14.triangles of the neck and root of the
•Descargar como PPTX, PDF•
70 recomendaciones•27,149 vistas

The anterior triangle of the neck contains three smaller triangles - the submandibular, submental, and muscular triangles. The submandibular triangle contains the submandibular gland and associated nerves and vessels, including the lingual and hypoglossal nerves. The submental triangle drains lymph from the chin and lower lip. The muscular triangle contains the infrahyoid strap muscles that depress the hyoid bone during swallowing.

Recomendados
Más contenido relacionado
La actualidad más candente
La actualidad más candente (20)
Destacado
Destacado (20)
Similar a 14.triangles of the neck and root of the
Similar a 14.triangles of the neck and root of the (20)
Último
Último (20)
14.triangles of the neck and root of the
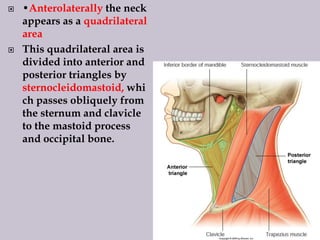
- 1. •Anterolaterally the neck appears as a quadrilateral area This quadrilateral area is divided into anterior and posterior triangles by sternocleidomastoid, whi ch passes obliquely from the sternum and clavicle to the mastoid process and occipital bone.
- 2. The ANTERIOR TRIANGLE lies anterior to the sternocleidomastoid muscle, while the POSTERIOR TRIANGLE lies posterior to the sternocleidomastoid muscle.
- 7. KIMAIGA H.O 1ST YEAR MBChB(UoN)
- 18. ANTERIOR TRIANGLE OF THE NECK BOUNDARIES Anteriorly- median line of the neck, Posteriorly-anterior margin of sternocleidomastoid. Base -inferior border of the mandible •and its projection to the mastoid process, •and its apexis at the manubrium sterni. Made of suprahyoid and infrahyoid areas above and below the hyoid bone, TRIANGLES HERE ARE: •Digastric/submandibular •Submental •Muscular •Carotid triangles By passage of digastric and omohyoid across the anterior triangle
- 20. Table of Muscles Muscle Origin Insertion Action Nerve Supply Sternohyoid sternum hyoid ansa Omohyoid Suprascapular notch hyoid ansa Sternothyroid Below sternohyoid on manubrium Thyroid cartilage oblique line ansa Thyrohyoid Thyroid cartilage oblique line hyoid C1-C2 (ansa) Anterior Belly Digastric ----intermediate tendon------ Inner surface of mandile Trigeminal nerve Posterior Belly Digastric Medial aspect of the mastoid process -intermediate tendon- Facial nerve Mylohyoid Mylohyoid line of mandible Hyoid bone Trigeminal nerve Hyoglossus Hyoid bone Lateral side of tongue hypoglossal Stylohyoid Styloid process hyoid Facial nerve
- 21. MUSCLE ORIGIN INSERTION ACTION INNERVATION Digastric •Digastric notch, •medial surface of base of mastoid process •Digastric fossa •Depress the mandible •Posterior belly: facial nerve •Anterior belly:nerve to mylohyoid Stylohyoid •Back of styloid process near the base of skull •By two slips into the junction between the greater horn and body of hyoid bone •ELevate hyoid bone •Facial nerve Mylohyoid •Whole length of mylohyoid line of its own side on the inner aspect of the mandible from medial to the third molar tooth to below the mental spines •Anterior ¾: into each other (interdigitation) •Posterior ¼: anterior surface of the body of hyoid bone •Forms a mobile but stable floor of the mouth •Mylohyoid nerve Geniohyoid •Inferior mental spine •Upper border of the body of hyoid bone. •Protracts and elevates the hyoid bone in swallowing or if the hyoid is fixed to depresses the mandible. •C1(superior root of ansa cervicalis)
- 22. Platysma is a broad sheet of muscle of varying prominence. •arises from the fascia covering the upper parts of pectoralis major and deltoid. •Its fibres cross the clavicle and ascend medially in the side of the neck. •Anterior fibres interlace across the midline with the fibres of the contralateral muscle, below and behind the symphysis menti. •Other fibres attach to the lower border of the mandible or to the lower lip or cross the mandible to attach to skin and subcutaneous tissue of the lower face.
- 24. Origin – fascia overlying the pectoralis major & deltoid muscle Insertion depression muscles of the corner of the mouth the mandible lower face Function wrinkles the neck depresses the corner of the mouth increases the diameter of the neck assists in venous return
- 26. Vascular supply •Platysma receives its blood supply from –the submental branch of the facial artery –and the suprascapular artery from the thyrocervical trunk of the subclavian artery. •Innervation •Platysma is innervated by the cervical branch of the facial nerve which descends on the deep surface of the muscle close to the angle of the mandible
- 27. Contraction diminishes the concavity between the jaw and the side of the neck and produces tense oblique ridges in the skin of the neck. •Platysma may assist in depressing the mandible, and via its labial and modiolar attachments it can draw down the lower lip and corners of the mouth in expressions of horror or surprise.
- 29. Origin Insertion mastoid process Nerve supply medial third of the clavicle (clavicular head) manubrium (sternal head) spinal accessory nerve (CNXI) Blood supply occipital a. or direct from ECA superior thyroid a. transverse cervical a.
- 30. Function – turns head toward opposite side & tilts head toward the ipsilateral shoulder Surgical considerations Leave overlying fascia (superficial layer of deep cervical fascia down) Lateral retraction exposes the submuscular recess
- 31. Origin Insertion via the intermediate tendon onto the clavicle and first rib hyoid bone lateral to the sternohyoid muscle Blood supply upper border of the scapula Inferior thyroid a. Function depress the hyoid tense the deep cervical fascia
- 32. The INFERIOR BELLY OF THE OMOHYOID MUSCLE crosses the posterior triangle as it spans from the hyoid bone to the scapula.
