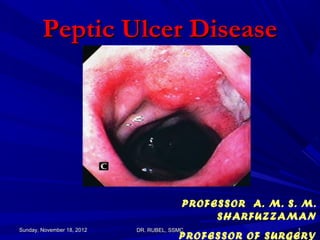
1. Peptic Ulcer Disease
PROFESSOR A. M. S. M.
SHARFUZZAMAN
Sunday, November 18, 2012 DR. RUBEL, SSMC 1
PROFESSOR OF SURGERY
2. Learning Objectives
To be able to decide on the most appropriate
techniques to use in the investigation of patients with
complaints relating to the stomach and duodenum.
To understand the critical importance of gastritis and
Helicobacter pylori in upper gastrointestinal disease.
To be able to investigate and treat peptic ulcer
disease and its complications.
Sunday, November 18, 2012 DR. RUBEL, SSMC 2
3. Definition
Peptic Ulcer Disease is defined as an ulcer
occurring in a region that touches gastric acid
and pepsin and usually refers to gastric ulcer or
duodenal ulcer.
Sites:
Duodenum, ……(80%)
Stomach ……….(19%)
Duodenum and Stomach……(4%)
G-E junction
Gastro-jejunostomy site (1%)
Meckel’s diverticulum
Sunday, November 18, 2012 DR. RUBEL, SSMC 3
4. Erosion :
a superficial lesion caused by
denudation of the surface epithelium
Ulcer :
a mucosal defect extending into the
muscularis mucosa
Sunday, November 18, 2012 DR. RUBEL, SSMC 4
5. Epidemiology of peptic ulceration
Frequency
United States:
One-year point prevalence is 1.8%. Lifetime prevalence is approximately 10%.
PUD affects approximately 4.5 million people annually.
Internationally:
The prevalence of H pylori infection in developing countries is as high as 50-
100%. The prevalence of PUD is increasing in developing countries.
Sex
There is a 3 to 1 male to female ratio for GU and 4 to 1 for DU. Prevalence has
shifted from predominance in males to similar occurrences for both sexes.
Lifetime prevalence is approximately 11-14% for men and 8-11% for women.
Age
The peak age for DU is increasing(25-50 years worldwide but higher in
developed countries), GU occurs in older age groups>50
Sunday, November 18, 2012 DR. RUBEL, SSMC 5
6. Mucosal defences against peptic ulceration
EXTRAMUCOSAL
Mucous cap; a hydrophobic gel layer secreted by the mucus cells,
Buffer layer; hydrogen carbonate is trapped in the mucous cap buffering
the acid,
Bicarbonate secretion: leads to a pH gradient from 2 in the lumen to 7 on
the epithelial surface.
MUCOSAL
Luminal cells resistance to acid.
Mucosal integrity(prostaglandin helps to maintain this so is reduced
when taking NSAIDs; other growth factors also help and are inhibited by
alcohol)
Tight cell junctions.
MICROVASCULAR
The microcirculation neutralises acid and removes toxic substances;
smoking-related microvascular disease reduces this blood flow.
Sunday, November 18, 2012 DR. RUBEL, SSMC 6
7. Pathogenesis;
Normal
Increased Attack
Hyperacidity
Weak defense
Helicobacter pylori
Stress, drugs,
smoking
Sunday, November 18, 2012 DR. RUBEL, SSMC 7
8. Pathogenesis;
Damaging forces: - Acid
- Pepsin
Defensive forces:*Surface mucous, *Bicarbonate ion in mucous, *Mucosal
blood Flow, *Apical surface membrane transport, *Epithelial
regeneration, *Prostaglandins
Sunday, November 18, 2012 DR. RUBEL, SSMC 8
9. Etiology;
H.Pylori
Urease – Ammonia stimulates gastrin release, increases
acid secretion
Protease – breaks glycoprotein of mucous
Lipopolysaccharide – attracts neutrophils
Hyperacidity
Zollinger – Ellison Syndrome
multiple endocrine neoplasia (MEN-I)
Antral G cell hyperplasia
Systemic mastocytosis
Basophilic leukemias
Drugs No effect of
NSAIDS
Corticosteroids
genetics and
Systemic stresses spicy foods
Cigarette smoking, Alcohol
Rapid gastric emptying
Personality and stress
Sunday, November 18, 2012 DR. RUBEL, SSMC 9
10. Helicobacter pylori:
Most common infection in the world (20%)
10% of men, 4% women develop PUD
Positive in 70-100% of PUD patients.
