERIALS
- 4. INTRODUCTION : NEED FOR RESTORATION IN PAEDIATRIC DENTISTRY • Preservation Of Deciduous Teeth Until Their Normal Exfoliation Is Essential Because: 1)They are considered essential in the development of the oral cavity and maintaining a healthy oral environment free of pain. a) In adulthood , the face and jaws are smaller size are present ,which are known as Deciduous or Primary teeth. b) With the growth , the jaw bones grow in size but the teeth once fully formed do not grow in size. Hence , permanent teeth of large sizes erupt in oral cavity, replacing deciduous teeth of smaller size.
- 5. INTRODUCTION : NEED FOR RESTORATION IN PAEDIATRIC DENTISTRY 2) They provide a guide for permanent tooth eruption. 3) The root of deciduous teeth provides an opening for the permanent teeth to erupt. 4) These teeth also help in speech and mastication. 6) Promote an aesthetic appearance. 7) Maintenance of arch length.
- 6. Nature of Restorative Materials Used In Pediatric dentistry In view of the limited lifespan of the deciduous teeth, plastic restorative materials are used, which can be placed directly into the cavity, especially for the first molars because of the difficulties which may be encountered in placing restorations such as gold inlays or gold foils in a young patient.
- 7. Requirements of an Ideal Restorative Material 1) Restoration of aesthetic 2) Maintenance of physical strength of the crown. 3) Preserving the anatomy of the occlusal surface and thus preserving the inter arch relationship with the opposing and adjacent teeth. 4) Prevention of further ingress of bacteria or their byproducts into the micro spaces between the restoration and tooth. 5) Long term adhesion between the restoration and tooth to ensure complete isolation.
- 8. Various Restorative Materials used in Pediatric Dentistry 1) Glass Ionomer Cement 2) Composite Resins 3) Amalgam
- 9. Glass Ionomer Cement This material was developed by Wilson and Kent in 1971. • These are adhesive tooth color anticariogenic restorative material. • It can be used as a luting cement, a lining under another restorative material or as a restoration. • It also known as Poly Alkenoate Cement and Alumino Silicate Polyacrylic Acid (ASPA)
- 10. Classification of Glass Ionomer Cement – On the basis of use: • Type I: For Luting Cements • Type II: For Restorations • Type III: Liners and Bases • Type IV: Fissure Sealants • Type V: Orthodontic Cement • Type VI: Core Build Up • Type VII: Fluoride Releasing • Type VIII: ART (Atraumatic Restorative Technique) • Type IX: Deciduous Teeth
- 11. Classification of Glass Ionomer Cement • According to other uses: – For Intermediate Restoration – In Sandwich Technique (As Adhesive Cavity Liners) – In ART (Atraumatic Restorative Technique) – In Deciduous Tooth
- 12. Classification of Glass Ionomer Cement • Chemical Classification 1) Conventional Glass Ionomer Cement 2) Resin Modified Glass Ionomer Cement (Conventional with addition of HEMA) 3) Hydrate Ionomer Cement (Also known as Dual Cure Glass Ionomer Cement) 4) Tri Cure Glass Ionomer Cement 5) Metal Reinforced Glass Ionomer Cement
- 13. Classification of Glass Ionomer Cement • Widely Accepted Classification of Glass Ionomer Cement • Type I: Luting Used in cementation of crowns, bridges and orthodontic devices Powder : Liquid is approximately 1.5:1 Radio Opaque • Type II: Restorative • Type IIA: Restorative Aesthetic – Used in all types of aesthetic restoration – Auto Cure or Resin Modified – Powder: Liquid is 3:1 or greater – Radio Opaque generally – High physical properties
- 14. Classification of Glass Ionomer Cement – Type IIB: Restorative » Restoration under high occlusal load » Auto cure or resin modified » Powder : Liquid is 3:1 or greater » Radio Opaque » Used as a denting substitute or as interim restoration. • Type III: Lining or Base – Simple lining under metallic restoration – Powder: Liquid is 1.5:1 – Auto Cure – Radio Opaque – High Strength bases for lamination technique.
- 15. Composition of Glass Ionomer Cement Glass = Formulation of glass powder Ionomer = Ionomeric Acid with Carboxyl group The three essential constituents of dental Ionomer glasses are – Silica (Si02), Alumina (Al2O3) and Calcium Fluoride (Cafl2) or Fluorite CaF2) Glass Ionomer Cement is a product of an Acid-Base reaction.
- 16. Composition of Glass Ionomer Cement Powder • The basic component is a Calcium Alumino Silicate Glass containing fluoride. Its constituents are: Calcium Fluoro Alumino Silicate Glass, Lanthanum, Strontium, Barium or Zinc Oxide • It is possible to substitute the Calcium with Strontium and the percentage of Fluoride in the formula can be varied. • Phospate can be added to decrease the melting temperature and modify the setting characteristics. • Fine colloidal Silver can be sintered to the particles and amalgam alloy particles can be added to the mix in an attempt to enhance the properties.
- 17. Composition of Glass Ionomer Cement Liquid Liquid is essentially a poly Alkenoic Acid. • The usual acid is 40-55% solution of 2:1 poly acrylic or Itaconic acid copolymer in water or a copolymer of malic acid and poly acrylic acid. • Its constituents are – – Poly Acrylic Acid – Itaconic Acid (Increases the reactivity and reduces the viscosity and tendencies for gelation) – Maleic Acid or Tricarboxylic Acid – Tartaric Acid – Improves handling characteristics, increases viscosity and working time and reduces setting time.
