

Recomendados
Recomendados
Más contenido relacionado
La actualidad más candente
La actualidad más candente (11)
Similar a Annual report 2067_68_final
Similar a Annual report 2067_68_final (20)
Último
Último (15)
Annual report 2067_68_final
- 1. A n nual R e p o rt Department of Health Services 206 2067/68 (2010/2011) GOVERNMENT OF NEPAL MINISTRY OF HEALTH AND POPULATION DEPARTMENT OF HEALTH SERVICES KATHMANDU
- 5. *RYHUQPHQW RI 1HSDO 0LQLVWU RI +HDOWK DQG 3RSXODWLRQ '(3$570(17 2) +($/7+ 6(59,&(6 2JQPG 0Q 3DFKDOL 7HNX .DWKPDQGX 1HSDO (QTGYQTF ,W LV P JUHDW SOHDVXUH WR SUHVHQW WKH $QQXDO 5HSRUW RI WKH 'HSDUWPHQW RI +HDOWK 6HUYLFHV WKH WK LQ D FRQVHFXWLYH VHULHV 7KH DQQXDO UHSRUW LV D PDMRU RXWFRPH RI WKH DQQXDO SHUIRUPDQFH UHYLHZ ZRUNVKRSV FRQGXFWHG DW QDWLRQDO UHJLRQDO DQG GLVWULFW OHYHOV ,W UHIOHFW DQG GRFXPHQW WKH SHUIRUPDQFH RI DOO WKH PDMRU SURJUDPV DQG DFWLYLWLHV FDUULHG RXW E YDULRXV KHDOWK LQVWLWXWLRQV DW DOO OHYHOV IURP WKH FRPPXQLW WR WKH FHQWHU 7KH IDFWV SUHVHQWHG LQ WKH UHSRUW DUH PDLQO EDVHG RQ LQIRUPDWLRQ PDQDJHG E WKH +HDOWK 0DQDJHPHQW ,QIRUPDWLRQ 6HFWLRQ +0,6 DV ZHOO DV RWKHU VRXUFHV ZLWKLQ WKH KHDOWK VVWHP 7KH UHSRUW SURYLGHV FRPSUHKHQVLYH LQIRUPDWLRQ DERXW KHDOWK FDUH DFWLYLWLHV SURJUDPV SROLFLHV VWUDWHJLHV DFKLHYHPHQWV DQG WKUHH HDUV RI VHUYLFH FRYHUDJH DV ZHOO DV SUREOHPV DQG FRQVWUDLQWV IRXQG GXULQJ WKH ILVFDO HDU 7KH UHSRUW DOVR FRYHUV WKH SURJUHVV RI DFWLYLWLHV FDUULHG RXW E RWKHU GHSDUWPHQWV XQGHU WKH 0LQLVWU RI +HDOWK DQG 3RSXODWLRQ DQG H[WHUQDO GHYHORSPHQW SDUWQHUV ,1*2V DQG 1*2V GXULQJ WKH UHIHUHQFHG HDU , DP SOHDVHG WR QRWH WKDW PRVW RI WKH DFWLYLWLHV SODQQHG E GLIIHUHQW 'LYLVLRQV DQG &HQWHUV KDYH EHHQ FDUULHG RXW VXFFHVVIXOO DQG WKH WUHQG RI VHUYLFH FRYHUDJH IRU PRVW KHDOWK LQGLFDWRUV LV VDWLVIDFWRU 'XULQJ WKH QDWLRQDO UHYLHZ SHULRG PDQ KHDOWK VHUYLFHV FRYHUDJH LQGLFDWRUV VKRZHG LPSURYHPHQW 7KH UHPDUNDEOH DFKLHYHPHQW RI FRPPXQLW EDVHG SURJUDPV SURJUHVV LQ FRQWURO DQG SUHYHQWLRQ RI HSLGHPLFV DQG QXPEHUV RI QHZ 23' YLVLWV JLYHV VDWLVIDFWLRQ 6WUHQJWKHQLQJ DQG H[SDQVLRQ RI VDIH PRWKHUKRRG VHUYLFHV FRPSUHKHQVLYH DERUWLRQ FDUH WKH PDWHUQLW LQFHQWLYH VFKHPH DQG EDVLF DQG FRPSUHKHQVLYH (PHUJHQF 2EVWHWULF &DUH (2& VHUYLFHV KDYH EHHQ FDUULHG RXW VXFFHVVIXOO +RZHYHU PRUH FROODERUDWLYH HIIRUWV DUH UHTXLUHG IRU LPSURYHPHQW WR PHHW WKH DVSLUDWLRQV RI WKH SHRSOH DQG WR GHOLYHU TXDOLW KHDOWK FDUH VHUYLFHV DV HQYLVDJHG E WKH 0'* KHDOWK VHFWRU JRDOV DQG QDWLRQDO SODQ GRFXPHQWV , ZRXOG OLNH WR H[WHQG P DSSUHFLDWLRQ WR )HPDOH &RPPXQLW +HDOWK 9ROXQWHHUV )&+9V JUDVVURRWV OHYHO KHDOWK ZRUNHUV 3+&& +3 6+3 DQG GLVWULFW OHYHO VWDII PHPEHUV IRU WKHLU XQWLULQJ HIIRUWV LQ SURYLGLQJ SULPDU KHDOWK VHUYLFHV DW WKH FRPPXQLW OHYHO , WKDQN WKH 5HJLRQDO +HDOWK 'LUHFWRUV 'LUHFWRUV RI 'LYLVLRQV DQG &HQWHUV DQG 6HFWLRQ &KLHIV IRU WKHLU VXSSRUW WR WKH GLVWULFW WHDPV WR H[HFXWH WKHLU DFWLYLWLHV LQ D WLPHO PDQQHU , DOVR ZLVK WR RIIHU P DSSUHFLDWLRQ WR WKH 1*2V ,1*2V H[WHUQDO GHYHORSPHQW SDUWQHUV DQG SULYDWH KHDOWK VHFWRU IRU FRQWULEXWLQJ VLJQLILFDQWO WR LPSURYH WKH KHDOWK VWDWXV RI SHRSOH LQ DOO FRUQHUV RI WKH FRXQWU )LQDOO , ZRXOG OLNH WR H[WHQG P DSSUHFLDWLRQ DQG WKDQNV WR WKH 'LUHFWRU DQG KLV 0DQDJHPHQW 'LYLVLRQ WHDP DQG HVSHFLDOO WKH 0DQDJHPHQW ,QIRUPDWLRQ 6HFWLRQ WHDP IRU WKHLU PHWLFXORXV DQG KDUG ZRUN LQ EULQJLQJ RXW WKLV $QQXDO 5HSRUW 'U <DVKRYDUGKDQ 3UDGKDQ 'LUHFWRU *HQHUDO (GDTWCT[
- 6. *RYHUQPHQW RI 1HSDO 0LQLVWU 2I +HDOWK DQG 3RSXODWLRQ 'HSDUWPHQW RI +HDOWK 6HUYLFHV 0DQDJHPHQW 'LYLVLRQ 7HO )D[ 3DFKDOL 7HNX .DWKPDQGX 1HSDO ĐŬŶŽǁůĞĚŐĞŵĞŶƚ /ƚ ŝƐ ŵLJ ŝŵŵĞŶƐĞ ƉůĞĂƐƵƌĞ ƚŽ ŽĨĨĞƌ ƚŽ ŽƵƌ ƌĞĂĚĞƌƐ ƚŚĞ ƐĞǀĞŶƚĞĞŶƚŚ ŶŶƵĂů ZĞƉŽƌƚ ŽĨ ƚŚĞ ĞƉĂƌƚŵĞŶƚ ŽĨ ,ĞĂůƚŚ ^ĞƌǀŝĐĞƐ͕ ĨŽƌ ƚŚĞ ĨŝƐĐĂů LJĞĂƌ ϮϬϲϳͬϲϴ ;ϮϬϭϬͬϮϬϭϭͿ͘ dŚĞ ƌĞƉŽƌƚ ŝƐ ƚŚĞ ŽƵƚĐŽŵĞ ŽĨ ƚŚĞ ĂŶŶƵĂů ƉĞƌĨŽƌŵĂŶĐĞ ƌĞǀŝĞǁ ǁŽƌŬƐŚŽƉƐ ĐŽŶĚƵĐƚĞĚ Ăƚ ǀĂƌŝŽƵƐ ůĞǀĞůƐ ŽĨ ŚĞĂůƚŚ ƐĞƌǀŝĐĞ ĚĞůŝǀĞƌLJ͘ /ƚ ŝƐ Ă ĐŽŵƉŝůĂƚŝŽŶ ŽĨ Ăůů ƚŚĞ ŵĂũŽƌ ĂĐƚŝǀŝƚŝĞƐ ĐĂƌƌŝĞĚ ŽƵƚ ďLJ ǀĂƌŝŽƵƐ ŚĞĂůƚŚ ŝŶƐƚŝƚƵƚŝŽŶƐ Ăƚ Ăůů ůĞǀĞůƐ ĨƌŽŵ ƚŚĞ ĐŽŵŵƵŶŝƚLJ ƚŽ ƚŚĞ ĐĞŶƚĞƌ͘ dŚĞ ĚĂƚĂ ƉƌĞƐĞŶƚĞĚ ŝŶ ƚŚŝƐ ƌĞƉŽƌƚ ŝƐ ďĂƐĞĚ ŽŶ ƚŚĞ ŝŶĨŽƌŵĂƚŝŽŶ ƐƵďŵŝƚƚĞĚ ďLJ ƚŚŝƐ ŝŶƐƚŝƚƵƚŝŽŶ ƚŽ ƚŚĞ ,ĞĂůƚŚ DĂŶĂŐĞŵĞŶƚ /ŶĨŽƌŵĂƚŝŽŶ ^LJƐƚĞŵ ;,D/^Ϳ ƐĞĐƚŝŽŶ͕ DĂŶĂŐĞŵĞŶƚ ŝǀŝƐŝŽŶ͕ ĞƉĂƌƚŵĞŶƚ ŽĨ ,ĞĂůƚŚ ^ĞƌǀŝĐĞƐ͘ /Ŷ ƚŚƌĞĞ ĚŝƐƚƌŝĐƚƐ ʹ >ĂůŝƚƉƵƌ͕ WĂƌƐĂ ĂŶĚ ZƵƉĂŶĚĞŚŝ ʹ ƉŝůŽƚŝŶŐ ŚĂƐ ďĞĞŶ ĐŽŶƚŝŶƵĞĚ ƚŽ ŐĞŶĞƌĂƚĞ ĐŽŵƉƌĞŚĞŶƐŝǀĞ͕ ŝŶƚĞŐƌĂƚĞĚ ĂŶĚ ĚŝƐĂŐŐƌĞŐĂƚĞĚ ŚĞĂůƚŚ ƐĞƌǀŝĐĞ ƐƚĂƚŝƐƚŝĐƐ ƚŚƌŽƵŐŚ ƚŚĞ ,ĞĂůƚŚ ^ĞĐƚŽƌ /ŶĨŽƌŵĂƚŝŽŶ ^LJƐƚĞŵ ;,^/^Ϳ͘ dŚĞ ƌĞƉŽƌƚ ƌĞĨůĞĐƚƐ ŝŶĨŽƌŵĂƚŝŽŶ ĂďŽƵƚ ŚĞĂůƚŚ ĐĂƌĞ ĂĐƚŝǀŝƚŝĞƐ͕ ŝŶĐůƵĚŝŶŐ ďƌŝĞĨ 'ŽĂůƐ͕ KďũĞĐƚŝǀĞƐ͕ ĂĐŬŐƌŽƵŶĚ ĂŶĚ ^ƚƌĂƚĞŐŝĞƐ ĂĚŽƉƚĞĚ ďLJ ƚŚĞ ƉƌŽŐƌĂŵƐ͘ /ƚ ĂŶĂůLJnjĞƐ ƚŚĞ ĂĐŚŝĞǀĞŵĞŶƚƐ ŽĨ ŵĂũŽƌ ĂĐƚŝǀŝƚŝĞƐ͕ ŚŝŐŚůŝŐŚƚŝŶŐ ƚŚĞ ƚƌĞŶĚƐ ŝŶ ƐĞƌǀŝĐĞ ĐŽǀĞƌĂŐĞ ĂŶĚ dĂƌŐĞƚ ǀƐ͘ ĐŚŝĞǀĞŵĞŶƚƐ ǁŝƚŚ ƌĞƐƉĞĐƚ ƚŽ ďƵĚŐĞƚ ĂůůŽĐĂƚŝŽŶ ĂŶĚ ĞdžƉĞŶĚŝƚƵƌĞ͘ dŚĞ ƌĞƉŽƌƚ ŶŽƚ ŽŶůLJ ŝĚĞŶƚŝĨŝĞƐ ƉĞƌƚŝŶĞŶƚ ŝƐƐƵĞƐ͕ ƉƌŽďůĞŵƐ ĂŶĚ ĐŽŶƐƚƌĂŝŶƚƐ͕ ďƵƚ ĂůƐŽ ƐƵŐŐĞƐƚƐ ĂĐƚŝŽŶƐ ƚŽ ďĞ ƚĂŬĞŶ ƚŽ ĂĚĚƌĞƐƐ ƚŚĞƐĞ ŝƐƐƵĞƐ ŝŶ ŽƌĚĞƌ ƚŽ ŝŵƉůĞŵĞŶƚ ƚŚĞ ĂĐƚŝǀŝƚŝĞƐ ƉůĂŶŶĞĚ͘ dŚĞ ƌĂǁ ĂŶĚ ĂŶĂůLJnjĞĚ ĚĂƚĂ ƐŚĞĞƚƐ ƉƌĞƐĞŶƚĞĚ ĂƐ ĂŶ ĂŶŶĞdž ƚŽ ƚŚĞ ƌĞƉŽƌƚ ƉƌŽǀŝĚĞ ĚĞƚĂŝůƐ ĂŶĚ ĨƵƌƚŚĞƌ ĂŶĂůLJƐŝƐ͘ dŚĞ ŝŶĨŽƌŵĂƚŝŽŶ ƉƌŽǀŝĚĞĚ ŝŶ ƚŚŝƐ ƌĞƉŽƌƚ ǁŝůů ďĞ ŽĨ ŐƌĞĂƚ ŚĞůƉ ƚŽ ƉůĂŶŶĞƌƐ͕ ŵĂŶĂŐĞƌƐ͕ ƐĞƌǀŝĐĞ ƉƌŽǀŝĚĞƌƐ͕ ĚĞĐŝƐŝŽŶͲŵĂŬĞƌƐ ĂŶĚ ƌĞƐĞĂƌĐŚĞƌƐ͕ ĂƐ ǁĞůů ĂƐ ƚĞĂĐŚĞƌƐ ĂŶĚ ƐƚƵĚĞŶƚƐ ŽĨ ƌĞůĞǀĂŶƚ ĨĂĐƵůƚŝĞƐ͘ /ƚ ƐĞĞŵƐ ŝŶĐƌĞĚŝďůĞ ƚŚĂƚ ƐĞƌǀŝĐĞ ĐŽǀĞƌĂŐĞ ŝŶ ŵĂŶLJ ƚŚĞŵĂƚŝĐ ĂƌĞĂƐ ŝƐ ŝŵƉƌŽǀŝŶŐ ĚĞƐƉŝƚĞ ƚŚĞ ĞĨĨĞĐƚƐ ŽĨ ƉŽůŝƚŝĐĂů ĂŶĚ ƐŽĐŝĂů ĐŚĂŶŐĞ͘ WĞƌĨŽƌŵĂŶĐĞ ŝŶ ĐŚŝůĚ ŚĞĂůƚŚ͕ ĨĂŵŝůLJ ŚĞĂůƚŚ͕ ĂŶĚ ĐŽŵŵƵŶŝƚLJ ƐƵƉƉŽƌƚĞĚ ƐĞƌǀŝĐĞƐ ƐĞĞŵƐ ƌĞĂƐŽŶĂďůLJ ƐĂƚŝƐĨĂĐƚŽƌLJ͘ dŚĞ ŝŶĨŽƌŵĂƚŝŽŶ ƉƌŽǀŝĚĞĚ ŝŶ ƚŚĞ ƌĞƉŽƌƚ ĐŽƵůĚ ďĞ ŽƉƚŝŵŝnjĞĚ ǁŝƚŚ ŝŵƉƌŽǀĞĚ ƵƚŝůŝnjĂƚŝŽŶ ŽĨ ƉůĂŶŶŝŶŐ͕ ƉƌŽŐƌĂŵŵŝŶŐ͕ ŵŽŶŝƚŽƌŝŶŐ ĂŶĚ ĞǀĂůƵĂƚŝŽŶ͘ / ǁŝƐŚ ƚŽ ĞdžƉƌĞƐƐ ŵLJ ƐŝŶĐĞƌĞ ŐƌĂƚŝƚƵĚĞ ƚŽ ƚŚĞ ƌĞƐƉĞĐƚĞĚ ^ĞĐƌĞƚĂƌLJ ŽĨ ,ĞĂůƚŚ ĂŶĚ WŽƉƵůĂƚŝŽŶ͕ ƌ͘ WƌĂǀĞĞŶ DŝƐŚƌĂ ĨŽƌ ƉƌŽǀŝĚŝŶŐ ƚŚĞ ƉƌĞĨĂĐĞ ƚŽ ƚŚĞ ƌĞƉŽƌƚ͘ 'ĞŶƵŝŶĞ ƚŚĂŶŬƐ ƚŽ ƌ͘ zĂƐŚŽǀĂƌĚŚĂŶ͘ WƌĂĚŚĂŶ͕ ŝƌĞĐƚŽƌ 'ĞŶĞƌĂů ŽĨ ƚŚĞ ĞƉĂƌƚŵĞŶƚ ŽĨ ,ĞĂůƚŚ ^ĞƌǀŝĐĞƐ͕ ĨŽƌ ŚŝƐ ƚŚŽƵŐŚƚĨƵů ŵĞƐƐĂŐĞ ĂŶĚ ƌĞŐƵůĂƌ ĚŝƌĞĐƚŝǀĞƐ ĂŶĚ ŐƵŝĚĂŶĐĞ͘ / ĂůƐŽ ĞdžƚĞŶĚ ŵLJ ƚŚĂŶŬƐ ƚŽ ƚŚĞ ŝƌĞĐƚŽƌƐ ŽĨ ƚŚĞ ŝǀŝƐŝŽŶƐ ĂŶĚ ĞŶƚĞƌƐ͕ ĂŶĚ ƚŽ ƚŚĞ ^ĞĐƚŝŽŶ ŚŝĞĨƐ ĨŽƌ ƐƵƉƉŽƌƚŝŶŐ ƵƐ ďLJ ƉƌŽǀŝĚŝŶŐ ƚŚĞŝƌ ĂŶĂůLJƚŝĐĂů ƌĞƉŽƌƚƐ͘ DLJ ĐŽůůĞĂŐƵĞƐ ŝŶ ƚŚĞ DĂŶĂŐĞŵĞŶƚ ŝǀŝƐŝŽŶ͕ ĞƐƉĞĐŝĂůůLJ Dƌ͘ WĂďĂŶ <ƵŵĂƌ 'ŚŝŵŝƌĞ ; ĞƉƵƚLJ ŝƌĞĐƚŽƌͿ͕ ƌ͘ >ŽŬ ZĂũ WĂŶĞƌƵ ;^DKͿ͕ Dƌ͘ ŝŶĞƐŚ ŚĂƉĂŐĂŝ ;^W, Ϳ͕ Dƌ͘ ŚƌƵďĂ ZĂũ 'ŚŝŵŝƌĞ ;^KͿ͕ Dƌ͘ WƵƐŚƉĂ >Ăů ^ŚƌĞƐƚŚĂ ; ĂƚĂ ŶĂůLJƐƚͿ͕ Dƌ͘ ĞĞƉĂŬ ĂŚĂů ;^KͿ͕ Dƌ͘ ^ƵƌLJĂ ĂŚĂĚƵƌ <ŚĂĚŬĂ ;^KͿ͕ Dƌ͘ 'ŽƉĂů ĚŚŝŬĂƌŝ ; KͿ͕ Dƌ͘ EĂǀƌĂũ ŚĂƚƚĂ ; KͿ͕ Dƌ͘ ĞĞƉĂŬ ŚĂŶĚĂƌŝ ; KͿ͕ Dƌ͘ WƌĂĚĞĞƉ WŽƵĚĞů ;D Θ ^ƉĞĐŝĂůŝƐƚͿ͕ Dƌ͘ ŵďŝŬĂ W͘ EĞƵƉĂŶĞ ;,D/^ ^ƵƉƉŽƌƚ KĨĨŝĐĞƌͿ ĂŶĚ ƚŚĞŝƌ ĂƐƐŝƐƚĂŶƚƐ ŝŶ ƚŚĞ DĂŶĂŐĞŵĞŶƚ /ŶĨŽƌŵĂƚŝŽŶ ^ĞĐƚŝŽŶ ĚĞƐĞƌǀĞ ƐƉĞĐŝĂů ĂƉƉƌĞĐŝĂƚŝŽŶ ĨŽƌ ƚŚĞŝƌ ŚĂƌĚ ĂŶĚ ƐŝŶĐĞƌĞ ǁŽƌŬ ĂŶĚ ƉĞƌƐŝƐƚĞŶƚ ĞĨĨŽƌƚƐ ƚŽ ƉƌŽĚƵĐĞ ƚŚŝƐ ŶŶƵĂů ZĞƉŽƌƚ ŽŶ ƐĐŚĞĚƵůĞ͘ / ĨĞĞů ŐƌĂƚĞĨƵů ƚŽ Ăůů ƚŚŽƐĞ ǁŚŽ ǁŽƌŬĞĚ ǁŝƚŚŽƵƚ ƌĞƐƚ Ăƚ ƌĞĐŽƌĚŝŶŐ͕ ƌĞƉŽƌƚŝŶŐ͕ ĐŽŵƉŝůŝŶŐ͕ ƉƌŽĐĞƐƐŝŶŐ ĂŶĚ ĂŶĂůLJnjŝŶŐ ƐĞƌǀŝĐĞ ĚĞůŝǀĞƌLJ ĂŶĚ ƉƌŽŐƌĞƐƐ ƌĞƉŽƌƚƐ ŽŶ ƚŝŵĞ͘ tŝƚŚŽƵƚ ƚŚĞŝƌ ĞĨĨŽƌƚƐ ƉƵďůŝĐĂƚŝŽŶ ŽĨ ƚŚŝƐ ƌĞƉŽƌƚ ǁŽƵůĚ ŶŽƚ ŚĂǀĞ ďĞĞŶ ƉŽƐƐŝďůĞ͘ / ƚĂŬĞ ƚŚŝƐ ŽƉƉŽƌƚƵŶŝƚLJ ƚŽ ŽĨĨĞƌ ŵLJ ƐŝŶĐĞƌĞ ĂƉƉƌĞĐŝĂƚŝŽŶ ƚŽ ƚŚĞ /E'KƐ͕ E'KƐ͕ DƵůƚŝůĂƚĞƌĂů ĂŶĚ ŝůĂƚĞƌĂů ĚĞǀĞůŽƉŵĞŶƚ ƉĂƌƚŶĞƌƐ ǁŚŽ ŚĂǀĞ ũŽŝŶĞĚ ƵƐ ŝŶ ƐĞƌǀŝĐĞ ĚĞůŝǀĞƌLJ ƉƌŽŐƌĂŵŵĞƐ͘ &ŝŶĂůůLJ͕ / ŚŽƉĞ ƚŚĂƚ ƚŚŝƐ ƌĞƉŽƌƚ ǁŝůů ďĞ ŽĨ ĞŶŽƌŵŽƵƐ ŚĞůƉ ŝŶ ƋƵŝĐŬůLJ ŝŵƉƌŽǀŝŶŐ ƚŚĞ ŚĞĂůƚŚ ƐĞƌǀŝĐĞƐ ŝŶ EĞƉĂů͘ / ĂůƐŽ ŚŽƉĞ ƚŚĞ ƌĞƉŽƌƚ ǁŝůů ƉƌŽǀŝĚĞ ǀĂůŝĚ ŝŶĨŽƌŵĂƚŝŽŶ ƚŽ Ăůů ƚŚŽƐĞ ǁŚŽ ǁŽƌŬ ƚŽ ƵƉůŝĨƚ ƚŚĞ ǁĞůĨĂƌĞ ŽĨ Ăůů EĞƉĂůĞƐĞ ĐŝƚŝnjĞŶƐ ƉĂƌƚŝĐƵůĂƌůLJ ƚŚĞ ƉŽŽƌ ĂŶĚ ǀƵůŶĞƌĂďůĞ͘ DĂƌĐŚ͕ ϮϬϭϮ
- 7. Executive Summary The Annual Report of Department of Health Services for the fiscal year 2067/68 (2010/2011) is the 17th consecutive report of its kind. This report analyses the performance of different programs over the preceding three fiscal years and also presents problems/constraints; actions taken against them and suggested actions for further improvement. This report is mainly based on the information collected by the Health Management Information System (HMIS) of DoHS from the health institutions across the country. The health institutions reporting to HMIS in this fiscal year include 95 public hospitals; 209 Primary Health Care Centers (PHCCs); 676 Health Posts (HPs); and 3,129 Sub Health Posts (SHPs). It also includes service coverage of 12,790 Primary Health Care/Outreach Clinics (PHC/ORC); 16,579 EPI Clinics and 48,680 Female Community Health Volunteers (FCHVs). A total of 445 NGO and 315 private health institutions have reported to HMIS. This implies that all 75 districts; 97.9 percent of public hospitals; 99.5 percent of HPCCs; 99.2 percent of HPs; 98.6 percent of SHPs; 86.4 percent of PHC outreach clinics; 92.9 percent of EPI clinics; 89.8 percent of FCHVs; 65.2 percent of NGO hospitals; and 69.2 percent of private hospitals have reported to HMIS in 2067/68 and overall 30.4 percent of the health facilities maintained timely reporting to HMIS. Complete and regular reporting particularly from non‐public health facilities have always been a challenge to HMIS. CHILD HEALTH IMMUNIZATION The national immunization coverage of all antigens in the regular NIP program in 2067/68 has improved compared to last fiscal years. However, the coverage is not uniform throughout the country. Thirty‐one districts (41%) have >90 percent coverage for all antigens. There has been 97 percent coverage for BCG, 95 percent for Polio‐3, 96 percent for DPT‐Hep B‐Hib 3, 88 percent for Measles and 41 percent for TT‐2 to pregnant women. BCG vs Measles dropout rate increased from 8.6 percent in 2066/67 to 9.8 percent in 2067/68. The vaccine wastage rate for DPT‐HepB‐Hib is 8.6 percent which is higher than the recommended wastage rate of five percent (single dose vial) and for OPV it is 23.4 percent which is higher than the recommended wastage rate of 15 percent. School Immunization programme has been continued. Two rounds of National Immunization Program and Intensified National Immunisation Days (NIDs) have substantially contributed towards the goal of eliminating polio. NUTRITION The growth monitoring services have been extended to children less than 5 years of age. There has been decrease in growth monitoring coverage by 7 percent from 46 percent in 2066/67 to 39 percent in 2067/68. The percent of under 5 years children among new growth monitored having malnourished status has decreased from 3.8 percent in last year to 3.4 percent this year. Two rounds of Vitamin A capsules were distributed to children aged 6 to 59 months. Almost two thirds (65%) of the pregnant women received Antihelmintic treatment and 73 percent received iron tablets. COMMUNITY BASED INTEGRATED MANAGEMENT OF CHILDHOOD ILLNESS (CB‐IMCI) AND NEWBORN CARE CB‐IMCI program has been implemented up to community level at all districts and it has shown positive results in management of childhood illnesses. There has been a substantial increment in the total number of infants of under 2 months who were treated at health facilities compared to last two years, an increment from 27,690 in 2065/66 to 33,751 in 2066/67 and to 48,669 this year. There has also been an increment in the number of cases treated for PSBI, LBI, Low weight and feeding problems. DoHS, Annual Report 2067/68 (2010/2011) i
