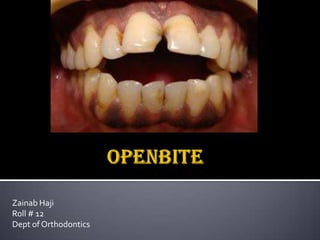
Openbite
•Descargar como PPTX, PDF•
51 recomendaciones•10,411 vistas

This document discusses open bite, including its definition, classification, causes, and management. Open bite is classified as anterior, posterior, dental/simple, or skeletal/complex. Causes include hereditary factors, environmental factors like mouth breathing, thumb sucking, and trauma. Management depends on the patient's age and involves things like habit control, growth modulation, functional appliances with bite blocks, and sometimes orthognathic surgery. High pull headgear is discussed as a way to control vertical growth.

Recomendados
Más contenido relacionado
La actualidad más candente
La actualidad más candente (20)
Destacado
Destacado (20)
Similar a Openbite
Similar a Openbite (20)
Último
Último (20)
Openbite
- 1. Zainab Haji Roll # 12 Dept of Orthodontics
- 3. Malocclusion in vertical plane. A deviation in the vertical relationship of the maxillary and mandibular dental arches characterized by a definite lack of contact between opposing segments of teeth.” (Daniel Subtelny, 1964). “Localized absence of occlusion while the remaining teeth are in occlusion” (Moyer’s).
- 4. According to location: Anterior OB. Posterior OB. According to cause: Dental or simple OB. Skeletal or complex OB.
- 5. Anterior OB: “Absence of contact between the maxillary and mandibular incisors at centric relation (Worms 1971).” Absence of vertical overlap of incisors. Posterior OB: “Lack of contact between the posterior teeth when the teeth are in centric occlusion.” Dental (Simple) OB: When the basal skeleton is normal and the open bite is confined to the teeth and alveolar processes. Skeletal OB: Results from skeletal dysplasia, so severe that the alveolar processes cannot cope to maintain occlusal stops.
- 6. Dental openbite 1) Heredity Secondary to class III malocclussion.
- 8. change in mode of respiration ,lowers the mandible and the tongue supra-eruption of posterior teeth downward and backward rotation of mandible increased facial (ant) height. Factors that cause mouth breathing Enlarged adenoids or tonsils. naso-pharyngeal deformities. Enlarged turbinates. Allergic rhinitis, nasal polyps, etc.
- 9. Normal upto 4-5 years - Inadequate development of the anterior alveolar process. - Incomplete eruption of the incisor teeth Accommodation of thumb Lowered positioning of mandible Alteration in vertical equilibrium Excessive eruption of posterior teeth
- 10. defined as placement of the tongue tip forward between the incisors during swallowing”. Transitional Displaced incisors Trauma Failure of eruption
- 11. Excessive tipping of the buccal segments. Elongation of lingual cusp Premature contacts Open Bite Distalization: Expansion treatment: as a consequence of orthodontic therapy Distalization of 6 l 6 Distal tipping Elongation of mesial cusps OpenBite (Great concern in vertical grower)
- 12. Jaw rotation during growth. The palatal plane rotates downward posteriorly. Mandible shows backward rotation with an increased in MPA
- 13. Diagnosis: Extraoral Intraoral Cephalogram Treatment: Deciduous dentition Mixed dentiton: -habit control -growth modulation
- 15. Gaining confidence of the patient Education to the patient Reminder Therapy Reward Therapy Restriction Therapy: Appliance : Vestibular screen. Tongue crib
- 17. Only if associated with long face syndrome. I. HIGH PULL HEADGEAR TO THE MOLARS: Maintains the vertical position of the maxilla. Inhibits eruption of the maxillary posterior teeth.. Duration : 14 hours, putting the headgear right after dinner and wearing it until next morning. Force : 350 – 450 gm / side (12 – 16 ounces). Drawback : It does not control the eruption of other teeth. II. HIGH PULL HEADGEAR TO A MAXILLARY SPLINT: acrylic splint to which a face bow and HP headgear is attached. appears to have substantial maxillary skeletal and dental effect with good vertical control. Unfortunately, this appliance allows mandibular posterior teeth to erupt freely, and if this occurs, there may be neither redirection of growth for favorable upward and forward mandibular rotation.