- 33. Surgical considerations Absent in 10% of individuals Landmark demarcating level III from IV Inferior belly lies superficial to the brachial plexus Phrenic nerve transverse cervical vessels Superior belly lies superficial to IJV
- 34. Origin digastric fossa of the mandible (at the symphyseal border) Insertion hyoid bone via the intermediate tendon mastoid process Function elevate the hyoid bone depress the mandible (assists lateral pterygoid)
- 35. Surgical considerations Posterior belly is superficial to ECA Hypoglossal nerve ICA IJV Anterior belly Landmark for identification of mylohyoid for dissection of the submandibular triangle
- 41. Origins and insertions on the mandible and hyoid
- 42. Origins and insertions on the mandible and hyoid
- 44. Omohyoid muscle (surgical landmark) Junction with IJV
- 46. Boundaries: Inferomedially: Anterior belly of digastric. Anterosuperiorly: Inferior border of the mandible. Inferolaterally: Posterior belly of digastric. Floor; Mylohyoid (forms diaphragm oris) hyoglossus middle constrictor muscle of the pharynx
- 48. ROOF OF SUBMANDIBULAR TRIANGLE: The skin. Superficial fascia Platysma Deep fascia containing branches of the facial and transverse cutaneous cervical nerves e.g. cervical branch of facial nerve
- 49. Removal of the superficial structures displays the submandibular salivary gland itself.
- 50. CONTENTS OF SUBMANDIBULAR TRIANGLE: Submandibular gland Hypoglossal nerve.XII Mylohyoid nerve. Facial artery and vein. Submandibular lymph nodes Lingual nerve and submandibular ganglion (ln) Submandibular duct (smd) Lingual artery (la) The lingual nerve and submandibular duct pass through a gap between the hypoglossal (hg) and mylohyoid (mh) muscles the lingual artery passes deep to the hyoglossus muscle.
- 51. Infection in submandibular region is limited to a triangular region. Posteriorly; hyoid bone and anterolaterally on each side by halves of mandibular base Because the layer of deep fascia is attached to these bones. Triangular swelling= Ludwig’s Angina The swelling may push tongue upwards
- 52. BOUNDARIES Apex –Inferior end of symphysis menti Laterally: Right and left anterior bellies of digastric. Base inferiorly -Body of the hyoid bone Floor - mylohyoid muscles.(mh) Arise from the body of the hyoid bone and insert into the mylohyoid line of the inside of the mandible. Aids in swallowing and in depressing the mandible.
- 54. CONTENTS OF SUBMENTAL TRIANGLE Submental lymph nodes. These receive lymph from the following areas: •Tip of the tongue. •Floor of the mouth. •Mandibular incisor teeth and associated gingivae •Central part of the lower lip. •Skin of the chin. Lymph from here drains into submandibular and deep cervical lymph nodes. Submental veins and arteries. The submental veins unite to form the anterior jugular vein.
- 55. In infections or cancer from any of the areas of drainage of the submental nodes, especially the tip of tongue and lip, the first nodes to be involved are submental nodes. Subsequently, the submandibular and deep cervical get involved. A discharging sinus on the point of the chin often results from an abscess of a mandibular incisor tooth. The pus from the infected tooth passes from the apex of the submental triangle located at the inferior end of the symphysis menti where it forms a sinus from which pus escapes.
- 56. BOUNDARIES Anteriorly -median line of the neck from the hyoid bone to the sternum, Inferoposteriorly by the anterior margin of sternocleidomastoid, Posterosuperiorly by the superior belly of omohyoid. Apex-jugular notch (3)
- 57. CONTENTS OF MUSCULAR TRIANGLE 1) Infrahyoid muscles (strap muscles). • Sternohyoid 1 • Sternothyroid • Thyrohyoid • Omohyoid* 2forming part of the boundary. NOTE: These muscles are innervated by ansa cervicalis (c1-c3) except thyrohyoid that is innervated by C1 via Hypoglossal nerve. They depress the hyoid bone and larynx during swallowing and speaking, anchoring it in position 2) The anterior jugular veins, run in both sides of the midline. They are joined by the jugular arch at the suprasternal notch. 1-Sternohyoid 2-Omohyoid 3-Sternal head of sternocleidomastoid
- 60. BOUNDARIES Superomedially Posterior belly of the digastric Laterally: Anterior border of the sternocleidomastoid muscle Inferomedially: superior belly of omohyoid
- 62. Skin and superficial fascia Platysma Deep fascia; ramifying in which are branches of the facial and cutaneous cervical nerves.