- 8. Incidence of diarrhoea per 1,000 under‐five years children has decreased from 598 in FY 2066/67 to 500 in 2067/68. However cases of 'Severe Dehydration' has remained constant at 0.4 percent in two consecutive years. Treatment of diarrhoea by Zinc+ ORS has increased from 48 percent in 2066/67 to 88 percent in 2067/68. ARI cases per 1,000 under‐five population has decreased from 882 in 2066/67 to 824 in 2067/68 and incidence of Pneumonia (Pneumonia + Severe Pneumonia) per 1,000 <5 children decreased from 255/1,000 in 2066/67 to 246/1,000 in 2067/68. Similarly, the percentage of severe pneumonia has declined from 0.6 in 2065/66 to 0.5 in 2066/67 and 0.4 in 2067/68. The decline of severe pneumonia cases for three fiscal years is due to the early detection and proper management of ARI cases by health workers, VHW/MCHW and FCHVs and increased access to the free health services. The Government of Nepal, with the objective of reducing neonatal mortality, initiated Community Based Newborn Care Package (CBNCP) in 10 districts in 2065/55 and this was further expanded to additional 15 districts in 2067/68. FAMILY HEALTH FAMILY PLANNING The contraceptive prevalence rate (CPR) for modern family planning method is 44 percent and it is comparable with 2011 NDHS (43%). Central development region reported the highest level of CPR (51%) and western development region reported the lowest (32%). Given the CPR estimated from the HMIS and NDHS, achieving NHSP‐II goal of 67 percent by 2015 from the current level demands innovative approaches and appropriate strategies. However, there has been decline in Total Fertility Rate (TFR) from 3.1 in 2006 to 2.6 in 2011 (NDHS 2011) and is expected to meet the NHSP‐II target of 2.5 by 2015. In FY 2067/68 the share of spacing method of the total CPR was 41 percent which is lower than the estimation of 2011 NDHS data (47%). SAFE MOTHERHOOD Service statistics of the fiscal year 2067/68 shows that 85 percent of the mothers received first antenatal care services and less than three fifths of them made four visits indicating that more than two fifths of the mothers did not complete the recommended four ANC visits. Skilled birth attendance during delivery has increased from 31 percent in 2066/67 to 37 percent in 2067/68. NDHS 2011 has also shown 36 percent of deliveries attended by SBA. Service statistics of the fiscal year 2067/68 shows that 37 percent of the mothers delivered in health facilities, this is close to the findings of NDHS 2011 (35%). There has been a slight increase in the percentage of mothers who received postnatal care at the health facility compared to last fiscal year. The SMNH long term plan (2006‐2017) has a target of providing CEOC services in 60 districts; 80 percent of PHCCs providing BEOC services; and 70 percent of Health Posts providing delivery services by 2017. In 2067/68 comprehensive emergency obstetric care services were provided from 99 public and private hospitals in 43 districts. Out of 99 CEOC sites, 37 were public hospitals, 14 medical colleges and 48 were private/NGO hospitals. EOC monitoring data received from 44 districts in the year 2067/68 shows that about one fifth of the births took place in B/CEOC facilities. A total of 192 providers including 74 nurses have been trained on safe abortion services (SAS) and 95,306 women received safe abortion services from 487 listed sites. There has been a significant improvement in the number of facilities providing delivery service; number of institutional delivery; and SBA during delivery after the launch of Aama Surakchhya program. Almost nine in every ten (89%) of the mothers who delivered in health facility have DoHS, Annual Report 2067/68 (2010/2011) ii
