

Recomendados
Más contenido relacionado
La actualidad más candente
La actualidad más candente (20)
Similar a Gonorrhea
Similar a Gonorrhea (20)
Último
Último (20)
Gonorrhea
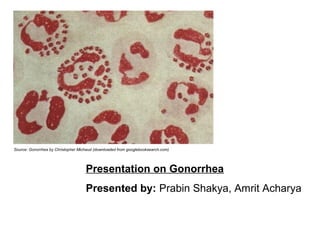
- 1. Source: Gonorrhea by Christopher Michaud (downloaded from googlebooksearch.com) Presentation on Gonorrhea Presented by: Prabin Shakya, Amrit Acharya
- 2. Gonorrhea: Gonorrhea is one of the common and highly contagious sexually transmitted diseases caused by Neisseria gonorrhoeae which differ in males and females in course, severity and ease of recognition and can lead to different systemic complication if left untreated.
- 3. Historical Background • Ancient disease known in human civilization • First scientific observation done by Hippocrates, he dissected the infected urethra • The name gonorrhea use first time by Greek doctor Galen in 130 BC • Gono means seed and rhoia means flow • He mistakenly thought that the abnormal discharge was semen • Slang named as “Clap”, “Drip”
- 4. Distribution • World wide in distribution. • Affects both sexes. • Most prevalent in lower socio economic condition and poor hygiene practices. • it one of the classical sexually transmitted disease. • In most of the developed countries the incidence have decreased during the past two decades • Resistance to penicillin and tetracycline is widespread. • WHO collaborating centers for development of gonococcal antimicrobial surveillance program
- 5. Epidemiological features 1). Agent factors a). Agent b). Reservoir of infection c). Sources of infection d). Period of Communicability 2). Host factors a). Age b). Sex c). High risk groups d) susceptibility and resistance
- 6. Mode of transmission 1). Sexual transmission 2). Congenital or Vertical transmission 3). Transmission from fomites
- 7. Incubation Period Usually 3-8 days with a range of 1-14 days in men and within 10 days for women
- 8. Pathogenesis • The common method of transmission is by sexual intercourse. • The risk of men contracting infection varies with the number of exposures with infectious female. It has been estimated 19% for one exposures and rising to 57% for >= to 4 exposures. • The risk of infection to female from the infected male have no been thoroughly investigated but it have been found in those who have been exposed on more than one occasion have infection rates of between 92% and 59%. • Similarly, it has also been found that males were probably at greatest risk from menstruating females. • From experimental research it has been found that 103 cfu are required reliably to infect male urethra where as the number of gonococci found in vagina seems to be highly variable. However, 4.0 x 102 to 1.8 x 107 cfu have been estimated to infect female.
- 9. Pathogenesis….contd • Once transferred, the gonococci rapidly become attached to mucosal cells. • Micturition after intercourse do not remove them. • Due to the presence of pili the organisms show marked ability to adhere to the human cells, especially to the squamocolumnar cells of uterine cervix. It have been found that pili present in the infectious gonococci can overcome the electrostatic forces of repulsions between the negatively charged bacterial surface and the sialic acid on the surface of host cells and bind the organisms loosely to the cell surface. • When organisms are loosely attached to the host cells, many other factors come into play. These include non specific mechanisms such as the mutual attraction of hydrophobic moieties on cell and bacterial surfaces, and more specfic mechanisms. • Gonococcal outer membrane protein II occurs in the cell membrane and helps in this process. The presence and absence of which produces different types of colonies and virulence. A single strain of gonococcus can produce many different variants of proteins and also none at all, this variation helps the organisms to spread to different tissues as it colonizes.
- 10. Pathogenesis….contd • The organisms produces endotoxin, damage some cells in the local environment, where as in other cells the organisms enter. • The organisms become attached to the microvilli of the cell membrane during the insertion of the organisms initially the major outer membrane protein (protein I) is first inserted in cell membrane. • The organisms enter the cells as the result of phagocytic process (endocytosis) and multiply therein. • This causes cell death and the organisms enters the subepithelial tissue. • In the urethral and cervical pus phagocytosed gonococci are found. • The gonococci are found inside the phagosomes, degranulated, with dead cells in the vacuoles. • However in some polymorphs, large number of viable organisms are found which damage the polymorphs and are called as the “infectious units”. These are protected from host attack and can invade epithelial cells.
- 11. Pathogenesis….contd • In female spread to the fallopian tubes occurs mainly at the time of menstruation. • Certain strains of gonococci seem to have particular abilities to spread to distant sites, so producing the DGI (Disseminated gonorrheal infection ) syndromes. • They show the resistance to the killing action of complement.