- 18. Composition of Glass Ionomer Cement Role of Fluoride in Glass Ionomer Cement • It lowers the temperature of fusion • Improves the working characteristics of the cement paste • It increases markedly the strength of the set cement • In moderate amount it enhances translucency • Contributes to therapeutic value of the cement by releasing fluoride over a prolonged period.
- 19. Setting reaction of Glass Ionomer Cement – When the glass ionomer cement powder and liquid are brought together to form a paste the glass powder which is basic reacts with liquid, that is Acid, to form a salt hydrogel which is the binding matrix – Here water in the reaction medium forms a part of Hydrogel.
- 20. Different Stages in the Setting reaction – Initially the surface of glass is attacked resulting in decomposition of glass and release of aluminum and calcium ions – These aluminium and calcium ions then migrate into the aqueous phase of the cement – As the reaction proceeds the concentration of ions and the viscosity of the paste increases – Initially calcium ions form part of the cross linkage with poly acrylic acid change to form solid mass.
- 21. Different Stages in the Setting reaction • Later within next 24 hours new phase is formed with aluminium ions becoming bound to cement matrix leading to more rigid set cement • Calcium polyacrylate is responsible for final hardening of the matrix. • Sodium and Fluoride do not participate in the cross linking of the cement • Some sodium ions may replace Hydrogen ions of carboxylic group, but rest combine with fluoride to form NaFl which is uniformly dispersed
- 22. Different Stages in the Setting reaction within the cement. – Unreacted glass particles are coated by silica gel (that form during removal of the cations from the surface of the particles) – Final set cement consists of agglomerated unreacted powder particles surrounded by a silica gel in an amorphous matrix of hydrated calcium and aluminium polysalts. ROLE OF MOISTURE CONTAMINATION AND DEHYDRATION During the setting process the cement should to protected from two extremes-dessiccation and aqueous environment.
- 23. ROLE OF MOISTURE CONTAMINATION AND DEHYDRATION • This can be achieved in an atmosphere of 80% relative humidity. • The cement should be protecting by varnish or petroleum jelly. • After initial set but before the cement is fully hardened a proportion of cement containing Aluminium Calcium , Fluoride and Polyacrylate containing ions are in a soluble form and so can be dissolved out of the cement by aqueous fluid leading to permanently weakened cement.
- 24. ROLE OF MOISTURE CONTAMINATION AND DEHYDRATION • If at this stage water is released out due to excessive drying restoration will lose aesthetic appeal ,shrink and become brittle. • It may take one hour until the cement remains vulnerable to moisture. • Hardening continues for 24 hrs. • Slow maturation continues over the period of months and becomes more rigid and gather strength.
- 25. FACTOR AFFECTING SETTING CHARECTERSTICS OF GLASS IONOMER CEMENT Role Of Fluorides: Fluoride forms metal complexes that restore the binding of cations to anionic sites on the polyelectrolyte chain and thereby delaying gelation and prolonging working time. It also delays pH dependent gelation . ROLE OF TARTARIC ACID It improves manipulation of the cement and increases the strength of set cement.
- 26. FACTORS AFFECTING RATE OF SETTING OF GLASS IONOMER CEMENT • Glass composition -especially the Al2O3 / SiO2 ratio and fluoride content. • Fluoride prolongs the working time. Increased ratio –faster is the set , shorter is the working time. • Particle size- Finer the particles size-Faster is the set and shorter is the working time.. • Addition of tartaric acid sharpens the set without shortening the w.t • Relative proportion of constituents in the cement mix i.e. glass / polyacid /tartaric acid / water . • Greater proportion of glass and lower is the working time. • Temperature of mixing-In higher temperature the faster is set shorter is w.t.
- 27. PROPERTIES OF GLASS IONOMER CEMENT •Physical Properties •Sets rapidly in the mouth •Initial compressive strength is low (24 hrs.)-6.6MPa •Hardness-70KHN •Solubilty-0.7% •Bioactive and possesses chemical bonding with the tooth. •Coefficient of thermal expansion is close to that of tooth causing less micro leakage around the restoration.
- 28. PROPERTIES OF GLASS IONOMER CEMENT ESTHETICS Translucent material Color is more stable. Resistance to stain is dependent on good surface finish. ADHESION Permanently adheres to the unreacted enamel and dentin chemically. Principle barrier to adhesion is water. Mechanism of adhesion-chelation of carboxyl group of the polyacids with the calcium ions in the apatite of enamel and dentin forming strong ionic bonds which increases the strength as the material sets. Surface conditioning also improves adhesion.
