
Recomendados
Más contenido relacionado
La actualidad más candente
La actualidad más candente (20)
Similar a 4 Restrictive Lung Diseases
Similar a 4 Restrictive Lung Diseases (20)
Más de Yaser Ammar
Más de Yaser Ammar (16)
Último
Último (20)
4 Restrictive Lung Diseases
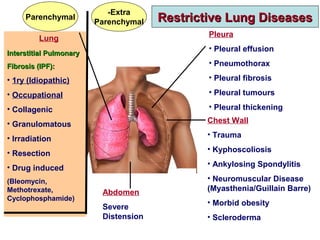
- 1. Lung Interstitial PulmonaryInterstitial Pulmonary Fibrosis (IPF):Fibrosis (IPF): • 1ry (Idiopathic) • Occupational • Collagenic • Granulomatous • Irradiation • Resection • Drug induced (Bleomycin, Methotrexate, Cyclophosphamide) Pleura • Pleural effusion • Pneumothorax • Pleural fibrosis • Pleural tumours • Pleural thickening Chest Wall • Trauma • Kyphoscoliosis • Ankylosing Spondylitis • Neuromuscular Disease (Myasthenia/Guillain Barre) • Morbid obesity • Scleroderma Abdomen Severe Distension Restrictive Lung DiseasesRestrictive Lung Diseases Extra- Parenchymal Parenchymal
- 3. Parenchymal RLD Extraparenchymal RLD FVC Decreased Decreased MVV Normal Decreased DLCO Decreased Normal FVC: Forced Vital Capacity MVV: Maximum Voluntary Ventilation DLCO: Carbon Monoxide Diffusion
- 4. Primary IPFPrimary IPF Diffuse Fibrosing AlveolitisDiffuse Fibrosing Alveolitis Usual Interstitial Pneumonia (UIP)Usual Interstitial Pneumonia (UIP) IPF is defined as a specific form of chronic, fibrosing interstitial pneumonia of unknown cause, typically affecting adults over 50 years, limited to the lungs, and associated with the histopathologic and/or radiologic pattern of usual interstitial pneumonia (UIP) It is the most frequent and devastating form of IPF (median survival 3 years).
- 5. Risk Factors for IPFRisk Factors for IPF Hereditary Acquired * Gene Mutations • Smoking (> 20 packs/year). • Pneumoconiosis. • GERD: microaspiration. • Viral infections (HCV, Herpes) • Autoimmunity.
- 6. Usual Interstitial Pneumonia (UIP) PatternUsual Interstitial Pneumonia (UIP) Pattern High Resolution Computed Tomography (HRCT) 1) Subpleural, basal predominance. 2) Honeycombing. 3) Reticular pattern. 4) Absence of features of alternative diagnosis, eg, - Upper or mid lung predominance. - Segmental or lobar consolidation. Histopathology 1) Marked fibrosis + honeycombing in a predominantly subpleural distribution. 2) Patchy pulmonary fibrosis. 3) Fibroblast foci. 4) Absence of features of alternative diagnosis, eg, granulomas, infection.
- 7. N
- 8. CO2 is much more diffusible than O2. Therefore, the diffusion defect affects O2 not CO2. So, we get hypoxia, not hypercapnoea.
- 10. IPF Stiff Lungs (Low Compliance) Restrictive Hypoventilation Exertional Dyspnoea V/Q Mismatch Diffusion Defect HYPOXIA Leathery Crepitations Central Cyanosis Clubbing Dry Cough Clinical Features End inspiratory, persist after cough ↑Pulmonary Vascular Resistance Pulmonary Hypertension Rt Ventricle Hypertrophy, Failure
- 11. Disease Onset Acute or Subacute )Hamman Rich Syndrome( Insidious • Rare. • Rapidly progressive, severe • Fatal within few months • Most cases. • Slowly progressive dyspnoea • Cyanosis may be only exertional )short time for gas exchange(.