H.pylori related disorders:
Chronic gastritis – 90%
Peptic ulcer disease – 95-100%
Gastric carcinoma – 70%
Gastric lymphoma
Reflux Oesophagitis.
Non ulcer dyspepsia
Sunday, November 18, 2012 DR. RUBEL, SSMC 10
11. H. pylori – silver stain
Sunday, November 18, 2012 DR. RUBEL, SSMC 11
12. H. pylori – giemsa stain
Sunday, November 18, 2012 DR. RUBEL, SSMC 12
13. H. pylori – H & E stain
Sunday, November 18, 2012 DR. RUBEL, SSMC 13
14. H. Pylori
S-shaped gram
negative rod, flagella
Produces urease,
protease, cytotoxin
Alters acid secretory
function
Binds to mucosal
blood group antigen
Colonization rate
increases with age:
up to 50% in persons
>50 years
Sunday, November 18, 2012 DR. RUBEL, SSMC 14
15. Risk factors for H.Pylori infection;
Birth in a developing country
Low socioeconomic status
Crowded living conditions
Large families
Unsanitary living conditions
Unclean food or water
Presence of infants in the home
Exposure to gastric contents of infected individuals
Sunday, November 18, 2012 DR. RUBEL, SSMC 15
16. Pathogenetic qualities of H.pylori;
Adheres to gastric epithelium
Lives within mucous gel layer overlying gastric epithelium
Penetrates intercellular junctions
Invades gastric glands and canaliculi of parietal cells
Secretes urease to produce ammonia, which protects it from
gastric acid
Produces cytotoxins that may play role in pathogenicity
Induces epithelial cytolysis and disrupts intercellular
junctions
Increases permeability of mucous layer to hydrogen ions
and pepsin
Enables gastric acid and pepsin to create ulcer craters
Evades host immune defenses
Damages tissue.
Sunday, November 18, 2012 DR. RUBEL, SSMC 16
17. Peptic Ulcer
Size – variable; 0.3 – 4 cm in
diameter
Shape - round to oval
Sharply demarcated, clean-cut,
punched-out area with clean base
Margins are usually level with
surrounding mucosa or slightly
elevated due to edema; the mucosa
is undermined at the edges
Radiating mucosal rugae
80% are solitary, 80% occur in the
duodenum, of which 90% in the
first part of the duodenum on the
anterior wall’ within a few
centimeter of the pyloric ring.
19% occur in the stomach(usually
at the lesser curvature at the border
of the body and antrum.
Sunday, November 18, 2012 DR. RUBEL, SSMC 17
25. Microscopy:
Overhanging gastric
mucosal margins (A)
A
B Necrotic fibrinoid
C, D debris (B)
Acute inflammatory
infiltrate (C)
Granulation tissue
(D)
E
Fibrotic scarred
base (E)
Sunday, November 18, 2012 DR. RUBEL, SSMC 25
26. Ulcer Base
Superficial thin layer of
necrotic fibrinoid debris
Zone of inflammatory
infiltrate with neutrophils
Zone of granulation
tissue with dilated blood
vessels and lymphocytes
Zone of fibrous scarring
Sunday, November 18, 2012 DR. RUBEL, SSMC 26
27. H. Pylori - Lab Studies
HP fecal antigen test
Monoclonal antibody immunochromatography of
stool samples.
Very specific (98%) and sensitive (94%).
13
Carbon-urea breath test
HP serology – IgG
Biopsy/Histopathology
CLO test,
Culture
Sunday, November 18, 2012 DR. RUBEL, SSMC 27
33. Typical radiographic features of duodenal ulcer. This
duodenal bulb ulcer is associated with marked edema,
resulting in the appearance of radiating folds to the ulcer
crater. The bulb is also distorted secondary to previously
existing ulceration
Sunday, November 18, 2012 DR. RUBEL, SSMC 33
34. Typical radiographic features of
a benign gastric ulcer;
A large well-
circumscribed
ulcer is seen
on the
angularis
Sunday, November 18, 2012 DR. RUBEL, SSMC 34
39. Typical endoscopic appearance of a benign gastric ulcer. The ulcer is
on the angularis, the most common location for a gastric ulcer, and is
well circumscribed without any associated mass effect. The
surrounding mucosa is mildly erythematous and without nodularity.