- 12. Clinical manifestation Gonorrheal infection may be symptomatic or asymptomatic. When symptomatic men usually have: -Dysuria -Urinary frequency -Purulent urethral discharge Women may have: -Abnormal vaginal discharge -Dysuria, and/or vaginal bleeding between menstrual periods -Diffuse pelvic inflammatory disease (PID) may cause fever along with pain and tenderness of the pelvic organs and lower abdomen
- 13. Clinical manifestation….contd. Other sign and symptoms: • Pharyngeal infection and anorectal infection in men and women may be asymptomatic • Symptoms of anorectal infection may include discharge, anal itching, soreness, bleeding, or painful bowel movements • The symptom of pharyngeal infection is a sore throat, but pharyngeal infection is usually asymptomatic
- 14. Clinical manifestation….contd. Complication The major complications of acute gonorrhea in women are: • 10%-20% risk of developing PID • subsequent risk for acute and chronic complications such as chronic pelvic pain, infertility and increased risk of ectopic pregnancy The major complications in men are: • epididymitis • urethral stricture • infertility, temporary or permanent The major complications in neonates are: • ophthalmia neonatorum • blindness • scalp abscess (at site of fetal monitor) • rhinitis • pneumonia • anorectal infection • joint infection
- 15. Clinical manifestation….contd. Additional major complications in any untreated individual include: • arthritis • dermatitis • endocarditis • meningitis • septicemia
- 16. Characters of causative organisms The causative organisms of gonorrhea is Neisseria gonorrhoeae, which is Gram- negative, aerobic, non-motile, oxidase positive diplococci which is strict parasites and human beings are the only known reservoirs of these pathogens. Taxonomy It belong to the family Neisseriaceae along with Moraxella, Acinetobacter and Kingella. Morphological Gram-negative diplococci, oval in shape, 0.6-1 micrometer in diameter and occur characteristically in pairs with adjacent sides concave i.e., bean shaped or kidney shaped. Possess pili. Cultural -fastidious -Culture in enriched and selective medium such as Thayer-Martin Medium and New York City Medium supplemented with antibiotics.
- 17. Characters of……contd After 24 hrs of incubation gives small, grey and glistening colonies appear which become larger at 48 hrs incubation. Five different types of colonies produced which are T1, T2, T3, T4, and T5 only T1 and T2 are virulent. Biochemical Oxidase positive and ferments only glucose with acid only Antigenic properties 1). Capsules 2). Pili 3). Proteins a). Por (Protein I) b). Opa (Protein II) c). Protein III 4). Lipopolysaccharides 5). Other protiens
- 18. Laboratory diagnosis Specimen collection: specimen are collected from genital sources, rectum in case of homosexuals, throat specimen as appropriate as well as for other extragenital infection such as oropharynx, skin lesion, inflamed joints, blood, and pelvic inflammatory disease The routine laboratory diagnosis of gonorrhea proceeds as follows: 1) Gram stain microscopy. 2) Culture on enriched selective medium. 3) Examine colonies for suspected colonies and perform oxidase test. 4) Perform Rapid carbohydrate utilization test (RCUT) along with beta lactamase prodution. 5) Slide agglutination test with commercially available monoclonal antibody kit. 6) Conduct antimicrobial susceptibility test 7) In suspected DGI perform blood cultures in Biphasic medium and incubate in a CO2 incubator with a cotton wool plug. And perform immunofluorescence staining.
- 19. Treatment Primarily large dose of intramuscular penicillin or oral ampicillin or doxycycline is used as the treatment therapy for gonorrhea but due to the penicillin resistance other alternatives such as cefuroxime, cefotaxime. Erythromycin, spectinomycin, or ciprofloxacin are used.
- 20. Prevention and control Sexually transmitted diseases can be prevented by abstinence or condom use. Ophthalmia neonatorum may be prevented by third-trimester treatment of cervically infected mothers and their sexual partners. Ocular prophylaxis of all newborns with ointments of 1 percent tetracycline or 0.5 percent erythromycin is recommended. Thus the control of gonorrhea can be listed as: • Rapid diagnosis • Use of effective antibiotics • Tracing, examination and treatment of contacts
- 21. References Books and Reports • Control of communicable diseases manual, Nepal government, Ministry of Health, department of health services, epidemiology and disease control division. • Greenwood.D, Peutherer.J, Slack.R (2006); Medical Microbiology; 16th edition; Longman Group Ltd. • Zuckerman AJ,Banatvala JE, Pattison JR, Griffiths P & Schoub B(2004) Topley & Wilson’s Principles of Bacriology,Virology, Immunology Volume IV; John Wiley& Sons Ltd.:England. • Collee JG et al (editors) (2007); Mackie and McCartney Practical Medical Microbiology, Elsevier, India. • Chakraborty P. (2004), A text book of Microbiology • Bailey and Scott’s Diagnostic Microbiology • Greenwood Medical Microbiology