- 9. received transportation incentive. There has been a substantial increase in the budget allocation for Aama Surakchhya Program and also increase in absorption capacity of the DoHS over the last couple of years. FEMALE COMMUNITY HEALTH VOLUNTEERS The major role of the Female Community Health Volunteers (FCHVs) is promotion of safe motherhood, child health, family planning, and other community based health services to promote health and healthy behaviour of mothers and community people with support from health workers and health facilities. At present there are 48,680 FCHVs actively working all over the country. FCHVs have contributed in distribution of 49 percent oral pills and 50 percent ORS packets at the national level. FCHVs distributed a total of 6,905,532 packets of condoms in the FY 2067/68. Service statistics of this shows that more than one half (55%) of the diarrhoea and ARI cases were treated by FCHVs. FCHVs contributed significantly in the distribution of oral contraceptive Pills, Condoms and Oral Rehydration Solution (ORS) packets and counselling and referring to mothers in the health facilities for the service utilization. PRIMARY HEALTH CARE OUTREACH CLINIC (PHC/ORC) Primary Health Care Outreach Clinics (PHC/ORC) are basically the extension of basic health services at the community level. Eighty‐six percent of the targeted 153,480 PHC/ORC were conducted in 2067/68 and this was five percent more than the previous year. On an average 21 clients were served per clinic per month during 2067/68, compared to 20 clients in 2066/67. DISEASE CONTROL MALARIA A total of 160,868 blood smears were collected against the target of collecting 150,000. However, only 66.3 percent (106,598) of collected blood smears could be examined. The Annual Blood Slide Examination Rate (ABER) decreased from 0.75 percent in 2065/66 to 0.66 percent in 2066/67 and remained same in 2067/68 where as Annual Parasite Incidence (API) increased from 0.14 per 1,000 in 2066/67 to 0.16 in 2067/68. Proportion of P.Falciparum (PF) decreased by around 5 percent, from 20.5 percent in 2066/67 to 15.7 in 2067/68. The data has revealed that imported malaria cases are remarkably high in number indicating need of more attention for cross border monitoring and surveillance of malaria. Like previous years, two rounds of Indoor Residual Spraying were carried out this year in 15 districts that protected 716,572 people. KALA‐AZAR Kala‐azar is a major problem in 12 districts of eastern and central Terai. Incidence of Kala‐azar has decreased from 1.71 per 10,000 areas at risk population in 2065/66 to 1.33 in 2066/67 and to 0.94 in 2067/68 (excluding foreign cases). Out of the 12 districts five districts have an incidence of more than 1, while 7 districts have an incidence of less than 1 case per 10,000 areas at‐risk population. A total of 806 Kala‐azar cases were recorded and of them 802 (99.5%) improved after the treatment while 4 patients (0.5%) died in 2067/68. LYMPHATIC FILARIASIS (LF) Lymphatic Filariasis is a public health problem and main cause of morbidity, primarily, lymphoedema of legs and hydrocele in many endemic areas of the rural and slum areas of the country. The government had initiated implementation of Mass Drug Administration (MDA) in Parsa district in 2003. Since then the program has expanded gradually in other endemic districts as well. MDA has DoHS, Annual Report 2067/68 (2010/2011) iii
- 10. stopped in 5 districts (Parsa, Makawanpur, Chitwan, Nawalparasi, Rupandehi) in fiscal year 2067/68 after completion of 5 rounds of MDA. DENGUE Dengue outbreak in 2006 had shown its face with 32 confirmed dengue cases followed by 27 cases in 2007, 10 cases in 2008, 30 cases in 2009 and 917 cases in 2010 with major outbreak in Chitwan and Rupandehi districts. In the fiscal year 2067/68 different districts showed dengue endemicity as reported in previous years. TUBERCULOSIS Tuberculosis is a major public health problem in Nepal. Treatment by Directly Observed Treatment Short course (DOTS) have been implemented in all 75 district of the country and TB patients are being treated with DOTS at 1,118 treatment centers and 3,103 sub centers. The Treatment Success Rate (TSR) stands at 90 percent and Case Finding Rate (CFR) at 73 percent. LEPROSY Leprosy is in declining phase, however, this decline is not enough to reach the goal of elimination. The new case detection rate has declined from 1.99/10,000 population in 2065/66 to 1.15/10,000 in 2066/67 and to 1.12/10,000 population in 2067/68. A total of 3,142 new leprosy cases were detected and 5,362 cases received treatment with MDT and 2,979 cases completed treatment and were made RFT. Among the registered MB cases 2,174 (94.4%) and 2,286 (96.9%) PB has completed treatment within the given time frame. HIV/AIDS AND STI HIV in Nepal is characterized as concentrated epidemic, where majority of infections are transmitted through sexual transmission. Prevention of HIV among key population is the key programmatic strategies, while providing quality treatment, care and support for infected and affected is equally important strategic directions to achieve the end results of national response. Since the detection of the first AIDS case in 1988, the HIV epidemic in Nepal has evolved from a low prevalence to concentrated epidemic. As of 2011, national estimates indicate that approximately 55,600 adults and children are infected with the HIV virus in Nepal. A total of 18,396 cases of HIV out of them 7,437 advanced HIV infection cases had been reported as of Asar 2068. The estimated prevalence of HIV in the adult population is 0.33 percent. SUPPORTING PROGRAMS HEALTH TRAINING National Health Training Centre has a network of 5 Regional Health Training Centres, one Sub Regional Health Training Centre, district level training facilities in 30 districts and 14 Training Health Posts in