

Recomendados
Más contenido relacionado
La actualidad más candente
La actualidad más candente (20)
Destacado
Similar a Pelvic ureter
Similar a Pelvic ureter (20)
Último
Último (20)
Pelvic ureter
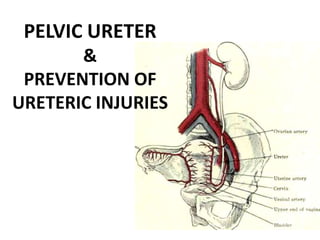
- 1. PELVIC URETER & PREVENTION OF URETERIC INJURIES
- 2. Retropritoneal spaces The retroperitoneal space of pelvic side walls contains: • Pelvic ureter • Internal iliac vessels • Pelvic lymph nodes • Obturator nerve
- 3. The pelvic ureter • Total length of ureter is 25-30 cm • Abdominal & pelvic portions are almost equal in length.
- 4. Abdominal & pelvic portions are almost equal in length, 12-15 cm
- 11. Structure From outside inwards 1. Fibres derived from the visceral layer of the pelvic fascia 2. Muscle coat: Outer: longitudinal Intermediate: circular Inner : longitudinal 3. Mucous layer : lined by Transitional epithelium
- 12. Ureter is comparatively constricted at 1. Where it crosses the pelvic brim 2. Where it is crossed by the uterine vessels 3. In the intravesical part
- 13. Blood supply • Segmental blood supply from nearly all the visceral branches of the anterior division of the internal iliac artery. • Venous drainage corresponds to the arteries.
- 14. Lymphatics • The lymphatics from the lower part drain into the external & internal iliac lymph nodes. • The upper part into the lumbar lymph nodes.
- 15. Nerve supply Sypathetic supply from: Hypogastric & Pelvic plexus Parasympathetic supply from: Sacral plexus
- 16. Development Ureter is developed as an ureteric bud which arises from caudal end of mesonephric duct.
- 17. Ureteric injuries • Overall incidence is 0.5 – 1 % of all pelvic operations • Incidence varies from 0.4 – 2.5 % for benign conditions as reported in different studies, but it can be as high as 30% in operations for malignancies
- 18. • About 75 % of ureteric injuries occur during an abdominal gynaecological surgeries with incidence 0.5 – 1 % for abdominal hysterectomy, compared to 0.1 % for vaginal hysterectomy.
- 19. Sites vulnerable to injury 1. At the pelvic brim during ligation of Infundibulo-pelvic ligaments. 2. At the base of the broad ligament, where it passes beneath the uterine arteries. 3. As it passes through it’s tunnel in the cardinal ligaments. 4. Along the course on lateral pelvic wall just above the uterosacral ligaments. 5. At the anterior fornix of vagina as it enters the bladder.
- 20. 6. Where it traverses through the musculature of bladder (Intra vesical part). 7. Lateral pelvic side wall over the iliac vessels during lymph node dissection. 8. Any congenital malformation eg. Duplex ureter makes it more vulnerable to injury at any of these sites.
- 21. Nature of ureteral injury 1. Simple kinking or angulation; obstruction 2. Ischaemic injury resulting from trauma to ureteric shaeth endangering its blood supply. 3. Ligation with suture. 4. Crushing injury by clamps. 5. Transection - partial or complete 6. Segmental resection - Accidental or planned. 7. Thermal injury, during laparoscopic surgeries. 8. Injury by staplers.
- 22. Gynaecological procedures associated with ureteric injuries Abdominal • Hysterectomy • Wertheim’s hysterectomy • Oophorectomy • Uterine suspension • Vesicovaginal fistula repair
- 23. Vaginal • Hysterectomy • Anterior colporrhaphy • Vesicovaginal fistula repair • Cervical biopsy Laparoscopic • Hysterectomy • Colposuspension • Treatment of endometriosis • Sterilisation (especially electrocoaguation)
- 24. • Goodno JA, Powers TW, Harris VD. Ureteral injury in Gynaecologic surgery: a ten year review in a community hospital. Am J Obstet Gynecol 1995; 172: 1817-1822 • Liapis A, Bakas P, Giannopoulos V, Creatsas G. Ureteral injuries during gynaecological surgery. Int Urogynecol J 2001; 12: 391-394
- 25. Significantly pelvic malignancies were present in 44 %. a/w dense adhesions, large masses displacing the ureter & anotomical changes distorting the course of the ureter.
- 26. However it should be noted that half of all the ureteric injuries had no identifiable risk factors & occur in so called ‘simple hysterectomy’
- 27. Distortion of pelvic anatomy 1. Cervical fibroid or low corporeal fibroid 2. Broad ligament tumours/ fibroids 3. Pelvic endometriosis 4. Large ovarian masses 5. PID 6. Gynaecological malignancies
- 28. 7. Prev. pelvic surgery 8. Pelvic haematoma 9. H/o pelvic irradiation 10.Ovarian remnant (when needs removal) 11.Congenital abnormalities like ureteric duplication, mega-ureter, ectopic ureter or kidney.
- 29. Prevention of ureteric injuries Preventive measures: • Pre operative intravenous urography • Placement of ureteric catheters. • Uriglow – ureteric catheters with incorporated light source.
- 30. Abdomino pelvic surgery • Adequate exposure • Most important axiom of surgery: Any imp structure at risk of inadvertent injury must be carefully dissected & adequately exposed. • To avoid blind clamping of blood vessels. • To not damage the shaeth of ureter; longitudinal vessels • Recognised by Pale glistening appearance, longitudinal vessels on surface, peristalsis.
- 31. 1. Divide the round ligament near the lateral pelvic side wall, then open the lateral peritoneum 10-15 cm in a cephalad direction. 2. Place an index finger on the external iliac artery, 3. By moving the finger upward (cephalad), the first structure to be exposed, crossing & in contact with the iliac artery, will be the ureter. 4. As the index finger is placed on the ureter, the infundibulopelvic lig. should be behind the middle phalanx, can be safely clamped with the ureter clearly visible. 5. Followed towards the cardinal lig. where it passes under the uterine artery; Push laterally & downward moving it away from cervix.
- 36. Vaginal surgery • To develop an adequate vesico-uterine space • To clamp, cut & ligate only small bites of paracervical & parametrial tissue • In post. culdoplasty ligation of uterosacrals to support vaginal apex after the uterus is removed can kink or obstruct the ureters if not done carefully. • Ant. colporrhaphy: Not to start too laterally or to insert deep sutures; distance between needle & ureter in upper third of vagina is only 0.9 cm (Hofmeister’s fluroscopic findings)
- 37. Laparoscopic surgery • Retroperitoneal dissection to locate ureters • Electrocoagulation of bleeding points around the uterosacral ligaments is risky, might better done with clips, sutures. • Sometimes width & length of the stapler makes safe application difficult; uterines,cardinals pedicles are better ligated vaginally.
- 38. Medicolegal considerations • The first step in risk management & prevention of litigation is at the initial consultaion for operation. • The necessity & risks associated with the procedure to be performed should be discussed in detail with the patient & properly documented In case notes.
- 39. KEY POINTS FOR CLINICAL PRACTICE • Thorough knowledge of the anatomy of the ureter is must & to be aware of the sites where it is liable to be injured. • Preop intravenous urography or stent placement has not been shown to decrease the incidence of ureteric injuries. • A high index of suspician & early investigations are necessary for diagnosis. • Early diagnosis & management will reduce postoperative morbidity & save renal loss. • Timings of repair should be individualised,as no difference in outcome in early & late repair.