Sunday, November 18, 2012 DR. RUBEL, SSMC 39
41. Erosions in the duodenal bulb and a
posterior duodenal ulcer
Sunday, November 18, 2012 DR. RUBEL, SSMC 41
42. Clinical presentation of PUD
Symptoms:
Abdominal pain
located in the epigastric area
burning in quality
occurred on an empty stomach 2 to 4 hours after meals
and/or at night (nocturnal pain);
relieved by antacids and/or meals
tend to wax and wane over months
“acid dyspepsia”
Sunday, November 18, 2012 DR. RUBEL, SSMC 42
43. Abdominal pain(cont.)
the majority of patients (approximately 70%)
with epigastric distress (“dyspepsia”) do not
have evidence of active ulcer disease;
conversely up to 40% of patients with an
active ulcer crater deny abdominal pain;
patients can present with an ulcer-related
complication, particularly hemorrhage,
without antecedent symptoms
Sunday, November 18, 2012 DR. RUBEL, SSMC 43
44. Abdominal pain(cont.)
Despite being both insensitive and
non-specific, the symptom of
epigastric abdominal pain, particularly
burning after meals and at night and
relieved with food or antacid,
suggests the possibility of ulcer
disease.
Sunday, November 18, 2012 DR. RUBEL, SSMC 44
45. Other symptoms
gastro esophageal reflux including upright and supine
reflux and non-cardiac chest pain
symptoms of indigestion occurring with or shortly after
eating and characterized by epigastric fullness and
discomfort belching bloating nausea early satiety and
specific food intolerances.
Sunday, November 18, 2012 DR. RUBEL, SSMC 45
46. Signs;
Physical examination is of limited value
in patients with uncomplicated ulcer.
For epigastric tenderness on deep
palpation, the sensitivity and specificity
are all approximately 50% or less.
Furthermore, many patients with non-
ulcer diseases also have epigastric
tenderness on physical examination.
Sunday, November 18, 2012 DR. RUBEL, SSMC 46
47. Signs(cont.)
In patients with free perforation or ulcer
penetration into the pancreas, findings of
peritonitis are usually present.
In patients with gastric retention who have been
fasting for a few hours, a succussion splash
(produced by auscultating the abdomen while
rocking the patient back and forth), suggests
retained gastric contents.
Sunday, November 18, 2012 DR. RUBEL, SSMC 47
48. Complications:
Hemorrhage
The most common complication of ulcer disease (in approximately
15% of patients) manifest as haematemesis and melena.
Perforation
Duodenal ulcers: perforate anteriorly
Gastric ulcers: perforate along the anterior wall of the lesser
curvature of the stomach.
Penetration
Mainly to posterior structure as pancreas.
Scarring and stenosis
Stomach: tea-pot deformity, hour-glass contracture.
Duodenum: pyloric stenosis as GOO.
Sunday, November 18, 2012 DR. RUBEL, SSMC 48
49. Hemorrhage
The most common complication of ulcer disease (in
approximately 15% of patients) manifest as
haematemesis and melena. Bleeding: Upper
gastrointestinal (UGI) bleeding secondary to peptic
ulcer is a common medical condition that results in
high patient morbidity UGI bleeding commonly
presents with hematemesis (vomiting of blood or
coffee-ground like material) and/or melena (black,
tarry stools).
Sunday, November 18, 2012 DR. RUBEL, SSMC 49
51. Perforated peptic ulcer.
Duodenal, antral, and gastric body ulcers account for 60, 20 and
20percent of perforations due to peptic ulcer, respectively . One-third
to one-half of perforated ulcers are associated with NSAID use; these
usually occur in elderly patients
Sunday, November 18, 2012 DR. RUBEL, SSMC 51
52. Penetration
Is similar pathologically to perforation,
except that the ulcer crater burrows through
the entire wall of the intestine, and instead
of leaking digestive contents into the
peritoneal cavity, the crater bores into an
adjacent organ.
Gastric ulcers most commonly penetrate
into the left lobe of the liver, while duodenal
ulcers penetrate posteriorly into the adjacent
pancreas, sometimes leading to pancreatitis.
Rarely, gastric ulcers may penetrate into the
colon, resulting in a gastrocolic fistula
Sunday, November 18, 2012 DR. RUBEL, SSMC 52
53. Gastric outlet obstruction (gastric retention
or pyloric stenosis);
Gastric outlet obstruction is the least frequent ulcer
complication. Most cases are associated with duodenal
or pyloric channel ulceration, with gastric ulceration
accounting for only 5 percent of cases.
functional impairment of antral motility due to the
effects of acute inflammation and edema;
mechanical obstruction due to scarring near the
gastroduodenal junction;
manifest as gastroesophageal reflux, early satiety,
weight loss, abdominal pain, and vomiting;
As the degree of retention increases, the quantity of
vomitus also increases, often containing food ingested
12 or more hours previously.