- 29. PROPERTIES OF GLASS IONOMER CEMENT BIOCOMPATIBILTY o Excellent marginal seal and fluoride release-Reducing the risk of secondary caries. o Continuous Fluoride release occurs around the restoration- tooth interface(3mm) for a period of 18 months. o Acid groups are attached to the polymer molecule which have limited diffusibilty , hence the pulp affects are limited to areas immediate . It adjacent to the material. o When fluid filled dentinal tubules are in direct contact with the unset material and problem occurs o High ionic concentration in the material cause dentinal fluid to rapidly diffuse outward into the cement producing a change in the pulpal pressure creating pain and sensitivity. o Hydrogen ions may move into the tubules towards the pulp and cause chemical irritation. o When the dentin thickness is less there is less fluid to buffer the acid. o Inflammatory response of pulpal tissue towards G.I.C. is more than Zinc Phospate cement and resolves in 20 days without formation of reparative dentin. o It is said that lining of calcium hydroxide or zinc oxide eugenol is required , when less than 0.5-1mm of sound dentin remains over the pulp.
- 30. MODIFIED GLASS IONOMER CEMENT ”ANHYDROUS” • In this modification , the liquid is delivered in a freeze dried form that is incorporated in powder. The liquid to be used is clean water only and this may enhance shelf life and facilitating mixing. • Another alternative is to use a dilute tartaric acid as the liquid with dehydrated polyacrylic acid included in the powder. • These alternatives makes it possible to use a polyacrylic acid with a higher molecular weight, thus improving physical properties. • The term anhydrous is actually a misnomer as its not possible for ion transfer to occur in any material in the absence of water.
- 31. RESIN MODIFIED GLASS IONOMER CEMENT • These are materials which have a small quantity of a resin into the liquid formula. • Less than 1% of photo initiators are allowed for the setting reaction to be initiated by light of the correct wavelength . • The advantages include early resistance to water uptake in the nearly set cement as well as enhanced translucency. • The resin utilized in these materials is Hydroxy Ethyl Meth Acrylate(HEMA) and its incorporated into the liquid in about 15-25% so as to have a powder liquid ratio of about 3:1
- 32. NANO IONOMERS • Nano-ionomers delivers greater wear resistance , esthetics and polish compared to other glass ionomers while affecting fluoride release similar to conventional and resin modified Glass ionomer • In the first ever paste glass ionomer restorative featuring nano filler technology, the product is designed to be quickly and easily be mixed and dispensed using dispenser. • Eg.- Ketac Nano Light Curing Glass Ionomer Restorative Material.
- 33. COMPOMER • This is the term developed by manufacturer with a claim to incorporate with a composite resin • A compomer is a composite resin that was an ionomer glass which is the major constituents of a glass ionomer as the filler. • There is also a small quantity of a dehydrated polyalkenoic acid incorporated with the filler particles. • The filler particles are held within an anhydrous resin matrix and there is complete absence of water. • Hence there can be no ion exchange, acid/base setting reaction and material remains inert.
- 34. COMPOMER • The setting reaction is lightly activated and there has been a degree of water uptake into the restoration. • a composite resin that was an ionomer glass which is the major constituents of a glass ionomer as the filler. • There is also a small quantity of a dehydrated polyalkenoic acid incorporated with the filler particles. • The filler particles are held within an anhydrous resin matrix and there is complete absence of water. • Hence there can be no ion exchange, acid/base setting reaction and material remains inert. • The setting reaction is lightly activated and there has been a degree of water uptake into the restoration.
- 35. COMPOMER • After water uptake there will be an ion exchange between the glass and the rehydrated polyalkenoic acid followed by a low grade fluoride release , but this will not be sustained at a higher level. • Since Fluoride uptake cannot take place a compomer cannot be regarded as a fluoride reservoir. • The most significant difference between the two materials is the absence of ion exchange adhesion. • The adhesive system used with a compomer is based on the acid etch resin bond system found with all composite resins • The %age of filler content is relatively low compared to hybrid composite resins. However ,both water uptake and wear factor are relatively high.
- 36. CERAMIC REINFORCED GLASS IOMOMER • Ceramic reinforced polymer G.I.C. featured stronger compressive , flexural and tensile strength as compared to Amalgam. • The main advantages is its excellent wear characteristics. • Some other features include superior radio-opacity, high level of Fluoride release, good biocompatibility and natural adhesion to tooth structure. • Material is excellent for core build-ups and posterior restorations. • Its available in white and a universal tooth shade. • Also , water mix and powder/liquid versions are available. • This material was mainly designed to match the strength and durability of amalgam . The presently available ceramic reinforced G.I.C. includes Amalgomer-CR
- 37. SETTING RECTION OF RESIN MODIFIED GLASS IONOMER The setting reaction of resin modified glass ionomer is similar to the acid base reaction though at a slightly slower pace. The usual ionomer salt hydrogel will form along with a poly HEMA matrix will be stimulated by light activation subsequently an oxidation / reduction reaction resin chains so that in the long run the entire restoration will be set . This has been designated as , “Tri-cure setting reaction”.
- 38. FACTORS AFFECTING SETTING RATE OF R.M.G.I. • Temperature of mixing slab: Lower the temperature of mixing slab , The longer the working time and vice versa. • However the temperature should always be above the dew point • Powder-Liquid ratio- • The higher the powder content the higher the physical properties. • However the care should be taken too ensure that the materials are properly dispensed before mixing. • Setting reaction of compomer. • These are essentially two different systems for initiating polymerizations in a composite resin. • The original material were all chemically activated , however they exhibit an undesirable color shift. • Subsequently, a system for light activation was developed and this has proven to be relatively color stable. • Its also possible to combine the two systems.
