Sickle cell anemia- An Overview
•
184 recomendaciones•52,255 vistas

Sickle cell Anemia- Biochemical defect, inheritance, frequency, clinical manifestations, diagnosis and treatment.

Recomendados
Más contenido relacionado
La actualidad más candente
La actualidad más candente (20)
Destacado
Destacado (20)
Similar a Sickle cell anemia- An Overview
Similar a Sickle cell anemia- An Overview (20)
Más de Namrata Chhabra
Más de Namrata Chhabra (20)
Último
Último (20)
Sickle cell anemia- An Overview
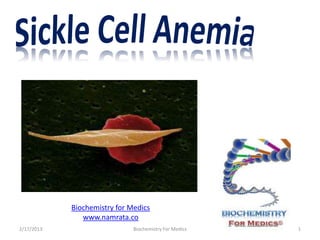
- 1. Biochemistry for Medics www.namrata.co 2/17/2013 Biochemistry For Medics 1
- 2. Normal Structure of hemoglobin Normal hemoglobin has four subunits called globins. Adult hemoglobin has two α (α 1and α 2) and two β (β 1 and β 2) globin chains. Each globin chain has an associated heme prosthetic group, which is the site of oxygen binding and release. The quaternary structure of HbA can be described as a dimer of α 1 β 1 and α 2 β 2 dimers. The αβ dimers move relative to one another during the binding and release of oxygen. 2/17/2013 Biochemistry For Medics 2
- 3. Structure of Hemoglobin All globin chains have similar primary sequences. The secondary structure of globin chains consists of approximately 75 percent α- helix. The similar primary sequence promotes a similar tertiary structure in all globins that is called the globin fold, which is compact and globular in overall conformation. 2/17/2013 Biochemistry For Medics 3
- 4. Normal Structure of hemoglobin Hemoglobin must remain soluble at high concentrations within the red blood cell to support normal oxygen binding and release properties. This is made possible by a distribution of amino acid side chains in which hydrophobic residues are sequestered in the interior core of the folded globin subunits, while hydrophilic residues dominate the water-exposed surface of the globin fold. The disk-shaped heme prosthetic group is inserted into a hydrophobic pocket formed by the globin. 2/17/2013 Biochemistry For Medics 4
- 5. Sickle cell disease- Biochemical Defect In Sickle cell disease, also called as sickle cell anemia, a single nucleotide alteration (point mutation) in the β globin gene of hemoglobin causes a change of thymine for adenine (GAG to GTG.), at the sixth codon of the ß gene. This change encodes Valine instead of Glutamic acid in the sixth position on the ß-globin molecule. The charge at this site is altered and allows for polymerization of hemoglobin under conditions of hypoxia. These properties are responsible for the profound clinical expressions of the sickling syndromes. The mutant β globin chain is designated as βs , and the resulting hemoglobin is referred as HbS. 2/17/2013 Biochemistry For Medics 5
- 6. Sickle cell disease- Biochemical Defect 2/17/2013 Biochemistry For Medics 6
- 7. Sickle cell disease- Biochemical Defect The continuous formation and destruction of sickled cells contributes to severe hemolytic anemia. These rigid cells may initiate small vessel occlusions. 2/17/2013 Biochemistry For Medics 7
- 8. Sickle cell disease- Inheritance It is a homozygous recessive disorder. It occurs in individuals who have inherited two abnormal genes (one from each parent) that code for the synthesis of β chain of the Hb molecule. Heterozygotes have on normal and one sickle cell gene. The blood cells of these individuals contain both HbS and HbA. These individuals have sickle cell trait and they usually do not show the clinical symptoms and Biochemistry For Medics 2/17/2013 can have a 8 normal life span.