appropriate district sites. A team of 5‐7 district training team provide training to the concerned health workers. Clinical competency based training are provided through 19 clinical training sites attached to regional and zonal hospitals. Various EDP’s are providing collaborative support to National Health Training Centre in planning and execution of training programs. NHTC have able to meet 90 percent of the targeted SBA training in 2067/68 and this has contributed in filling the gap of required number of SBA service providers in the country. NHTC also conducted basic, in‐service, refresher, up‐grading training along with clinical, non‐clinical and other management training. HEALTH EDUCATION, INFORMATION AND COMMUNICATION Health Education, Information and Communication Centre (NHEICC) is responsible for developing, producing and disseminating messages to promote and support health programs and services in an DoHS, Annual Report 2067/68 (2010/2011) iv
- 11. integrated manner. The health education and communication units in the district Health Offices implement IEC activities utilizing various media and methods according to the needs of the local people in the district. Local media and languages are used in the district for dissemination of health messages. The main activities include health education programmes in the schools and community; print materials production and distribution; production and dissemination of regular, weekly and periodic radio, television and FM radio programs; publication and dissemination of health messages through newspapers, social mobilisation, advocacy, workshop/seminar, folk events, observation on special days and exhibitions. LOGISTICS MANAGEMENT The major function of Logistic Management Division (LMD) is to procure, store and distribute health commodities for the government health facilities. It also involves repair and maintenance of bio‐ medical equipments, instruments and the transportation vehicles. LMD has been implementing and monitoring Pull System for contraceptives, vaccines and essential drugs in the districts. Rural Telemedicine Program has been implemented in 25 hill and mountain districts. HEALTH LABORATORY SERVICES National Public Health Laboratory (NPHL) is a nodal institute for developing policy, guidelines and overall framework for capacity building in laboratory sector. Attention has been given in strengthening laboratory procedure and communication between national, regional and district levels and in strengthening the system ensuring the availability of essential equipment, logistics and human resources. At present there are eight central hospital based laboratories, three regional hospital based laboratories, two sub regional hospital based laboratories, 11 zonal hospital based laboratories, 66 district hospital based laboratories, and 204 PHCC based laboratories in the country. In the private sector there are above 1,300 laboratories. NPHL is also conducting the laboratory surveillance activities on various disease pathogens such as Measles/Rubella surveillance, Japanese encephalitis surveillance, Influenza surveillance and Antimicrobial resistance surveillance. PRIMARY HEALTH CARE REVITALIZATION Primary Health Care Revitalization Division (PHCRD) works towards reducing poverty by providing equal opportunity for all to receive quality and affordable health care services. This division is envisaged to revitalize PHC in Nepal by addressing emerging health challenges in close collaboration with other DoHS divisions and relevant actors. In 2067/68 monitoring committees were developed at all levels of health system; citizen charter were displayed in most of health facilities on EHCSs; trainings were conducted on rational drug prescription in 75 districts; integrated public health campaigns were organized in 8 districts and Peers Group discussion were conducted for rational use of drugs in 22 districts. PHCRD also provided transportation cost for marginalized community and senior citizen. Community Health Insurance piloting activities is continued in 8 PHCCs. PERSONNEL ADMINISTRATIVE MANAGEMENT The administrative section under the Department of Health Services (DoHS) manages to distribute the health work force to deliver health services in the country. Altogether 27,300 employees are recorded under MoHP of which 21,000 are technical and 6,300 persons are administrative. Under the transfer policy DoHS manages transfer and posting of staff up to 7th level. There is a strong need of improving personnel record keeping and defining employee’s roles and responsibilities. FINANCIAL MANAGEMENT Out of total national budget of Rs. 297,818,882,000 a sum of Rs. 23,813,993,000 (8.0%) was allocated for the health sector in 2067/68 (2010/2011). Of the total health sector budget, Rs. DoHS, Annual Report 2067/68 (2010/2011) v