- 39. STEPS INVOLVED IN CLINICAL PLACEMENT OF GLASS IONOMER CEMENT Shade selection Isolation of tooth , rubber dam is the material of choice. Cavity Preparation – the objective is to remove all caries and unsupported enamel. Minimal extension is the keyword. If the dentin thickness is 0.5-1mm,lining of calcium hydroxide should be placed. Surface prep-The surface smear is removed by pumice wash. The tooth surface is conditioned with 10% polyacrylic acid application for 10-15 seconds ,followed by 30 seconds water rinse.
- 40. STEPS INVOLVED IN CLINICAL PLACEMENT OF GLASS IONOMER CEMENT Cement is mixed according to the manufacturer instructions It should be mixed rapidly to gain working time and should not be more than 45-60 seconds. The tooth should be isolated all through. Place matrix wherever possible and fill the cavity with G.I.C. Remove the matrix and immediately protect it with waterproof material like varnish or Vaseline. Trim the excess with scalpel, Rotary cutting instruments should be used.
- 41. STEPS INVOLVED IN CLINICAL PLACEMENT OF GLASS IONOMER CEMENT After the removal of excess material a layer of protective material a layer of protective material is re applied. Finishing and polishing is done after 24 hrs. Re-apply the protective material after finishing and polishing .
- 42. CRITICAL PROCEDURES FOR GLASS IONOMER RESTORATIONS Surface conditioning to remove smear layer P:L ratio must be maintained. Mixing time- not more than 45-60 secs and surface should be glossy due to polyacid that has not participated in the reaction which helps in bonding.
- 43. CRITICAL PROCEDURES FOR GLASS IONOMER RESTORATIONS Placement of material-with plastic instrument or injected. Mixed material should be used within 5 minutes. Surface finishing-Delayed for 24 hrs. MODIFICATIONS OF GLASS IONOMER CEMENT Its done to improve strength, fracture toughness and resistant to wear. SILVER ALLOY ADMIX-Mixing spherical amalgam alloy powder with Type-I glass ionomer. B.CERMET FUSING GLASS POWDER TO SILVER PARTICLES. C.RESIN MODIFIED G.I.C.- to overcome moisture sensitivity and low early strength. Also, called as Light cured , Dual cured (LC and Acid Base Reaction) , Tricure (dual cure and chemical cure) resin ionomer compomers or hybrid ionomers.
- 44. COMPOSITION OF RESIN MODIFIED G.I.C. Powder-Ion leachable glass Initiator for light or chemical cure or both. Liquid-Water Polyacrylic acid/Polyacrylic acid with carboxylic group modified with methacrylate and Hydroxy ethyl meth acrylate monomer.
- 45. SETTING REACTION OF RESIN MODIFIED GLASS IONOMER CEMENT Physical Properties The difference is due to presence of polymerized resin and less amount of water and carboxylic acid in liquid. Tensile strength is higher than that of conventional G.I.C. Greater amount of plastic deformation.
- 46. SETTING REACTION OF RESIN MODIFIED GLASS IONOMER CEMENT Bonding similar to conventional G.I.C. Higher bond strength compared to composite resin. Greater degree of shrinkage due to polymerization, lower water and carboxylic content. Reduced water sensitivity. Transient temperature increase during polymerization.
- 47. ADVANTAGES AND USES OF GLASS IONOMER CEMENT •Extended working time •Improved physical properties •More resistant to dehydration and cracking. •It is a tooth colored material. •It will adhere directly to both enamel and dentin through an ion exchange method. •Its biologically active, as its capable of releasing fluoride , calcium and phosphate ions.
- 48. DISADVANTAGES OF GLASS IONOMER CEMENT •Its physical properties are not sufficient to withstand heavy occlusal load in large restorations. •Resistance to fracture is one of the main limitation to the use of G.I.C.. Its generally quite satisfactory for one surface lesion , but a two surface lesion is always at risk. •Resistance to fracture also depends on the particle size of the powder and particle size distribution.
- 49. DISADVANTAGES OF GLASS IONOMER CEMENT Improvement in enhancement of strength of G.I.C. can only be of chemical origin or through of microporosities. Resistance to abrasion and wear is a little less than that of a composite resin. They also remain susceptible to dehydration throughout the lifespan, so patients with a dry mouth, should not have their teeth restored with glass ionomer.
- 50. COMPOSITE RESINS Composite Resins were developed by R.L.BOWEN. Since epoxy reins have some disadvantages or shortcomings like slow cure and some tendency to discolor, So , He combined the advantages of epoxy resins and acrylic resins leading to the development of BIS-GMA molecule . It has an aromatic ester of Dimethacrylate with epoxy resin as the backbone and acrylic as the functional reactive group. Composite Resins are the only restorative material other than glass ionomer cement ,to that has the ability to restore esthetics and to develop and maintain adhesion in oral environment.
- 51. CLASSIFICATION OF COMPOSITE RESINS Classification Based on Filler Particle Size: Megafillers >100 microns (megafilI) Macrofillers =10-100 microns(macrofill) Midfillers =1-10 micron (microfill) Minifillers =0.1-1 micron (minifill) Microfillers =0.01-0.1 micron (microfill) Nanofillers =0.05-0.01 microns( Nanofill) Picofillers =0.005 microns
- 52. CLASSIFICATION OF COMPOSITE RESINS Heavily Filled Materials contain inorganic filler about 75 % Wt. or more Lightly Filled Materials contain inorganic filler about 66 Wt. %
- 53. CLASSIFICATION OF COMPOSITE RESINS CLASSIFICATION BASED UPON MASS PARTICLES SIZE OF THE MAJOR FILLER 1.Conventional=8-12 micron meter 2.Small Particle=1-5 micron meter 3.Microfilled=0.04-0.4micron meter 4.Hybrid=0.1-1.0micron meter.