- 13. Acute Exacerbation of IPFAcute Exacerbation of IPF Diagnostic Criteria • Previous or concurrent diagnosis of idiopathic pulmonary fibrosis. • Unexplained worsening or development of dyspnea within 30 days. • HRCT with new bilateral ground-glass abnormality and/or consolidation superimposed on background reticular or honeycomb pattern consistent with UIP. • Exclusion of alternative causes: Infection Left heart failure Pulmonary embolism
- 15. Cause of Death in IPF IPF ]N=543[ 1-7year Follow up 60%Died ]N=326[ Respiratory failure 39% Lung cancer 10% Pulmonary embolism 3% Pulmonary infection 3% Cardiovascular disease 27% Other 18%
- 16. InvestigationsInvestigations• Spirometry. • Chest X-Ray. • HRCT. • ABG / Oxymetry • DLCO. • Auto Antibodies: ANA, RF )+ve in up to 20% of cases(. • Lung Biopsy. • 6 Minute Walk Test
- 17. Walk Tests Treadmill Corridor Time Based 2 MWT 6 MWT 12 MWT Distance Based Velocity Based
- 18. 6 Minute Walk Test
- 19. • A test of aerobic capacity and endurance. • Tests the global and integrated responses of all systems involved during exercise, including pulmonary, cardiovascular and neuromuscular systems. • Does not provide specific information on each system/organ. Advantages • Easy, affordable )no need for expensive equipment or advanced technician training(. • Reflective of ADL )activities of daily living(: self-paced and done at submaximal exercise capacity, like ADL. • Safe. • Strongly correlated with peak O2 uptake in many pulmonary conditions.
- 21. Indications It is used in many chronic cardiac (coronary heart disease, heart failure) and respiratory (COPD, IPF) conditions for: • Assessment of Functional Status. • Prediction of Morbidity, Mortality. • Pre-Treatment, Post-Treatment Comparison. Contraindications • Absolute: Unstable angina or myocardial infarction during last month. • Relative: - HR > 120 or < 50 bpm. - BP > 180/100 mmHg. Revise a recent ECG and revise the need for the test - O2 Saturation < 88%>
- 22. Instructions • Usual walking aids used. • Usual drug regimen continued. • Supplemental O2 continued. • Warming up period not allowed. • Sit at rest on a chair near the start line for > 10 mins before the test starts. • STOP in case of: - Chest pain - Staggering - Intolerable dyspnoea - Diaphoresis - Leg cramps - Pallor
- 23. What to Record at End of Test • 6MWD (absolute value and percent of predicted value). • Pulse, BP, RPP (Rate Pulse Product, a measure of myocardial exertion). • Perceived dyspnoea, perceived exertion (modified Borg scale). • O2 saturation.
- 24. Treatment of IPF:Treatment of IPF: Non-Pharmacologic TreatmentNon-Pharmacologic Treatment • Home Oxygen Therapy If there is hypoxaemia (O2 Saturation < 88%) at rest or induced by 6MWT. • Respiratory Rehabilitation improves distance of 6MWT and improves health- related quality of life. • Lung Transplantation The only treatment in advanced IPF that results in a major functional improvement.
- 25. PPI + Anti-Reflux measures IV Methyl Prednisolone 500-1000 mg/day for 3 days then Prednisone 0.5 mg/Kg/day, gradually tapered Established role
- 26. Pirfenidone (Pirfenex)Pirfenidone (Pirfenex) • The only drug with confirmed efficacy against IPF. • The only drug that was specifically licensed for treatment of IPF. • FDA approved for this indication in 2014. • ↓ Fibroblast proliferation, ↓ TGF-β stimulated collagen production → Anti-Fibrotic effect • Has also an anti-inflammatory effect. • IPF is a fibroblast- activated process. Inflammation is a 2ry event. • ↓ Disease progression, ↓ decline in FVC, ↑ exercise capacity. • Dose: One capsule (200 mg) / 8 h for 1 week 2 capsules / 8 h for 1 week 3 capsules / 8 h thereafter, for at least 12 months. • Continued longer if there is some disease improvement or stabilization.
- 27. Adverse Effects, CautionsAdverse Effects, Cautions Adverse EffectAdverse Effect CautionCaution GI Upset (N, V, dyspepsia) Taken after food to ↓ these upsets (though food significantly ↓ its absorption) Anorexia and Weight Loss Monitor weight, ↑ caloric intake if needed. Photosensitivity Avoid exposure to sunlight, use sunscreen. ↑ Transaminases Check at baseline, monthly for 6 M, then every 3 M Dizziness Avoid before driving vehicles
- 28. InteractionsInteractions It is metabolized through CYP1A2 enzyme pathway: Inducers ↓ Effect • Smoking: quit. • Omeprazole: Use pantoprazol Inhibitors ↑ Toxicity • Fluvoxamine (Faverine): Contraindicated. • Ciprofloxacin, Amiodarone: Caution
- 29. ContraindicationsContraindications • End- stage liver disease. • End- stage renal disease. • Concomitant Fluvoxamine. • Pregnancy.