- 63. The muscles, at this level, are Thyrohyoideus, hyoglossus, the middle and inferior pharyngeal constrictors (mpc and ipc). The structures seen passing through this level are: superior laryngeal nerve, a branch of the vagus its 2 terminal branches internal laryngeal (ilb)sensory to upper part of the larynx external laryngeal (elb)motor to the Cricoid muscle)
- 64. common facial vein (cf) (within carotid triangle) Other structures near by: retromandibular vein (rm) posterior auricular vein (pav) facial vein (fv) external jugular vein (ej) anterior jugular vein (aj)
- 65. The nerves that enter the carotid triangle and that lie superficial to the internal jugular vein, internal and external carotid arteries are: hypoglossal (XII) C1 root of ansa cervicalis (C1) C1 fibers running with hypoglossal nerve (nerve to thyrohyoid muscle (nth) C2-C3 root of ansa cervicalis ansa cervicalis (ac)
- 67. cca-common carotid artery eca-external carotid artery sta-supterior thyroid artery oa-occipital artery la-lingual artery fa-facial artery ica-internal carotid artery
- 69. 1.masseter muscle 2. 5.parotid gland 8.facial artery 28.common carotid artery 29. internal carotid artery 30.external carotid artery 31. Superior thyroid artery 32. Ansa cervicalis
- 71. THE CAROTID SHEATH: Location: Longitudinal interval between cervical viscera (pharynx, esophagus, larynx, trachea and thyroid gland) medially, and prevertebral muscles posteriorly Formation: Prevertebral fascia behind Pretracheal fascia medially
- 72. Mnemonics Of Carotid Sheath Contents "I SEE(I.C)10 CC's IN THE IV" I SEE (I.C) = Internal carotid artery 10 = 10 cranial nerve (vagus nerve) CC = Common carotid artery IV = Internal juglar vein
- 74. CONTENTS OF CAROTID SHEATH 1. Common and Internal Carotid arteries medially. 2. Internal jugular vein laterally. 3. Vagus nerve posteriorly and between the above two. 4. Ansa cervicalis embedded in the carotid sheath(anteriorly). 5. Deep cervical lymph nodes. Note: 1) Common carotid artery divides at superior border of thyroid gland (C3,4). 2) The carotid sinus (the baroreceptor) is a slight dilatation at the proximal part of the internal carotid artery. It is innervated by: •Carotid sinus nerve, a branch of glossopharyngeal. •A branch of vagus nerve. •Sympathetic division of ANS. 3) The carotid body, is a small reddish brown, ovoid mass of tissue located at the carotid bifurcation. The same nerves that go to the carotid sinus innervate it.
- 75. A-Vagus nerve B-Comon carotid artery
- 76. COMMON CAROTID ARTERY ORIGIN Right: Brachio cephalic trunk- behind right sternoclavicular joint Left: Aortic arch – behind manubrium sterni Course Extends from sternoclavicular joint to upper border of thyroid gland c3/ c4 Anterolateral neck in the carotid sheath lateral to trachea/ esophagus and larynx/ pharynx Palpable between sternocleidomastoid and angle of the mandible Divides in the carotid triangle into internal and external carotid arteries Innervation Parasympathetic: Submandibular ganglion Sympathetic: superior cervical ganglion
- 77. BRANCHES OF EXTERNAL CAROTID ARTERY From the ventral side: From the Terminates by dorsal side: dividing into: •Superior •Occipital thyroid artery. artery. [7] [5] •Lingual artery. [4] •Facial artery. [3] •Ascending pharyngeal (may form from medial side). •Superficial temporal artery [1] •Posterior •Maxillary artery. [2] auricular. [6]
- 80. INTERNAL JUGULAR VEIN Origin Union of sigmoid and inferior petrosal sinuses Extent Base of skull to sternoclavicular joint Landmark Between sternal and clavicular heads of sterno cleido mastoid muscles Tributaries Pharyngeal veins Lingual Common facial Superior thyroid Middle thyroid Termination: Joins subclavian vein to form brachio-cephalic vein
- 81. VAGUS NERVE COURSE 1. Emerges through jugular foramen 2. Two ganglia- superior and inferior cervical ganglia 3. Runs straight down in the carotid sheath 4. Between and behind carotid artery and internal jugular veins 5. At the root of the neck, it passes infront of the subclavian artery to enter mediastinum
- 82. BRANCHES AND DISTRIBUTION Branch Meningeal Auricular Carotid body branch Pharyngeal branch Superior laryngeal External Laryngeal Internal Laryngeal Recurrent Laryngeal Cardiac branches Distribution •Dura of posterior cranial fossa •Postero inferior quadrant of external surface of tympanic membrane •Floor of external auditory meatus •Skin on the cranial auricular canal •Carotid body •Carotid sinus •Muscles of pharynx except stylopharyngeus •Muscles of soft palate except tensor palate • •Cricothyroid muscle •Inferior pharyngeal constrictors •Pharyngeal mucosa •Laryngeal mucosa above vocal folds •Trachea and Esophagus •Cricopharyngeus •Laryngeal muscles except cricothyroid •Laryngeal mucosa below vocal folds • •Heart
- 84. The scalene triangle/ gap is bounded by: 1. Posteriorly: Scaleneus medius 2. Anteriorly: Scaleneus anterior 3. Base: First rib Through this gap, pass the subclavian artery and the brachial plexus. Compression of these structures causes the scalenus anterior syndrome.
- 86. Posterior : anterior border of trapezius Base : middle 3rd of clavicle Apex : meeting point of sternocleidomastoid & trapezius at superior nuchal line. The inferior belly of omohyoid mscle, divides the posterior triangle into two; Occipital triangle Supraclavicular/ omoclavicular triangle.
- 87. The floor of the posterior triangle consists of four muscles, covered by the prevetebral layer of the deep cervical fascia. The splenius capitus, levator scapulae, ane the three scalenus muscles.
- 88. The anterior free edge of the TRAPEZIUS MUSCLE forms the posterior border of the posterior triangle.
- 89. The LEVATOR SCAPULAE MUSCLE forms a portion of the floor of the posterior triangle.
- 90. The SCALENE MEDIUS AND POSTERIOR MUSCLES complete the floor of the posterior triangle
- 91. The SCALENE ANTERIOR MUSCLE appears in the lower anterior corner of the triangle, often under the cover of the sternocleidomastoid muscle.
- 92. The PHRENIC NERVE can be observed on the anterior surface of the scalene anterior muscle.
- 93. The ROOTS AND TRUNKS OF THE BRACHIAL PLEXUS emerge from the interval between the scalene anterior and scalene medius & posterior muscles.
- 94. a. Skin b. Superficial facia c. Investing layer of deep cervical facia d. Roof is pierced by : 1. Nerves : i. Lesser occipital ii. Great auricle iii. Transverse cutaneous nerves of neck iv. Supraclavicular nerves 2. Veins : external jugular veins and its tributaries. 3. Lypmh vessels
- 95. 1. external jugular vein (blue) 2. superficial cervical lymph nodes (green) 3. lesser occipital nerve (lc) 4. great auricular nerve (ga) 5. transverse cervical nerve (tc) 6. supraclavicular nerves (sc) 7. spinal accessory nerve (sa)
- 96. Mainly form by 2nd layer of muscle of neck 1. Splenius capitis. 2. Levator scapulae. 3. Occasionally by semispinalis capitis at apex. 4. Scaleneus medius. 5. Scaleneus posterior. 6. Muscular floor is carpeted by preverterbral facia.