- 54. CLASSIFICATION OF COMPOSITE RESINS Classification based upon the method of polymerization Self cure Light cured Composition Of composite materials Resin Matrix : BIS-GMA is the most commonly used resin followed by Urethane Dimethacrylate Diluent monomer like methyl methacrylate monomer or Dimethacrylate monomers such as : TEGDMA(TRIETHYL GLYCOL DIMETHACRYLATE),are used to attain higher filler levels and to produce pastes of clinically usable consistencies. TEGDMA allows extensive cross linking to occur between chains resulting in a matrix that is more resistant to solvents , but also increase the polymerisation shrinkage. Filler Particle: Improves the properties of the matrix material. Reduces polymerization shrinkage, Reduces polymerization ,shrinkage, Reduces water sorption and coefficient of thermal expansion.
- 55. Composition Of composite materials Improves Tensile strength , compressive strength and modulus of elasticity and abrasion resistance. Materials used as fillers are- Colloidal silica , Quartz , Barium , Strontium , Zirconium .
- 56. Composition Of composite materials : Materials used as fillers QUARTZ It has been extensively used as filler in particularly in conventional composites. Advantages : Its chemically inert but its so hard that its difficult to polish and may abrade opposing teeth are restoration. Other materials are not as stable as quartz and may leach out into aqueous medium. Translucency of the filler must be similar to that of tooth structure and its index of refraction must closely match that of resin. For BIS-GMA+TEGDMA combination refractive index is about 1.5 Most of the glass or quartz that are used as fillers have R.I. of 1.5
- 57. Composition Of composite materials Coupling Agent It provides a bond between the resin matrix and fillers , thus improving the physical and mechanical properties and providing stability by preventing water from penetrating along the resin filler interface. Eg. - Organosilanes are commonly used 1) Titanates 2) Zirconates INHIBITORS Hydroquinones butylated hydroxytoluene (<0.01%) Minimizes or prevents spontaneous polymerization . It reacts with free radicals if formed.
- 58. Composition Of composite materials UV Absorbers To improve color stability Eg - 2-Hydroxy-4-Methoxy Benzophenols Activators For self cure-Tertiary amine For Light Cure-Light Initiators Self Cure- Benzoyl Peroxide , Light CURE-Alpha diketones like camphor quinones, UV light- Benzoin Methyl Ether, Pigments
- 59. PROPERTIES OF COMPOSITE RESINS •Linear coefficient of thermal expansion is twice as much as the value of Amalgam and 3-4 times greater than that for tooth structures. •Most composites can be practically cured only to levels of 55-65% conversion of monomer sites. Usually due to inadequate curing energy from visible light cure unit and is improved by post curing.
- 60. PROPERTIES OF COMPOSITE RESINS •Water absorption swells the polymer portion and promotes diffusion and desorption of any unbound monomer . Water plasticizes the composite and chemically degrades the matrix into the monomer . Increased filler content lower is water absorption. •Microfill composites are the least wear resistant. •Composite with high matrix content and self cured have more tendency to undergo yellowing . Addition of white light absorbs and antioxidants reduce the chance of yellowing. •Beveling tend to blend any color difference associated with margins and provide more surface area of bonding. •Good Marginal integrity- •Butt joint margin wear slowly but create a meniscus appearance against enamel . Beveling produces thinner ledges of material that are prone to fracture. •Biocompatible, but unemployed materials are potentially cytotoxic. They are very poorly soluble in water and are polymerized into a bound state before dissolution or diffusion.
- 61. PROPERTIES OF COMPOSITE RESINS •Compared to unfilled resins ,filled resins are more stronger ,increased modulus of elasticity(increased modulus of elasticity= less is the flexibility and vice versa) , good abrasion resistance and lower coefficient of thermal expansion.
- 62. CLINICAL STEPS • 1)Etching and Bonding • 2)Delivery and Placement • 3)Incremental Build Up • 4)Depth of cure
- 63. CLINICAL STEPS - Etching & Bonding An essential pre-requisite for the micro-mechanical attachment is that the enamel should be etched with 37% Orthophosphoric acid. To demineralize the enamel to a depth of 20-30 mm and render it porous. A very low viscosity unfilled resin is then flowed over the surface and allowed to soak into the porosities for about 30 secs. before its light activated . Composite resin is then built over resin bond. Pre-Requisite for etching First the enamel at the cavity margins must be fully mineralized and based on healthy dentin. There must be no crack on the tooth. Best union will be at the ends of enamel rods rather than along the long sides , so its desirable to develop a reasonably long bevel at the cavosurface margin
- 64. CLINICAL STEPS - Etching & Bonding In juvenile enamel there is less mineral or more organic collagen. There will be more water present because of the presence of dentinal tubules and their direct access to pulp and the amount of fluid and their direct access to pulp and the amount of pulp and the amount of fluid flow will only be enhanced following acid etching because it will lead to opening and funneling of tubules Even a small cavity will be relatively close to pulp and therefore there will be a greater density of tubules on the floor of cavity and a relatively greater fluid flow.