- 12. 15,035,390,000 (63.1%) was allocated for execution of programs under the Department of Health Services. Of this Rs. 13,635,303,000 (90.7%) was allocated to recurrent and Rs. 1,400,087,000 (9.3%) was allocated to capital budget. The EDPs contribution comprised 48.4 percent of the total budget under DoHS. PLANNING, MONITORING, SUPERVISION AND INFORMATION MANAGEMENT As in the previous years Management Information System (MIS) Section continued providing trimester reporting to all Divisions, Centres, Regional Directorates and District Health/Public Health Offices. Annual Performance Review workshops were conducted at district, regional and national levels. Management Division also conducted several training activities on oral health, nursing leadership and management, quality assurance to improve skills of heath workers. Some health facilities were upgraded to higher level. It continued implementation of Health Sector Information System (HSIS) in three districts: Llitpur, Parsa and Rupandehi. Other Programs DRUG ADMINISTRATION As in the previous years the Department of Drug Administration conducted a number of activities to raise awareness on the rationale use of medicines through different media; audited drug industries for good manufacturing practices; checked quality of marketed drugs; and drafted good manufacturing practice regulation and revised national medicine policy and national list of essential medicines. AYURVEDA A total of 784,822 people received health care services from Aurveda health facilities in 2067/68. The highest number of people were served in western region (219,195) where as the least number of people were served in far western region (87,048). DoHS, Annual Report 2067/68 (2010/2011) vi
- 14. INDICATORS MALARIA / KALA‐AZAR Annual Blood Slide Examination Rate (ABER) per 100 Annual Parasite Incidence (API) per 1,000 Proportion P.falciparum (PF %) Clinical Malaria Incidence (CMI)/1000 Incidence of Kala‐azar /10,000 Risk Population TUBERCULOSIS Treatment Success Rate on DOTS Sputum Conversion Rate LEPROSY New Case Detection Rate (NCDR) /10,000 Prevalence Rate (PR) /10,000 Disability rate Grade 2 among new cases HIV/AIDS AND STI Estimated HIV cases Cumulative HIV reported cases CURATIVE SERVICES Total OPD new visits Total OPD new visits as % of total population 2065/66 2066/67 2067/68 (2008/2009) (2009/2010) (2010/2011) 0.75 0.68 0.66 0.18 0.15 0.16 22.18 20.48 15.71 5.72 5.41 4.10 1.33 0.95 0.75 89 90 90 89 89 89 1.66 1.15 1.12 1.09 0.77 0.79 3.90 2.72 3.50 70,000 70,000 56,000 14,787 16,138 18,396 18,947,923 20,894,118 19,708,800 69.19 75.98 70.39 Note= * Unadjusted Source: NTC, LCD, NCASC, EDCD and HMIS/DoHS DoHS, Annual Report 2067/68 (2010/2011) viii
- 15. Table of Contents Executive Summary .................................................................................................................................. i Table of Contents ................................................................................................................................... ix Acronyms ............................................................................................................................................... xi INTRODUCTION ....................................................................................................................................... 1 1.1 BACKGROUND ........................................................................................................................... 1 1.2 DEPARTMENT OF HEALTH SERVICES (DoHS) .................................................................................. 2 1.3 SOURCES OF INFORMATION ......................................................................................................... 5 1.4 STRUCTURE OF THE REPORT ........................................................................................................ 7 CHILD HEALTH ......................................................................................................................................... 9 2.1 IMMUNIZATION ......................................................................................................................... 9 2.2 NUTRITION ............................................................................................................................. 22 2.3 COMMUNITY BASED INTEGRATED MANAGEMENT OF CHILDHOOD ILLNESSES (CB‐IMCI) AND NEWBORN CARE...................................................................................................................... 35 FAMILY HEALTH..................................................................................................................................... 50 3.1 FAMILY PLANNING ................................................................................................................... 50 3.2 SAFE MOTHERHOOD AND NEWBORN HEALTH ............................................................................. 61 . 3.3 FCHV PROGRAM .................................................................................................................... 75 . 3.4 PRIMARY HEALTH CARE OUTREACH ............................................................................................ 79 3.5 DEMOGRAPHY AND REPRODUCTIVE HEALTH RESEARCH ................................................................. 82 3.6 ADOLESCENT SEXUAL AND REPRODUCTIVE HEALTH ....................................................................... 