- 19. III. FUNCTIONAL APPLIANCES WITH BITE BLOCKS : The retraction force of headgear is replaced by the somewhat lesser “headgear effect” of the functional appliance with posterior bite block Purpose: To inhibit eruption of posterior teeth and vertical descent of the maxilla. When the mandibular is held in this position by the appliance, the stretch of soft tissues (including but not limited to the muscles) exerts a vertical intrusive force in the posterior teeth. In children with AOB the anterior teeth are allowed to erupt, which reduces the OB. As this allows the mandible to position forward, horizontal growth of mandible can be encouraged.
- 20. IV. HP HEADGEAR TO A FUNCTIONAL APPLIANCE WITH BITE BLOCKS: Most effective approach in OB classII. HP headgear: Increases the control of maxillary growth. Allows the force to be delivered to the whole maxilla Improves retention appliance. Produces force direction near the estimated center of resistance of the maxilla. The headgear tube – is incorporated in premolar regions. Force = 250 – 500 /side
- 22. High pull headgear to a maxillary molars High pull headgear to maxillary splint Functional appliance with bite blocks High pull headgear to a functional appliance with bite blocks
- 23. Surgical Orthodontics is a term that refers to surgical procedures carried out as an adjunct to or in conjunction with orthodontic treatment. Orthognathic surgery is a surgical procedure carried out along with orthodontic therapy to correct dento-facial deformities or severe orofacial disproportion involving the maxilla, the mandible or both in combination.
- 24. I. MAXILLARY SURGERY: LeeForte I down fracture of maxilla, or. Segmental maxillary osteotomy, and Combination. II. MANDIBULAR SURGERY: 1. BSSO (BILATERAL SAGITTAL SPLIT OSTEOTOMY) 2. INVERTED ‘L’ OSTEOTOMY OF RAMUS WITH RIF: III. SUPERIOR REPOSITIONING OF THE CHIN BY A MANDIBULAR LOWER BORDER OSTEOTOMY
- 26. (AOB NOT RELATED TO LONG FACE): There are 2 major possibilities: 1-Deficient eruption of maxillary incisor: *LeForte 1 osteotomy with or without anterior and posterior components. *Maxillary anterior segmental osteotomy.
- 27. 2-AOB due to deficient eruption of mandibular incisors +excessive eruption of posterior teeth: *anterior subapical osteotomy *total submandibular sub-apical osteotomy
- 28. Worms F.W, Meskin L.H, Isaacson R.J., Open bite. AJO 1971; 59:589-95. Klein: The Thumb sucking habit: Meaningful or Empty. AJO 1971. Bishara. Clinical Biomechanics, Seminar Orthodontics; March 2001, Vol 7. No.1. Carano A., Machita W. A rapid molar intruder for `Noncompliances treatment’ . JCO 2002 March; 8: 137-142. Iscan M.N. Akkaya Sevil and Koralp E. The effects of the spring - loaded posterior bite-block on the maxillo-facial morphology. Eur J Orthod 1992; 14:54-60.
Notas del editor
- Adenoid Facies: A special facial type has become associated with individuals who have a long history of mouth breathing. It is characterized by -Open mouth posture.A nose that appears to be flattened.Nostrils that are small and poorly developed.A short upper lip.A voluminous + pouting lower lip.A vacant facial expression as a result of hanging posture of the lower
- Interference with normal eruption of incisors due to an interposed thumb or fingers.Excessive eruption of posterior teeth.
- Gaining confidence of the patient:Should be gentle, caring, calm, concerned + friendly.Education to the patient :Adult approach:a. Explain consequences.b. Explain result of treatment.c. Use casts + photographs.Often enough to terminate habit.More effective in older children.Reminder Therapy:Meant for the children who want to quit the habit but need help:Securing an adhesive bandage with waterproof tape on the finger that is sucked.Anterior portion of quad helix appliance.4. Reward Therapy:Small tangible reward daily for not engaging in the habit.Large rewards for complete cessation of habit.5. Restriction Therapy:Indicated for these children who want to quit the habit but when all above approaches have failed.An elastic bandage to prevent the arm from being flexed should be used.Should be prescribed for night only for 6-8 weeks.The child should be explained that this is not a punishment.6. Appliance Therapy:Includes:Vestibular screen.Tongue crib-Removable.Fixed. Fixed is preferred because of patient compliance.