- 65. CLINICAL STEPS - Etching & Bonding The goal of resin dentin bonding agent is to attach composite resins to healthy dentin and to seal the dentinal tubules against the entry of bacteria and their toxins. This will avoid post restoration sensitively caries and loss of restoration. Its possible to demineralize some of the dentin.
- 66. CLINICAL STEPS - Etching & Bonding PRINCIPLES TO SUCCESSFUL RESIN DENTIN BONDING Dentin should be etched to remove smear layer and dentin tubule plugs Etching should be sufficient to demonstrate the surface layer of intertubular and intratubular dentin leaving collagen fibers exposed and available for a mechanical interlock with resin. Surface should be washed thoroughly to remove all remaining etchant.
- 67. CLINICAL STEPS - Etching & Bonding Surface should remain wet but not flooded. Apply a hydrophilic primer containing acetone or similar to guide and facilitate penetration of resin adhesive around the exposed collagen fiber. Finally apply the resin adhesive and cure before applying composite resins.
- 68. CLINICAL STEPS : Delivery &Placement Chemical cure and the dual core materials will be packaged as a paste /paste system or a powder / liquid system. To ensure proper adaptation to the cavity floor ,its desirable to place the freshly mixed material into the disposable syringe and then temp the material into the cavity with a small plastic sponge . Light activated materials will always be delivered in light proof carpules or which have been loaded under vacuum. This means they are free of porosity at the time of delivery.
- 69. CLINICAL STEPS : Delivery and placement Placement must be undertaken with care and attention to detail with particular reference to the depth of cure available through a curing light , by checking periodically to ensure that lower layers are also cured adequately. INCREMENTAL BUILD UP Due to problems posed by light activation of composite resins , its essential to any restoration deeper than that about 2.0mm. Incremental placement means placement of the composite in small quantity in selected areas of the cavity and then directing the light activating unit in such a way that while curing the resin will shrink towards the tooth structure rather than away from it.
- 70. CLINICAL STEPS : Delivery and placement • Its recommended that increments be as small as possible . The activator be applied from many positions during Buildup. • DEPTH OF CURE • In a child , its imperative that the activator light be placed within 1-2mm of the surface of the newly placed restoration , otherwise the depth of cure will be limited. • Factors to be considered while curing • The degree of cure will decrease with increased depth of cure, greater the translucency deeper the cure. • Light activator units vary in their light output over time as well as with power fluctuations.
- 71. CLINICAL STEPS : Delivery and placement • Tip of the light source should be placed as close as possible to the restoration and should never be more than 4mm away. • The depth of cure should be measured from the face of the activator light. • Curing through tooth structure will reduce the depth of cure to the same extent as if curing through a composite resin of similar opacity. LIMITATIONS OF COMPOSITE RESINS • Both resins and fillers are used anhydrous and completely inert .However , some of the minor constituents such as HEMA , have been identifiable in the pulp tissue in certain mer chain may be an irritant to the pulp in circumstances and care should be exercised in its use. • Any unreacted polymer chain may be an irritant to the pulp and lead to post insertion sensitivity. • The tissue cells respond less favorably to composite resins then do to glass ionomer and it has been postulated that incomplete cure of resin is the prime cause of this.
- 72. CLINICAL STEPS : Delivery and placement CLINICAL CONSIDERATIONS • IN Pediatric dentistry , a restoration will not be expected to last for more than few years , so a limited amount of wear an be tolerated. • However , a relatively large setting shrinkage will be undesirable. • Esthetics and fracture resistance will not be of great significance but the ability to bond effectively to both the enamel and dentin will not be relevant • A relatively shorter concentration span from the patient as well as limited access to oral cavity , to simplicity of placement technique will be important
- 73. CLINICAL STEPS : Delivery and placement • The operator must be aware of the relevant properties of both composite resins and G.I.C. , so that a logical decision regarding use can be made.
- 74. Amalgam • Silver Amalgam restorative material is obtained by the trituration of Amalgam alloy with mercury. • It’s the most reliable and inexpensive dental restorative material of all.
- 75. TYPES OF DENTAL AMALGAM ALLOYS Based On the content: • High Copper alloy : copper content more than 12% • Low copper alloy : copper containing less than 6% • Gallium alloy
- 76. TYPES OF DENTAL AMALGAM ALLOYS Based on particle shape and type • Lathe cut: Irregularly shaped filings produced by cutting an ingot of alloy on a lathe. • Spherical particles: Produced by atomizing the alloy whilst still liquid into a stream of inert gas. Based on Zinc content • Zinc containing :Alloys with more than 0.01% Zinc • Zinc free: Alloys with less than 0.01% Zinc
- 77. TYPES OF DENTAL AMALGAM ALLOYS Based on Gamma2 content • Amalgams may be classified as gamma 2 containing or gamma2 free • A) low cu amalgam contain the Sn-Hg phase which is called Gamma2 phase to distinguish it from gamma2 phase of silver tin and silver mercury alloy systems. • B)Within several hours after amalgamation all correctly manipulated High cu amalgams are gamma2 free.