- 100. This vein is formed near the angle of the mandible by the union of the posterior branch of retromandibular and posterior auricular veins . • It crosses sternocleidomastoid muscle, runsover the roof of the triangle and joins the subclavian veins • The vein drains most of the scalp and face on the same side. • This vein dilates and becomes visible in fluid overload, in heart failure in SVC obstruction, prolonged raised intrathoracic pressure, e.t.c. • The walls of the vein are attached to the deep fascia. If the vein is lacerated, the fascia pulls the vein open and blleding is severe. Also, air embolism could follow.
- 103. External Jugular Vein is relatively superficial therefore: It can be easily lacerated Can be used to draw blood, infuse drugs or catheterize the heart is visible when distended in heart failure It pierces investing fascia therefore, when lacerated Can bleed profusely Predispose to air embolism
- 104. The subclavian artery (third part) -B • Transverse cervical artery from thyrocervical trunk to supply muscles in scapular region. • Suprascapular artery from the thyrocervical trunk. • Occipital artery, from the external carotid artery. Note the boundaries: A: Anterior scalene muscle B: Middle scalene muscle
- 105. The TRANSVERSE CERVICAL ARTERY crosses the posterior triangle. It divides into a deep branch which enters the floor of the triangle, and a superficial branch which passes laterally, deep to the trapezius muscle to travel with the spinal acessory nerve.
- 106. The SUPRASCAPULAR ARTERY AND VEIN crosses the lower portion of the posterior triangle just beneath the clavicle.
- 107. The spinal accessory nerve and the lymph nodes are the true contents of the posterior triangle . All others are behind or in front of the facial floor. a. Muscle : inferior belly of omohyoid b. Nerves : 1. 2. Accessory nerves Root, trunks of brachial plexus and their branches : i. ii. iii. iv. Nerves to rhomboideus Nerves tomserratus anterior Nerves to subclavius Suprascapular nerve
- 110. 3. Cervical nerves : i. ii. iii. iv. v. Greater occipital nerve emerges from the apex to pass on the scalp. Great auricle nerve Lesser occipital nerve Transverse cervical nerve of neck Supraclavicular nerve 3rd and 4th cervical nerves supplying trapezius
- 111. Spinal accessory nerve to the sternocleidomastoid muscle and the trapezius muscle. Cervical plexus and its cutaneous branches from up downwards. • Lesser occipital nerve (c2) • Great auricular nerve (c2 c3) • Transverse cervical nerve (c2 c3) Suprascapular nerves (c3c4) Supraclavicular part of the brachial plexus
- 112. runs upward over the sternocleidomastoi d muscle to supply the skin of neck and angle of the mandible.
- 113. traverses across the sternocleidomastoid muscle to supply the skin over the anterior triangle.
- 114. LESSER OCCIPITAL NERVE crosses the upper posterior edge of the sternocleidomastoid muscle to distribute to the scalp posterior to the ear.
- 115. The ANTERIOR and INTERMEDIATE SUPRACLAVICULA R NERVES are cutaneous branches of the cervical plexus over the anterior border of the clavicle.
- 117. The SPINAL ACCESSORY NERVE (CRANIAL NERVE IX) passes from behind the sternocleidomastoid muscle from slightly higher than the nerves of the cervical plexus. It innervates both the sternocleidomastoid and trapezius muscles.
- 118. The spinal accessory nerve (Cranial Nerve XI) pierces the anterior border of the sternomastoid muscle nerar its upper attachment and leaves the muscle at about the midpoint of its posterior border. The nerve then passes obliquely downward and laterally across the posterior triangle, but within a sleeve of the investing layer of deep cervical fascia. It enters the trapezius muscle at the inferolateral corner of the psoterior triangle.
- 119. The spinal accessory nerve runs in a very superficial position within the deep cervical fascai and may be injuried during surgical procedures of the superficial neck. It is at risk during surgery of the deep cervical lymph nodes, particularly to those of the juguloomohyoid group. Damage to the nerve will paralyze the trapezius muscle and cause severe limitations of upward rotation of the scapula such that the arm cannot be abducted beyond 90 degrees.
- 121. Originates in the spinal nucleus Extend to the fifth cervical segment Union of motor neurons Passes through two foramen Foramen Magnum – enters the skull posterior to the vertebral artery Jugular Foramen – exits the skull with CN IX, X and the IJV
- 123. Crosses the IJV Crosses lateral to the transverse process of the atlas Occipital artery crosses the nerve Descends obliquely in level II (forms and IIb Level IIa
- 124. 4. Arteries i. Occipital artery emerges from apex ii. 3rd part of subclavian artery and branches of subclavian artery a. Branches of thyrocervical trunk 1st part of subclavian-Transverse cervical, Suprascapular b. Transverse cervical artery divides into acending and descending branch anterior border of sternocleidomastoid. 5. Veins External jugular veins and its tributaries. Subclavian vein is lower down and not include in the triangle. 6. Lymph nodes : a. Supraclavicular lymph nodes along the posterior border of sternomastoid. b. Occipital lymph nodes
- 125. The transverse cervical and suprascapular arteries arise medial to the scalenus anterior muscle. To reach the posterior triangle they pass from medial to lateral, anterior to the scalenus anterior muscle. They cross the posterior triangle to reach the trapezius and scapular muscles respectively.