Sunday, November 18, 2012 DR. RUBEL, SSMC 53
54. Barium upper gastrointestinal study
demonstrates the size of the stomach.
Pyloric
stenosis
Sunday, November 18, 2012 DR. RUBEL, SSMC 54
55. Endoscopy demonstrates the pyloric
obstruction with an active ulcer crater seen
in the pyloric channel.
Sunday, November 18, 2012 DR. RUBEL, SSMC 55
59. TREATMENT;
Medical treatment
Given the current understanding of the pathogenesis of PUD,
most patients with PUD are treated successfully with cure of H
pylori infection and/or avoidance of NSAIDs, along with the
appropriate use of antisecretory therapy.
A number of treatment options exist for patients presenting
with symptoms suggestive of PUD or ulcerlike dyspepsia,
including empiric antisecretory therapy, empiric triple therapy
for H pylori infection, endoscopy followed by appropriate
therapy based on findings, and H pylori serology followed by
triple therapy for patients who are infected. Breath testing for
active H pylori infection may be used.
Sunday, November 18, 2012 DR. RUBEL, SSMC 59
60. Medical treatment(cont.)
Computer models have suggested that obtaining H pylori
serology followed by triple therapy for patients who are
infected is the most cost-effective approach; however, no
direct evidence from clinical trials provides confirmation.
Perform endoscopy early in patients older than 45-50 years
and in patients with associated so-called alarm symptoms,
such as dysphagia, recurrent vomiting, weight loss, or
bleeding.
Sunday, November 18, 2012 DR. RUBEL, SSMC 60
61. Surgical Care
With the success of medical therapy, surgery has a very limited role in the
management of PUD.
Potential indications for surgery include refractory disease. Complications of
PUD include the following:
Refractory, symptomatic peptic ulcers, though rare with the cure of H
pylori infection and the appropriate use of antisecretory therapy, are a
potential complication of PUD.
Perforation usually is managed emergently with surgical repair.
However, this is not mandatory for all patients.
Obstruction can complicate PUD, particularly if PUD is refractory to
aggressive antisecretory therapy, H pylori eradication, or avoidance of
NSAIDs. Obstruction may persist or recur despite endoscopic balloon
dilation.
Sunday, November 18, 2012 DR. RUBEL, SSMC 61
62. Surgical Care(cont.)
Penetration, particularly if not walled off or if a gastrocolic fistula
develops, is a potential complication of PUD.
Bleeding can complicate PUD, particularly in patients with massive
hemorrhage and hemodynamic instability, recurrent bleeding on
medical therapy, and failure of therapeutic endoscopy to control
bleeding.
The appropriate surgical procedure depends on the location and nature of
the ulcer.
Many authorities recommend simple oversewing of the ulcer with treatment
of the underlying H pylori infection or cessation of NSAIDs for bleeding
PUD.
Additional surgical options for refractory or complicated PUD include
vagotomy and pyloroplasty, vagotomy and antrectomy with gastroduodenal
reconstruction (Billroth I) or gastrojejunal reconstruction (Billroth II), or a
highly selective vagotomy.
Sunday, November 18, 2012 DR. RUBEL, SSMC 62
63. Diet
No special diet is required.
Medication
Treat all patients with peptic ulcers and associated H pylori infection with proton
pump inhibitor (PPI)-based triple therapy, which results in a cure rate of
infection and healing in approximately 85-90% of cases. Ulcers can relapse in
the absence of successful H pylori eradication.
Dual therapies, which are alternative regimens for treating H pylori infection,
are usually not recommended as first-line therapy because of a variable cure
rate that is significantly less than the cure rate achieved with triple therapy.
Active ulcers associated with NSAID use are treated with an appropriate course
of PPI therapy and the cessation of NSAIDs. For patients with a known history
of ulcer, and in whom NSAID use is unavoidable, the lowest possible dose and
duration of the NSAID and co-therapy with a PPI or misoprostol are
recommended
Sunday, November 18, 2012 DR. RUBEL, SSMC 63
64. Medication(contd.)
PPI-based triple therapies for H pylori are considered the first-line therapies for
the treatment of H pylori in the United States with a cure rate of 85-90%. These
regimens consist of a PPI, amoxicillin, and clarithromycin for 7-14 days. A
longer duration of treatment (14 d vs 7 d) appears to be more affective and is
currently the recommended duration of treatment. Amoxicillin should only be
substituted by metronidazole in penicillin-allergic patients because of the high
rate of metronidazole resistance.