- 78. TYPES OF DENTAL AMALGAM ALLOYS According to size • Fine cut (particle size is 36 micron) • Micro cut(particle size is 26 micron) According to the method of dispensing • As powder and liquid • As a capsule • As pellets or pills of alloy powder(3% of the Hg is mixed with the alloy powder and this facilitates faster reaction)
- 79. PROPERTIES OF AMALGAM • Increased mercury – leads to increased expansion , creep and corrosion. • Compressive strength-Admixed is 430 Mpa after 7 days • Tensile strength-Admixed is 50MPa after 24 hrs. • Surface hardness – 3-8 mins. • Setting Time-5-10 mins. • Increased expansion is due to increased mercury ,short trituration , low condensation pressure and water contamination. • Creep is associated with increased or decreased trituration , time lags between trituration and condensation , increased mercury , less condensation force.
- 80. Criterion for selection of Amalgam Alloy • Small particles are selected ; Better strength, easy to carve ,good surface finish , good marginal adaptation , poor corrosion resistance. • Spherical is selected: Better strength , easy to curve , good finish , good marginal adaptation , good corrosion resistance and easy condensation (Lathe cut resists condensation, may result in poor corrosion resistance , porous restoration with rough surface and poor marginal adaptation).
- 81. Criterion for selection of Amalgam Alloy • High copper is preferred : Better strength less creep , good corrosion resistance due to absence of alpha2 phase. DRAWBACKS OF SILVER AMALGAM • Good conduction of Heat(Requires good insulation). • Poor marginal adaptation : so varnish is applied. • Poor esthetics
- 82. DRAWBACKS OF SILVER AMALGAM • Poor modulus of elasticity , proportional limit, and tensile strength. • Electrolyte corrosion • Poor adhesion to tooth structure. • Ditched amalgam
- 83. CONDENSATION AND CARVING OF SILVER AMALGAM • Amalgam alloy and mercury is dispensed and mixed as per the manufacturer’s instructions • Material is loaded into the amalgam carrier • Proximal box is first filled in a class II cavity • In other cavities its started from one side slowly moving and filling the entire cavity • The material is firmly condensed into the cavity. • Amalgam is condensed using condensers. • Initial condenser should be small enough to condense the material into the line angles. • Each condensing stroke should be small enough to condense the material into the line angles. • Each condensing stroke should overlap the previous condensing stroke to ensure that entire mass is well condensed • Cavity is overfilled and condensed with a large condenser. • Parallelogram condenser is used to condense narrow occlusal cavity.
- 84. CONDENSATION AND CARVING OF SILVER AMALGAM • This is followed by pre-carve burnishing of the amalgam . Its form of condensation done with a large ball burnisher , using heavy strokes mesiodistally and faciolingually . This helps to remove all she excess Amalgam and blends the restorative material with cavity margins. • Initial gross carving of the restoration is done followed by fine carving of cuspal inclines , triangular fossa and grooves . Hollenbeck , wards or diamond amalgam carvers are used for the purpose of carving amalgam • Wedges and matrix placed can be removed after initial carving • Post carve burnishing is done using a ball burnisher : It involves the light rubbing of the carved surface to improve smoothness and produces satin appearance.(not a shiny).insertion. • Finishing and polishing is done after 24 hrs of insertion.
- 85. CONDENSATION AND CARVING OF SILVER AMALGAM • Mercury Hygiene - Precautions that should be taken regarding the mercury exposure in dental office staff and the patients are: • When removing an old amalgam restoration rubber dam should be in place and high vacuum evacuation should be used . Glasses and disposable free masks are worn • Amalgam capsules should be preferred to the conventional dispensing • Closed amalgamator should be used • Free mercury and amalgam scraps should be stored in an unbreakable tightly closed container away from any source of heat preferably in water. • Since, mercury vaporizes at room temperature operatories should be well ventilated to minimize the mercury level in air. • Its necessary to place a lining material on the floor of the cavity prior to placement of final restoration.
- 86. LINING MATERIALS MATERIALS USED IN PAST AND REASONS FOR USE 1)ZINC PHOSPHATE CEMENT • This was used extensively may years ago on the theory that it was strong enough to accept the load imparted to the dentin by condensation of an amalgam restoration. • It was accepted that there was no therapeutic value in this material and in fact , it has shown to be mildly irritating if placed close to the pulp. • Its outdated in the present.
- 87. LINING MATERIALS : MATERIALS USED IN PAST AND REASONS FOR USE 2) ZINC OXIDE EUGENOL This became popular because of the antibacterial property of Eugenol as well as the sedative effectiveness of Zinc oxide • Its used a s a temporary sedative dressing over a large cavity with a n inflamed pulp. • Its effective as it provides a seal around the periphery of a cavity as a bacteria can not penetrate through Eugenol. • Fast setting type were developed to allow this to be used alone as a lining but as its relatively weak , it does not offer support for an amalgam restoration placed over the top.
- 88. LINING MATERIALS : MATERIALS USED IN PAST AND REASONS FOR USE RECENT MODIFICATION • Embonte Zinc Oxidizing Eugenol Temporary Cement which is conveniently packaged in an Auto mix delivery system. • This is engineered with pure essential oil extracts. • Creamy consistency of Embonte Auto mix allows easy application from static mixing tip to crown.