- 126. The dorsal scapular artery passes posteriorly through the brachial plexus to supply the posterior muscles of the back, specifically the rhomboids. It is usaully present in approximately 75% of individuals. In the remaining 25%, the dorsal scapular artery is absent. In these cases, the transverse cervical artery, while in route to the trapezius muscle, will give rise to a deep branch which will pass posterior to the scapula to supply the rhomboids. Once behind the scapula, the terminology of dorsal scapular artery applies regardless of its origin.
- 129. Nerve point of the neck: is the region around the midpoint of the posterior border of the sternocleidomastoid muscle. Several nerves lie superficially here, deep to the platysma. This point is important because: Slash wounds of the neck may severe these relatively superficial nerves , resulting in loss of cutaneous sensation in the neck, and posterior part of the scalp. Anaesthetic agent can be injected here. Brachial plexus block . Local anaesthetic solution is injected around the brachial plexus, superior to the midpoint of the clavicle. Be careful to locate the subclavian artery by palpation so it is not damaged. Subclavian artery, can be pressed in the suprascapular fossa, to control bleeding in the upper limb. Block dessection, is sometimes done in this region for the removal of lymph nodes. The accessory and Phrenic nerves, together with the other structures should be saved. Safe/ danger sides. The accessory nerve may be used to divide the posterior triangle into a carefree area superiorly and a danger area inferiorly, which has major nerves and blood vessels
- 130. The scalene hiatus is the trianglular gap in which rami and trunks of the brachial plexus and the subclavian artery pass between the scalenus anterior and medius muscles. It is bounded by the anterior and medial scalene muscles and the first rib to which the
- 131. 1) Left supracavicular (Virchow’s) lymph nodes are enlarge in malignancy of testis, stomach and other abdominal organs. 2) The pressure in the external jugular vein can be recorded in the recumbent position. It is increased in right sided heart failure and in the obstruction of the superior vena cava. 3) The retropharyngeal abscess maybe expressed in the lower part of posterior triangle.
- 133. CERVICAL PLEXUS
- 134. Results from damage to the cervical sympathetic chain. Therefore it presents with Ptosis Myosis Facial flushing on the affected site
- 135. Prevertebral and lateral muscles
- 137. Fascial planes of the Neck a) Investing layer b) Pretracheal layer c) Prevertebral
- 140. The fascia of the neck has a number of unique features. •The superficial fasciain the neck contains a thin sheet of muscle (the platysma), •Platysma begins in the superficial fascia of the thorax, •runs upwards to attach to the mandible •and blend with the muscles on the face, •is innervated by the cervical branch of the facial nerve [VII], and is only found in this location. FUNCTIONS 1.Affords the slipperiness which enables structures to move and pass over one another , without difficulty, e.g. during swallowing. 2.Allows twisting of the neck without it creaking like a manilla rope. 3.It allows a looseness that provides the easiest pathways for vessels and nerves to reach their destinations.
- 141. ATTACHMENTS Proximal External occipital protuberances Superior nuchal line Ligamentum nuchae Spines of cervical vertabra Mastoid process Lower border of the mandible Zygomatic arch Styloid process Hyoid bone Distal Acromion Clavicle Manubrium sterni
- 142. Encloses Sternomastoid muscle (1) Trapezius (2) Omohyoid muscle Parotid Submandibular gland Roofs Posterior triangle of the neck Anterior triangle of the neck Covers Infrahyoid muscles
- 143. In the Suprasternal notch, the investing fascia splits into two layers: One attaches to the anterior border of the manubrium The other to the posterior border This leaves a small suprasternal space containing: A little fat A lymph node Lower sections of the anterior jugular veins Jugular venous arch Sternal heads of sternomastoid
- 144. External jugular vein Cervical plexus Lymphatics
- 145. Attachments From hyoid bone to the superior mediastinum. Oblique lines of thyroid cartilage Cricoid cartilage The pericardium, and T. adventitia of the bases of great vessels. Becomes continous with bucopharyngeal fascia covering constrictor muscles behind
- 146. Thyroid gland (1) Infrahyoid muscles Air and food passages
- 147. The fascia at the back of the thyroid lobe is thickened to form a lateral ligament or “ligament of Berry” which gains attachment to the cricoid cartilage. At the level of the thyroid isthmus a looser attachment of the pretracheal fascia occurs infront of trachea.
- 148. Attachments Base of the skull Transverse process of cervical vertebrae Extends further down into the abdomen
- 149. Prevertebral muscles Scalene muscles Phrenic nerve Thus, it covers the floor of the posterior triangle of the neck Vertebral artery
- 150. In front of the subclavian artery, it is prolonged laterally as the cervico-axillary(axillary) sheath which invests the brachial pexus and the vessels. The carotid sheath – said to be derived from fusion or pretracheal and prevertebral fascia. Surrounds the • Common and the internal carotid arteries. • Internal jugular vein • vagus nerve
- 151. Investing Fascia: Forms a tight sheath for the glands especially the parotid, restricting swelling. Iinflammation of this glands causes pain due to high pressure. Pretracheal Fascia: The thyroid is completely enclosed in pretracheal fascia. The attachments to the larynx and trachea result in movement of the thyroid gland with larynx during swallowing. When a neck swelling moves in this way, it is almost certain to be associated with the thyroid gland. The Spaces around the pretracheal fascia provides for spread of infection. Thus infections from the head and neck can spread infront of the trachea or behind the esaophagus and reach the superior mediastinum . Prevertebral Fascia: The retropharyngeal space between pharynx and pre-vertebral fascia is clinically important because it frequently becomes infected secondary to upper respiratory tract infrections in childhood. The swelling appears on one side of the posterior pharyngeal wall and may obstruct the airway. In adults such infections are usually secondary to tuberculosis of the cervical vertebral column.