In the setting of active ulcers caused by H pylori, treatment with a PPI beyond
the 14-day course of antibiotics and until the confirmation for the eradication of
H pylori is recommended for complicated ulcers..
Sunday, November 18, 2012 DR. RUBEL, SSMC 64
65. PPI-based triple therapies consist of a 14-day treatment of the
following:
Omeprazole (Prilosec): 20 mg PO bid or
Lansoprazole (Prevacid): 30 mg PO bid or
Rabeprazole (Aciphex): 20 mg PO bid or
Esomeprazole (Nexium): 40 mg PO qd
Plus:
Clarithromycin (Biaxin): 500 mg PO bid and
Amoxicillin (Amoxil): 1 g PO bid
The alternative combination therapy consists of the following
treatments administered for 14 days:
Omeprazole (Prilosec): 20 mg PO bid or
Lansoprazole (Prevacid): 30 mg PO bid or
Rabeprazole (Aciphex): 20 mg PO bid or
Esomeprazole (Nexium): 40 mg PO qd
Plus:
Clarithromycin (Biaxin): 500 mg PO bid and
Metronidazole (Flagyl): 500 mg PO bid
Sunday, November 18, 2012 DR. RUBEL, SSMC 65
66. Quadruple therapies
for H pylori infection are generally reserved for patients
who have failed a course of treatment and are administered
for 14 days. The treatment includes the following drugs:
PPI PO bid and
Bismuth 525 mg PO qid and
Metronidazole 500 mg PO qid and
Tetracycline 500 mg PO qid
Sunday, November 18, 2012 DR. RUBEL, SSMC 66
67. Further Outpatient Care
Endoscopy is required to document healing of gastric ulcers and to rule out
gastric cancer. This usually is performed 6-8 weeks after the initial
diagnosis of PUD.
Documentation of H pylori cure with a noninvasive test, such as the urea
breath test or fecal antigen test, is appropriate in patients with complicated
ulcers
In/Out Patient Meds
Consider maintenance therapy with half standard doses of H2-receptor
antagonists at bedtime in patients with recurrent, refractory, or complicated
ulcers, particularly if cure of H pylori has not been documented or if an H
pylori-negative ulcer is present.
Sunday, November 18, 2012 DR. RUBEL, SSMC 67
68. PREVENTION
Primary prevention of NSAID-induced ulcers includes the
following:
Avoid unnecessary use of NSAIDs.
Use acetaminophen or nonacetylated salicylates when possible.
Use the lowest effective dose of an NSAID and switch to less toxic
NSAIDs, such as the newer NSAIDs or cyclooxygenase-2 (COX-2)
inhibitors, in high-risk patients without cardiovascular disease.
Consider prophylactic or preventive therapy for the
following patients:
Patients with NSAID-induced ulcers who require chronic, daily NSAID
therapy
Patients older than 60 years
Patients with a history of PUD or a complication such as
gastrointestinal bleeding
Patients taking concomitant steroids or anticoagulants or patients with
significant comorbid medical illnesses
Sunday, November 18, 2012 DR. RUBEL, SSMC 68
69. Prognosis
When the underlying cause is addressed, the prognosis is excellent.
Most patients are treated successfully with the cure of H pylori
infection, avoidance of NSAIDs, and the appropriate use of
antisecretory therapy.
Cure of H pylori infection changes the natural history of the disease,
with a decrease in the ulcer recurrence rate from 60-90% to
approximately 10-20%. However, this is a higher recurrence rate than
previously reported, suggesting an increased number of ulcers not
caused by H pylori infection.
Patient Education
Stop smoking.
Avoid NSAID and aspirin use.
Avoid heavy alcohol use.
Stress reduction counseling might be helpful in individual cases but is
not needed routinely.
.
DR. RUBEL, SSMC 69
Sunday, November 18, 2012
70. Summary
Most PU are caused by H. pylori or NSAIDs and changes in
epidemiology mirror changes in these principle etiological
factors.
DU are more common than GU, but the symptoms are
indistinguishable.
GU may become malignant and an ulcerated GU may mimic
a benign ulcer.
Gastric antisecretory agents and H. pylori eradication therapy
are the mainstay of treatment, and elective surgery is not now
commonly performed.
The common complication of peptic ulcer are perforation,
bleeding and stenosis.
The treatment of the perforated PU is primarily surgical,
although some patients may be managed conservatively.
Sunday, November 18, 2012 DR. RUBEL, SSMC 70