- 89. LINING MATERIALS : MATERIALS USED IN PAST AND REASONS FOR USE 3) CALCIUM HYDROXIDE • Used as a liner because of its antibacterial property as well as because of the theory that the excess calcium ions present in the cement would be available to the pulp and would encourage remineralization within the pulp chamber. • Its very alkaline with a pH 13 ensures the fact that its very presence will make the bacteria unable to thrive and help in stabilizing conditions on the floor of the cavity.
- 90. LINING MATERIALS : MATERIALS USED IN PAST AND REASONS FOR USE • If placed to close necrosis of the subjacent soft tissue , but in the absence of bacteria the pulp is likely to survive beyond the necrotic area. • It will then lay down a calcific barrier a short distance away and it was assumed that it was calcium ions from the lining which promoted the repair. 4 ) GLASS IONOMER This is now a material of choice for lining the cavity because its an effective barrier to temperature change and also – Gallium alloy : A mercury free metallic substitute to silver amalgam , provides barrier to temperature change and also provides ion exchange adhesion that is most effective barrier to micro leakage of bacteria under a restoration
- 91. RECENT ADVANCEMENTS IN RESTORATIVE MATERIALS USED IN PEDIATRIC DENTISTRY 1) ALTERNATIVE TO AMALGAM- • In view of hazards of mercury present in amalgam a mercury free alloy has been suggested . • Eg. - Gallium alloy : A mercury free metallic substitute to silver amalgam
- 92. RECENT ADVANCEMENTS IN RESTORATIVE MATERIALS USED IN PEDIATRIC DENTISTRY 2) RECENT ADVANCEMENTS IN FIELD OF COMPOSITE RESIN RESTORATIVE MATERIAL A) Dentil flow- Its a new flowable composite having acceptable shear bond strength for bonding orthodontic bracket , when used with an intermediate unfilled low viscosity resin. B) Packable composites - Its obtained by varying particle size and size distribution through the water uptake and wear factor will remain standard and acceptable . Material is less sticky
- 93. RECENT ADVANCEMENTS IN FIELD OF COMPOSITE RESIN RESTORATIVE MATERIAL C) TETRIC EVOFLOW -It’s the new nano optimized flowable composite form. • Ivoclar vivadent and successor product of Tetric flow • Characterized by optimum surface affinity. • Penetrates even into areas that are difficult to reach.
- 94. RECENT ADVANCEMENTS IN RESTORATIVE MATERIALS USED IN PEDIATRIC DENTISTRY 3) RECENT ADDITIONS IN G.I.C. a) Interval II Plus- Interval II Plus is a dependable , one component , ready mixed , temporary filling material with glass ionomer and leachable fluoride. • With no ZnO /Eugenol , Its safe on resin based materials.
- 95. RECENT ADVANCEMENTS IN RESTORATIVE MATERIALS USED IN PEDIATRIC DENTISTRY 4) SMART MATERIALS -These materials though not available commercially , retain the potential to replace currently used ones • These have been termed as ,”SMART”, as they are consistent with the newer generation of materials that support the remaining tooth structure with cavity preparation done in a conservative manner. • Some of these materials are biomimetic in nature wherein there may be properties that mimic natural tooth substance such as enamel and dentin better.
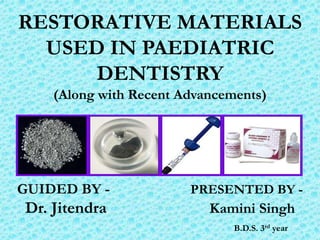
- 96. Ariston pHc restoration of tooth 24, class II, DO cavity (image in a mirror) 12 months after the filling placement. No signs of marginal leakage or fracture.
- 97. SMART MATERIALS IN DENTISTRY CAN BE CLASSIFIED AS RESTORATIVE DENTISTRY TYPES A. Passive Smart Restorative Material Glass Ionomer Cement Resin Modified Glass Ionomer Cement Compomer Dental Composite B. Active Smart Restorative Material Smart Composites Ariston pHC ACP Composites C. Prosthetic Dentistry Smart Ceramics Smart Impression Material
- 98. SMART MATERIALS IN DENTISTRY CAN BE CLASSIFIED AS D. Prosthetic Dentistry Shape Memory Alloy E. Preventive Dentistry Fluoride releasing pits and fissures sealants F. Endodontics Niti Rotary instruments
- 99. BRIEF INTRODUCTION : ACTIVE SMART MATERIALS 1) AMORPHOUS CALCIUM PHOSPHATE-ACP: it’s a vital antecedent in the biological formation of hydroxyapatite . ACP has two properties : Preventive Restorative Due to the above mentioned properties its used in dental cements and adhesives pits and fissure sealants and composites.
- 101. Mechanism Of Action : ACP
- 102. Mechanism Of Action : ACP - DEMINERALIZATION
- 103. Mechanism Of Action : ACP - REMINERALIZATION
- 104. Mechanism Of Action : ACP - BENEFITS OF ACP
- 105. BRIEF INTRODUCTION : ACTIVE SMART MATERIALS 2) Ariston Phc : Alkaline Glass Restorative Material 3) Ivoclar – Vivadent (Liechenstien), introduced a material in 1998 , Ariston pHC (pH control),which is claimed to release fluoride , hydroxide and calcium ions , when the pH in restorations of this material falls to the critical Ph. • This is said to neutralize acid and counteract the decalcification of enamel and dentin.