- 152. •the deep cervical fascia is organized into several distinct layers 1.an investing layer, which surrounds all structures in the neck; 2.the prevertebral layer, which surrounds the vertebral column and the deep muscles associated with the back; 3.the pretracheal layer, which encloses the viscera of the neck; 4.the carotid sheaths, which receive a contribution from the other three fascial layers and surround the two major neurovascular bundles on either side of the neck
- 153. The prevertebral layer is a cylindrical layer of fascia that surrounds the vertebral column and the muscles associated with it (Fig. 8.152). Muscles in this group include the prevertebral muscles, the anterior, middle, and posterior scalene muscles, and the deep muscles of the back. •The prevertebral fascia is attached posteriorly along the length of the ligamentumnuchae, and superiorly forms a continuous circular line attaching to the base of the skull. This circle begins
- 154. anteriorly as the fascia attaches to the basilar part of the occipital bone, the area of the jugular foramen, and the carotid canal; •continues laterally, attaching to the mastoid process; •continues posteriorly along the superior nuchal line ending at the external occipital protuberance, where it associates with its partner from the opposite side. •Anteriorly, the prevertebral column of fascia is attached to the anterior surfaces of the transverse processes and bodies of vertebrae CI to CVII.
- 155. The prevertebral fascia passing between the attachment points on the transverse processes is unique. In this location, it splits into two layers, creating a longitudinal fascial space containing loose connective tissue that extends from the base of the skull through the thorax. •There is one additional specialization of the prevertebral fascia in the lower region of the neck. The prevertebral fascia in an anterolateralposition extends from the anterior and middle scalene muscles to surround the brachial plexus and subclavian artery as these structures pass into the axilla. This fascial extension is the axillarysheath.
- 156. The pretracheal layerconsists of a collection of fascias that surround the trachea, esophagus, and thyroid gland (Fig. 8.152). Anteriorly, it consists of a pretracheal fascia that crosses the neck, just posterior to the infrahyoid muscles, and covers the trachea and the thyroid gland. The pretracheal fascia begins superiorly at the hyoid bone and ends inferiorly in the upper thoracic cavity. Laterally, this fascia continues and covers the thyroid gland and the esophagus. •posteriorly, the buccopharyngeal fascia forms the pretracheal layer and separates the pharynx and the esophagus from the prevertebral layer. •The buccopharyngeal fascia begins superiorly at the base of the skull and ends inferiorly in the thoracic cavity.
- 158. •The arrangement of the various layers of cervical fascia organizes the neck into four longitudinal compartments: •the first compartment is the largest, includes the other three, and consists of the area surrounded by the investing layer; •the second compartment consists of the vertebral column, the deep muscles associated with this structure, and is the area contained within the prevertebral layer; •the third compartment (the visceral compartment) contains the pharynx, the trachea, the esophagus, and the thyroid gland, which are surrounded by the pretracheal layer; •finally, there is a compartment (the carotid sheath) consisting of the neurovascular structures that pass from the base of the skull to the thoracic cavity, and the sheath enclosing these structures receives contributions from the other cervical fascias
- 159. FASCIAL SPACES •Between the fascial layers in the neck are spaces that may provide a conduit for the spread of infections from the neck to the mediastinum. •Three spaces could be involved in this process: 1.pretracheal space the first is the pretracheal spacebetween the investing layer of cervical fascia (covering the posterior surface of the infrahyoid muscles) and the pretracheal fascia (covering the anterior surface of the trachea and the thyroid gland), which passes between the neck and the anterior part of the superior mediastinum; 2.the second is the retropharyngeal spacebetween the buccopharyngeal fascia (on the posterior surface of the pharynx and esophagus) and the prevertebral fascia (on the anterior surface of the transverse processes and bodies of the cervical vertebrae), which extends from the base of the skull to the upper part of the posterior mediastinum 3.the third spaceis within the prevertebral layer covering the anterior surface of the transverse processes and bodies of the cervical vertebrae. This layer splits into two laminae to create a fascial space that begins at the base of the skull and extends through the posterior mediastinum to the diaphragm
- 160. 1) Describe the boundaries, sub divisions and their respective contents of the posterior triangle of the neck 2) Write short notes on: External jugular vein Cervical plexus Pretracheal fascia 3) Describe the attachments, extents, enclosures and applied anatomy of the investing cervical fascia
- 161. POSITION: Antero- inferior part of the neck Isthmus is midline between second and fourth tracheal rings The lobes are antero-lateral between C4 and C6 Lobes are between trachea and esophagus medially and carotid sheath laterally. Deep to platysma and strap muscles. 1. 2. 3. 4. 5. 6. 7. 8. Isthmus Left lobe of thyroid gland Right lobe of thyroid gland Cricothyroid Right common carotid artery Vagus nerve Thyroid cartilage Cricoid cartilage
- 162. ISTHMUS Anteriorly- Strap muscles, anterior jugular vein Posterior -Second to fourth tracheal rings Laterally -Continous with lobes Superiorly -Anastomosis of superior thyroid artery Inferiorly -Anastomosis of inferior thyroid artery
- 163. LOBES Antero laterally -Strap muscles, anterior jugular veins Posterior -Parathyroid glands, prevertebral muscles. Postero-laterally Carotid sheath and its contents common carotid artery (4), internal jugular vein (5) , vagus nerve (6). The sympathetic chain is nearby. Medially Larynx(1) pharynx and external laryngeal nerve above, trachea, oesophagus(2) and recurrent laryngeal nerve below.
- 164. Arterial • Inferior thyroid artery 2 from the thyrocervical trunk • Superior thyroid artery 1from the external carotid artery. • Occasional (unpaired) thyroidea ima (middle thyroid) from brachiocephalic trunk . • Several unnamed twigs from pharyngeal and tracheal vessels. All these arteries anastomose with each other.