- 9. Sickle cell disease-Frequency Sickle cell disease has been recognized in the malarial areas of the world. In malarial areas there is a selective advantage to the heterozygote (Hb AS), Individuals with sickle cell trait have lower levels of Plasmodium falciparum parasitemia, higher hemoglobin counts, and less severe reinfections than individuals with homozygous Hb A. 2/17/2013 Biochemistry For Medics 9
- 10. Protection against Malaria ? Sickling might protect a person from malaria by either of the following: Making it more difficult for the parasite to metabolize or to enter the sickled cell By accelerating Sickling parasitized cells are quickly removed While children with sickle cell trait Hb SA seem to have a milder form of falciparum malaria, those with homozygous Hb S have a severe form that is associated with very high mortality rate. 2/17/2013 Biochemistry For Medics 10
- 11. Protection against Malaria ? 2/17/2013 Biochemistry For Medics 11
- 12. Sickle cell disease-Frequency Sickle cell disease is most common in individuals of African descent but is seen in Hispanics, Arabians, Indian s, and whites. In the United States the incidence is 1 in 625 live births to African- Americans. 2/17/2013 Biochemistry For Medics 12
- 13. Biochemical Basis for Sickling The substitution of the nonpolar Valine for a charged glutamate forms a protrusion on the β –globin that fits in to a complementary site on the α –chain of another hemoglobin molecule in the cell. At low oxygen tension, HbS polymerizes inside the red blood cells, first forming a gel, then subsequently assembling in to a net work of fibrous polymers that stiffen and distort the cell, producing rigid misshapen erythrocytes- sickle shaped erythrocytes. 2/17/2013 Biochemistry For Medics 13
- 14. 2/17/2013 Biochemistry For Medics 14
- 15. Biochemical Basis for Sickling After recurrent episodes of sickling, membrane damage occurs and the cells are no longer capable of resuming the biconcave shape upon reoxygenation. Thus, they become irreversibly sickled cells (ISCs). From 5-50% of RBCs permanently remain in the sickled shape. The life span of an erythrocyte homozygous for HbS is approximately 20 days compared to 120 days for a normal RBC. 2/17/2013 Biochemistry For Medics 15
- 16. Factors affecting Sickling of Red blood cells The extent of Sickling depends on the factors that increase the proportion of HbS in the deoxy state. These factors include – Decreased oxygen tension as a result of high altitude or flying in nonpressurized plane, Increased pCO2 Decreased pH and Increased concentration of 2, 3 bisphosphoglycerate. 2/17/2013 Biochemistry For Medics 16
- 17. Consequences Of Sickling Reduced life span of red blood cells Sickled cells frequently block the flow of blood in the narrow capillaries. The interruption in the supply of oxygen leads to tissue anoxia, causing pain and eventually death of cells (infarction) in the vicinity of blockage. Because of the disruption of the red cell membrane, the increased adhesiveness of sickle reticulocyte, and the increased leukocyte count there is a thrombotic coagulopathy associated with sickle cell anemia that contributes to the severity of the disease. 2/17/2013 Biochemistry For Medics 17
- 18. Sickle cell disease(SCD)- Clinical Manifestations The presenting symptoms of SCD involve pain and anemia. SCD usually manifests early in childhood. For the first 6 months of life, infants are protected largely by elevated levels of Hb F The disease is associated with growth retardation, delayed sexual maturation, and being underweight Anemia is universally present. It is chronic and hemolytic in nature and usually very well tolerated. Anemia may be complicated with Megaloblastic changes secondary to folate 2/17/2013 Biochemistry For Medics 18
- 19. Sickle cell disease(SCD)- Clinical Manifestations- Cont. The spleen enlarges in the latter part of the first year of life. Pneumococcal infections are common in childhood. The most common clinical picture during adult life is vasoocclusive crisis. Many individuals with Hb S disease experience chronic low-level pain, mainly in bones and joints. The acute chest syndrome consisting of chest pain, fever, tachypnea, leukocytosis, and pulmonary infiltrates may be there Central nervous system involvement is one of the most devastating aspects of SCD.Medics 2/17/2013 Biochemistry For 19
- 20. Sickle cell disease(SCD)- Clinical Manifestations- Cont. The heart is involved due to chronic anemia and micro infarcts. Chronic hemolysis with hyperbilirubinemia is associated with the formation of bile stones. Cholelithiasis may be asymptomatic or result in acute cholecystitis, requiring surgical intervention Repeated infarction of joints, bones, and growth plates leads to aseptic necrosis Blood in the pulmonary circulation is deoxygenated, resulting in a high degree of polymer formation. Pulmonary hypertension may develop The kidneys lose concentrating capacity Leg ulcers are a chronic painful problem Chronic organ damage- Most common are lungs, kidneys, liver, skeleton and skin. 2/17/2013 Biochemistry For Medics 20