86 DISEASE CONTROL ................................................................................................................................ 90 4.1 MALARIA ............................................................................................................................... 90 . 4.2 KALA‐AZAR ............................................................................................................................ 97 4.3 LYMPHATIC FILARIASIS ............................................................................................................ 102 4.4 DENGUE .............................................................................................................................. 105 . 4.5 TUBERCULOSIS ...................................................................................................................... 108 4.6 LEPROSY............................................................................................................................... 121 4.7 HIV/AIDS AND STI ................................................................................................................. 132 CURATIVE SERVICES ............................................................................................................................ 143 5.1 BACKGROUND ....................................................................................................................... 143 5.2 ANALYSIS OF ACHIEVEMENTS .................................................................................................... 144 SUPPORTING PROGRAMS ................................................................................................................... 153 6.1 HEALTH TRAINING ................................................................................................................. 153 6.2 HEALTH EDUCATION, INFORMATION AND COMMUNICATION ........................................................ 162 6.3 LOGISTICS MANAGEMENT ....................................................................................................... 166 6.4 PUBLIC HEALTH LABORATORY SERVICES..................................................................................... 177 6.5 PERSONNEL ADMINISTRATION MANAGEMENT ........................................................................... 184 6.6 FINANCIAL MANAGEMENT ...................................................................................................... 187 6.7 MANAGEMENT ..................................................................................................................... 194 6.8 PRIMARY HEALTH CARE REVITALIZATION ................................................................................... 199 DoHS, Annual Report 2067/68 (2010/2011) ix
- 16. OTHER PROGRAMS ............................................................................................................................. 203 7.1 DRUG ADMINISTRATION ......................................................................................................... 203 7.2 AYURVEDA ........................................................................................................................... 207 DEVELOPMENT PARTNERS ................................................................................................................ 212 8.1 MULTILATERAL ORGANIZATIONS .............................................................................................. 213 8.2 BILATERAL ORGANIZATIONS .................................................................................................... 214 8.3 INTERNATIONAL NON GOVERNMENT ORGANIZATIONS (INGOs) ................................................... 215 8.4 NON GOVERNMENTAL ORGANIZATIONS .................................................................................... 221 REFERENCES ........................................................................................................................................ 222 ANNEXES ANNEX 1: ACTIVITIES CARRIED OUT IN FY 2067/68 ........................................................................... 224 ANNEX 2: HEALTH INDICATORS ......................................................................................................... 236 ANNEX 3: HEALTH SERVICES .............................................................................................................. 243 DoHS, Annual Report 2067/68 (2010/2011) x