- 165. • Superior thyroid vein (A) – Internal jugular vein • Middle thyroid vein (B) – Internal jugular vein • Inferior thyroid vein (C) – Brachio cephalic vein. The inferior thyroid veins cover the trachea inferior to the thymus. They constitute potential sources of haemorrhage in tracheostomy
- 166. Inferior deep cervical lymph nodes [1]. Prelaryngeal lymph nodes[2] Paratracheal lymph nodes[3]. Pretracheal lymph nodes.[4] Parasternal lymph nodes. Some may empty directly into the thoracic duct.
- 167. Autonomic innervation from the cervical sympathetic ganglia and vagus. This innervation is vasomotor and affects the gland indirectly through the action on blood vessels.
- 168. When the strap muscles are reflected, you can see the thyroid gland (tg) with its arteries (superior thyroid artery from the external carotid (sta) and the inferior thyroid artery from the thyrohyoid trunk from the subclavian (ita).
- 169. If the thyroid gland is reflected laterally, the structures making up the larynx and trachea are seen: Cartilages and membranes thyrohyoid membrane (thm) thyroid cartilage (Adam's apple)(tc) cricothyroid membrane and ligament (ctm) cricoid cartilage (cc) tracheal rings (tr)
- 174. The thyroid gland is hidden under the sternohyoid and sternothyroid muscles and consists of two lobes and an isthmus. An occasional pyramidal lobe extends upward near the mid line. The inferior thyroid artery is closely associated with the recurrent laryngeal nerve (rln).
- 175. Four small reddishbrown pea-sized glands may be seen on the deep surface of the thyroid gland. These are the superior and inferior parathyroid glands (ptg). Also note the close relationship of the recurrent laryngeal nerves to the thyroid gland and inferior thyroid artery (rln, ita).
- 176. • Thyroglossal duct cysts (TDC): May develop from a persistent thyroglossal duct anywhere along the course of the duct. The cysts may be in the tongue in the midline of the neck or retrosternal. TDC move up with protrusion of the tongue • Thyroglossal duct sinuses: Are openings into the skin from a patent part of the thyroglossal duct. They usually open in the neck and could be due to perforation of the cyst following infection. • Ectopic thryoid gland: Could be in the tongue, larynx, retrosternal or hyoid region.
- 177. • Goitre: This is an enlargement of the thyroid gland. It could be due to iodine deficiency, hormone or enzyme defect, infection or tumor. May be associated with hyperfunction or hypofunction . (What are the features of each?) Besides, goitre causes compression of the following: Trachea: affecting breathing. Oesophagus: affecting swallowing. Recurrent laryngeal nerve: affecting voice. A retrosternal goitre is worse for there is no space for expansion.
- 178. Thyroid gland in its capsule is enclosed by pretracheal fascia, which attaches inter alia to the hyoid bone. Thus, the thyroid gland moves upwards with swallowing and speech. This is a good test for masses in the neck. Thyroglossal cysts move when the tongue is protuded due to the attachment of the thyroglossal duct to the tongue. • The inferior thyroid artery runs close to the recurrent laryngeal nerve near the gland. Thus, the artery should be ligated further laterally to avoid injury to the nerve.
- 179. The superior thyroid artery is closer to the external laryngeal nerves superiorly than near the gland. Thus, this artery can be ligated as close to the gland as possible without danger of injury to the nerve. • In thyrodectomy, the recurrent laryngeal nerve must be preserved. The parathyroids must be identified and at least one spared. • Since colossal sizes of goitre may damage the recurrent laryngeal nerve, it is good habit to do laryngoscopy before thyroidectomy, so that preoperative damage can be distinguished from postoperative damage.
- 180. The cricothyroid ligament and membrane are frequently pierced in emergency situations to open the airway. It has been known that an empty ball-point pen or a hollow stem has been used in the field to save lives, where an air passage has been closed above this region.
- 181. STRUCTURES AT THE ROOT OF THE NECK Brachio cephalic trunk Subclavian artery and its branches Subclavian vein Termination of internal jugular vein Thoracic duct Apex of lung Phrenic nerve Vagus nerve
- 182. • • • • The brachiocephalic trunk. Right common carotid. Right subclavian. May also give thyroidea ima.
- 183. Divided into 3 parts by scalenus anterior muscle. Part 1: Medial to the muscle and gives 3 branches: • Vertebral artery : Enters foramen transversarium at C6 • Thyrocervical trunk : Inferior thyroid artery, transverse cervical artery and suprascapular artery. • Internal thoracic artery. Part 2: Posterior to the muscle and gives 1 branch, the costocervical trunk which gives superior intercostal and deep cervical arteries. Part 3: Lateral to the muscle, usually giving one branch (dorsal scapula). It may also occasionally give the suprascapular artery.
- 185. Branch Distribution relevant to respiration Vertebral •Respiratory center in the midbrain •Cervical cord segments that give phrenic nerve Internal thoracic •Intercostal muscles •Ribs and sternum •Thoracic diaphragm •Phrenic nerve •Abdominal wall Supreme Intercostal •1st two ribs Inferior thyroid •Trachea •Larynx •Cervical portion of spinal cord Transverse Cervical •Trapezium and Scapula muscles Suprascapular artery •Clavicle and scapula to which accessory muscles are attached
- 187. • External jugular veins. • Anterior jugular veins: These either drain into the external jugular or subclavian vein. The two veins are joined by the jugular venous arch, but could unite to form a single trunk in the midline of the neck. These veins have no valves. • The subclavian vein: A continuation of the axillary vein. This vein usually has only one named tributary, the external jugular vein. The veins that correspond to the arterial branches
- 188. The Vagus Nerve: This is cranial nerve 10. Located between common carotid and the internal jugular vein. This nerve gives the following branches in the neck: 1. Meningeal nerve: Recurrent to the dura. 2. Auricular nerve: Anastomoses with similar branches from the glossopharyngeal and facial nerves and supplies the pinnae and external auditory meatus. 3. Pharyngeal nerves: Join the pharyngeal plexus. 4. Superior laryngeal nerve: Divides into internal laryngeal and external laryngeal. 5. Recurrent laryngeal nerve: 6. Cardiac branches: Cardiac plexus.