- 30. Occupational IPFOccupational IPF (Pneumoconeosis)(Pneumoconeosis) Organic Dust Inorganic Dust • Cotton: Byssinosis • Sugar Cane: Bagassosis •Silica: Silicosis • Asbestos: Asbestosis
- 31. Progression can occur after exposure has ceased, due to the retention of fibers in the lung and persistent inflammatory/fibrotic response. AsbestosisAsbestosis
- 32. Asbestosis Containing MaterialsAsbestosis Containing Materials • Asbestos is a broad term that includes a group of naturally occurring fibrous mineral silicates of magnesium and iron. • Asbestos content varies in different materials (1%-100%). • Asbestos rich materials include: • Wall and ceiling insulators • Floor and Ceiling tiles • Cement pipes • Brake and clutch pads.
- 33. • Asbestos fibers are remarkably insulator to heat, electricity and sound, so they were widely used in industry. • Asbestos tends to break into very tiny fibers which remain suspended in air for hours or days. •Asbestos fibers are resistant to acid, alkali, water, heat and flame. So, they are environmentally persistent, not biodegradable and virtually indestructible.
- 34. Routes of ExposureRoutes of Exposure • Asbestos containing material is not generally considered harmful unless it is releasing dust or fibers into the air where they can be inhaled or (less frequently) ingested. • Many of the fibers will become trapped in the mucous membranes of the nose and throat where they can then be removed, but some may pass deep into the lungs, or, if swallowed, into the digestive tract. • People at risk: o Construction workers. o Car mechanics. o Those exposed at home.
- 35. Pleuro-Pulmonary Disease due to AsbestosisPleuro-Pulmonary Disease due to Asbestosis Benign • Pleural Disease – Pleural Thickening (localized or diffuse): commonest health consequence of asbestos exposure. – Pleural Effusion – Rounded Atelectasis • Lung Disease (Asbestosis): IPF (Latency 15 - 20 Y) Malignant • Pleural mesothelioma • Peritoneal mesothelioma • Lung Cancer Cause of Death: • Cancer: - Bronchial Carcinoma: most common cause of death - Mesothelioma less common but more characteristic. • Respiratory Failure.
- 36. Determining Factors for Development ofDetermining Factors for Development of Asbestos- Related DiseaseAsbestos- Related Disease – Level, frequency, and duration of exposure. There is no “safe” level; any exposure is risky. – Time elapsed since exposure – Age at time of exposure Younger persons more likely to develop disease. – Smoking history (significantly ↑ risk of lung cancer). – Individual susceptibility factors (?)
- 37. • Considered a “signal neoplasm” because of its rarity in absence of exposure to asbestos. • Latency: ≥ 20 years. • Presenting symptoms often are chest pain and dyspnea, due to pleural effusions. • Rapidly invasive. • At high concentrations: cancer of GIT, kidney, pancreas. Mesothelioma of Pleura / Peritoneum
- 38. Prevention / Risk Reduction • Never “disturb” asbestos containing materials: Drill, Hammer, Cut, Saw, Break, Move. • Smoking Cessation. • Influenza / Pneumococcal vaccine. • Warning labels on asbestos containing materials.
Notas del editor
- Restrictive lung diseases are broadly classified into parenchymal and extra-parenchymal groups Parenchymal restriction results from diseases involving the lung itself. Interstitial pulmonary fibrosis (IPF) is the most common and most serious among these parenchymal disorders. Collagenic diseases: like rheumatoid arthritis, scleroderma, systemic lupus erythematosus Granulomatous: as sarcoidosis Irradiation: eg, for cancer breast Resection of part of lung tissue leads to actual loss of functioning parenchyma. Ankylosing spondylitis: chronic inflammatory condition of the spine (vertebral column: spondylitis) with partial fusion of the vertebrae and limitation of their movement (ankylosis). The mobility of the joints between ribs and vertebral column (costovertebral joints) is encroached upon.
- Reminder about respiratory functions In obstructive disease, air trapping leads to marked increase of RV. Consequently, FRC and TLC (which include RV) are also increased. Vital capacity as a whole may be slightly decreased, but limitation of expiratory airflow leads to marked diminution of the earliest (and normally greatest) part of expiratory FVC (FEV1). So, we get marked decrease of FEV1/FVC. In restrictive disease, all lung volumes and capacities are decreased.
- Smoking index: number of packs consumed daily, multiplied by number of years of smoking
- Plain X-Ray chest: Early: ground glass Late: honeycomb
- Both Oxygen saturation &lt; 88% and distance covered are predictors of mortality.
- 6MWD: 6 minute walk distance
- Chest X Ray showing bilateral pleural thickening due to asbestosis.
- Mesothelioma of diaphragmatic pleura.