- 21. Laboratory Findings 1) A complete blood cell count usually reveals an increased reticulocytes count (5– 15%), 2) Total Leukocyte count (12,000– 20,000/mm3), upper limit of normal or greater. 3) Differential Leukocyte count- normal (or predominance of neutrophils 4) Mean corpuscular volume (MCV) normal (unless thalassemic hemoglobin is present), 5) Hb- mild to moderate anemia (5–9g/dL), 6) Platelet count- normal to increased, 2/17/2013 Biochemistry For Medics 21
- 22. Laboratory Findings-Contd. 7) Blood smear- A diagnosis of sickle cell disease can be suspected by examination of the peripheral blood film and that shows the presence of target cells, poikilocytes, hypochromasia, sickle red cells, nucleated RBCs, and Howell-Jolly bodies 2/17/2013 Biochemistry For Medics 22
- 23. Laboratory Findings-Contd. 8) Sickle solubility test-A mixture of hemoglobin S (Hb S) in a reducing solution (such as sodium dithionite) gives a turbid appearance, whereas normal Hb gives a clear solution. 9)Hemoglobin electrophoresis-The substitution of the nonpolar Valine for the charged Glutamic acid results in decreased mobility of the HbS in the electric field as compared to HbA. This altered mobility is due to the presence of less negative charge on the two β –globin chains 10) HPLC-The diagnosis is confirmed by high- pressure liquid chromatography (HPLC). 2/17/2013 Biochemistry For Medics 23
- 24. Laboratory Findings-Contd. 10) Bone marrow is markedly hyper plastic with erythroid predominance. 11) Radiological studies may reveal characteristic bony findings of sickle cell disease in the vertebral bodies, mild expansion of the marrow cavities, osteoporosis, and possibly sclerosis of the long bones and femoral heads. 12) Liver function tests, as well as BUN, creatinine, and serum electrolytes are also required to be performed. 2/17/2013 Biochemistry For Medics 24
- 25. Treatment Treatment strategies include the following 7 goals: (1) management of vasoocclusive crisis, (2) management of chronic pain syndromes, (3) management of the chronic hemolytic anemia, (4) prevention and treatment of infections, (5) management of the complications and the various organ damage syndromes associated with the disease, (6) prevention of stroke, and (7) detection and treatment of pulmonary hypertension. 2/17/2013 Biochemistry For Medics 25
- 26. Treatment (Contd.) Vasoocclusive crisis is treated with vigorous hydration and analgesics. Pain control is best achieved by the administration of opioids. Prevention of infection improves chances of survival in SCD. Allogeneic bone marrow transplantation (BMT) can cure the disease, but it is difficult to decide which patients should be offered BMT. Therapy with hydroxyurea- Hydroxyurea increases the production of Hb F, which retards gelation and sickling. Blood transfusion is indicated only in specific situations Surgical care is limitedBiochemistry For Medics 2/17/2013 to treating disease complications. 26
- 27. Prevention of sickle cell disease Screen for Hb S at birth. This method of case finding allows institution of early treatment and control. Prenatal diagnosis is also available. The laboratory procedures employed in prenatal testing are sensitive and rapid. Prenatal testing must be accompanied with genetic and psychological counseling. 2/17/2013 Biochemistry For Medics 27
- 28. Prognosis Because this is a lifelong disease, prognosis is guarded. The goal is to achieve a normal life span with minimal morbidity. As therapy improves, the prognosis also improves 2/17/2013 Biochemistry For Medics 28
- 29. Sickle cell trait About 8% of African Americans and about 30% of Nigerians are heterozygous for sickle cell trait. HbS heterozygotes have minimal clinical problems Overall life expectancy is similar to normal individuals Individuals with sickle cell trait may develop sickle cell crisis if they become severely hypoxic May have recurrent episodes of painless hematuria due to impaired ability to form concentrated urine. These individuals are not placed at high risk. 2/17/2013 Biochemistry For Medics 29
- 30. Sickle beta Thalassemia Commonly encountered from Mediterranean countries as well as from central Africa Patients have congenital hemolytic anemia of varying severity, accompanied by splenomegaly in 70 % of cases. Sickle β0 Thalassemia have vaso- occlusive manifestations comparable to homozygous SS disease. Sickle β+ Thalassemia have less severe anemia, fewer pain crisis and less organ damage 2/17/2013 Biochemistry For Medics 30
- 31. Sickle C disease Hb electrophoresis reveals 50% HbS and 50% Hb C One of the beta chain gene is defective for Hb S and the other is defective for Hb C( The 6th position in beta chain is replaced by Lysine in place of Glutamic acid There is increased tendency for SC cells to sickle cell as compared to sickle cell trait Occasional painful crisis or organ infarcts High rate of complications during pregnancy 2/17/2013 Biochemistry For Medics 31
- 32. 2/17/2013 Biochemistry For Medics 32