- 189. Root value : C3, C4, C5 Course Descends obliquely on the anterior surface of scalenus anterior muscle Crosses first part of sub clavian artery on the left Crosses posterior to sub clavian vein on both sides Lies anterior to the internal thoraci artery Goes through thoracic inlet Distribution Parietal pericardium Parietal pleura Thoracic diaphragm Biliary apparatus
- 190. From T1 to T4. There are 3 ganglia, lies on pre-vertebral fascia behind carotid sheath Inferior cervical ganglion: At the level of the superior border of the neck of the first rib. It is commonly fused with the first thoracic ganglion to form cervicothoracic ganglion (Stellate ganglion). Middle cervical ganglion: On the anterior aspect of the inferior thyroid artery , at the level of cricoid cartilage pm the posterior aspect of inferior thyroid. Superior cervical ganglion: Located at the level of the axis and atlas / (C1/ C2) / angle of mandible. From these ganglia, postganglionic fibres reach their targets in four principal ways: Joining spinal nerves. Joining cranial nerves. Forming plexuses on blood vessels Directly. Provides secretomotor innervation to blood vessels and glands of the head and neck
- 191. There are lymph nodes within the carotid sheath, along the internal jugular vein. Another group runs along the transverse cervical artery. These, deep cervical lymph nodes are divided into superior and inferior, relative to the omohyoid muscle. The efferents drain into the jugular lymph trunk, which drains into the right lymphatic duct, or the thoracic duct. Both of these ducts enter the venous system, at the junction of the subclavian and the internal jugular veins.
- 192. They are small, yellowishbrown endocrine glands Located posterior to the thyroid, in their own capsule, but sharing the same fascial investment. The superior are thought to originate in the 4 th pharyngeal pouch. The superior ones are consistent in position. The inferior are inconsistent and could be found in the anterior mediastinum.
- 193. Blood supply Usually by the inferior thyroid arteries but may be supplied by the superior thyroid arteries or from longitudinal anastomosis between superior and inferior thyroid arteries. The veins drain into the thyroid plexus of the veins on the anterior surface of the thyroid. Lymphatics of the Parathyroid glands • Inferior deep cervical lymph nodes. • Paratracheal lymph nodes. The lymph vessels from here end in the thoracic duct. Innervation of the parathyroid glands Autonomic from the cervical sympathetic chain (and vagus). These are vasomotor.
- 194. The parathyroid glands are essential for regulation of blood calcium. (What are the functions of calcium in the body?) They are in danger of being destroyed or removed during thyroidectomy. Surgeons usually leave bits of the thyroid posteriorly or identify and preserve at least one of them.
- 195. Hyoid bone Thyrohyoid membrane Thyroid cartilage Cricothyroid membrane Cricoid cartilage 2 Crico-tracheal ligament Thyroid gland isthmus Tracheal rings Jugular venous arch. It is important to identify these important midline structures. (When and where is tracheotomy and laryngectomy done? What structures may be injured?)
- 196. Position Continuous with laryngopharynx at pharyngo esophageal junction Starts at lower border of cricoid cartilage (C6 vertebrae) and ends at thoracic inlet In the median plane Inclines slightly to the left
- 197. Anterior Posterior •Trachea •Longus coli •Recurrent •Body of C7 laryngeal nerve in tracheoesophagea l groove Right •Right lobe of thyroid •Right carotid sheath •Apex of right pleura Left •Left lobe of thyroid •Left carotid sheath •Left subclavian artery •Apex of left pleura •Thoracic duct
- 198. Musculature •Voluntary muscle •Outer longitudinal and inner muscle •Cricopharyngeal fibres of inferior constrictor act as a sphincter Blood supply •Segmental anastomosing esophageal branches of inferior thyroid artery •Veins drain into inferior thyroid vein Lymphatic drainage •Para tracheal nodes •Inferior deep cervical lymph nodes Innervation •Somatic motor and sensory: Recurrent laryngeal nerve •Vasomotor: Inferior cervical sympathetic ganglion through plexus on inferior thyroid artery
- 199. Position Found in the midline of the lower neck Continues from larynx into thoracic trachea Extends from lower edge of cricoid cartilage (C6) to thoracic inlet at T1 Inclines backwards as it descends
- 200. Relations Anterior Posterior •Isthmus of thyroid gland occassionaly pyramidal lobe and thyroidea ima if present •Inferior thyroid vein •Jugular venous arch •Sternohyoid and sternothyroid muscles •In babies left brachiocephalic vein and pleurae •Esophagus •Recurrent laryngeal nerve and inferior thyroid artery •Lateral •Lobes of thyroid gland •Carotid sheath and its contents •Brachiocephalic trunk on the right side
- 201. Blood supply •Inferior thyroid artery •Inferior thyroid vein Lymphatic drainage •Pre tracheal nodes •Paratracheal nodes •Inferior deep cervical nodes Innervation Sensory - Recurrent laryngeal nerve Sympathetic- Inferior cervical ganglion
- 202. Diagnosis (metastatic lymph node) Lymph node groups with the most likely sites of the primary lesion.
- 204. 1. 2. 3. 4. 5. 6. Give an account of the boundaries , contents and applied anatomy of the various subdivisions of the anterior triangle of the neck Describe the location , extents , relations , blood supply and lymphatic drainage of the thyroid gland. Add notes on the clinical importance of the topographic relations of the arteries and nerves of the thyroid State the boundaries , contents and clinical relevance of the scalene triangle and the triangle of the vertebral artery Give an account of the course ,origin,relations and distribution of the vagus nerve in the neck Describe the origin , course and distributions of the vertebral artery . Add a note on the clinical importance. Discuss the distribution of the first part of the subclavian artery