- 23. Chapter 1 1.1 INTRODUCTION BACKGROUND The Annual Report of Department of Health Services for the fiscal year 2067/68 (2010/2011) is the 17th consecutive report of its kind. This report analyses the performance and achievements of Department of Health Services (DoHS) in the fiscal year 2067/68 (2010/11). It mainly deals with the program specific policies, goal, objectives, strategies, major activities and achievement. It also presents the problems/issues/constraints raised by different wings of DoHS and stakeholders and recommendation for actions to be taken in order to improve performance and targets for the next fiscal year. In addition, this report also provides information on contributions from other departments, partners and stakeholders, contemporary issues in the health sector as well as progress status of major programs implemented through DoHS, RHDs, D/PHOs and health institutions under DoHS. Preparation of this report followed the Regional Annual Performance Review Meetings conducted in all five development regions which culminated in the National Annual Performance Review Meeting. These review meetings were attended by the Regional Directorates, Divisions of DoHS, Centres, Central hospitals, and representatives from External Development Partners and NGOs/INGOs at each level. During the workshop, policy statements of each program were reviewed in the light of the present context and analysed to an extent. The data generated from the HMIS in the form of raw numbers, were carefully and critically analysed utilising the selected indicators along with data available from other sources. These data were interpreted during the presentations and discussions. The National Annual Performance Review Meeting achieved the following objectives: Reviewed the status of achievement against target set for the FY 2067/68 (2010/2011) by Divisions/Centres/Sections of DoHS with respect to released budget and expenditure. Compared trend of service coverage of the FY 2067/68 with previous two successive fiscal years and analyze the fact. Reviewed the status of implementation of recommendation made by the previous National Annual Performance Review Meting. Identified management issues/problems/constraints in implementing the program and suggested recommendations and specific strategy and actions plans to address those issues. Facilitated the process of generating specific strategies for low coverage Region and Districts to boost up their coverage and moderating on specific action plan to scale up the level of achievement and highlight the best performing Region & districts to be replicated to achieve most advantageous results. Interaction among Region/Department of Health Services/Ministry of Health and Population and External Development Partners (EDPs). The outcome of this workshop can be seen in the program specific chapters of this Annual Report. Detailed district‐specific raw data and analysed data are available in each of the five Regional Reports as well as in Annex 3 of this document. DoHS, Annual Report 2067/68 (2010/2011) 1
- 24. 1.2 DEPARTMENT OF HEALTH SERVICES (DoHS) Ministry of Health and Population has been delivering preventive, curative, promotional and rehabilitative health care services and other health system related functions such as policy and planning, human resource development and mobilisation, financing and financial management, and monitoring and evaluation. It has six Divisions: Administration Division, Policy, Planning and International Cooperation Division, Curative Services Division, Human Resources and Financial Management Division, Public Health Administration and Monitoring and Evaluation Division, and Population Division. There are five autonomous bodies established by law for education, research and service delivery purposes. In addition to these, there are four professional councils to provide accreditation to health‐related schools/ training centres and to regulate care providers. There are three Departments under the MoHP: Department of Health Services (DoHS), Department of Ayurved (DoA) and Department of Drug Administration (DDA). The DoHS and other departments are responsible for formulating programs as per policy and plans, implementation, use of appropriate financial resources and accountability, and monitoring and evaluation. DDA is the regulatory authority for assuring the quality and regulating the import, export, production, sale and distribution of drugs. Department of Auyurveda offer Aurvedic care to the people and also implement health promotional activities. Department of Health Services (DoHS) is responsible for delivering preventive, promotive and curative health services throughout Nepal. Director General (DG) is the organisational head of the DoHS. The recent reorganisation of the DoHS includes six Divisions: Management Division with infrastructure, planning, quality of care and management information system; Family Health Division with the responsibility of reproductive health care, including safe motherhood and neonatal health, family planning and Female Community Health Volunteers (FCHVs); Child Health Division covering nutrition, IMCI, and EPI; Epidemiology and Disease Control Division wit the responsibility of controlling epidemics, Pandemic and endemic diseases as well as treatment of animal bites; Logistics Management Division covers procurement, supplies and management of logistics, equipments and services required by DoHS and below levels; and newly formed Primary Health Care Revitalization Division with the responsibility of carrying out activities for primary health care. Key functions of DoHS include: • Provide GoN with necessary technical advice in formulating health related policies, develop and expand health institutions established in line with these policies; • Determine requirement of manpower for health institutions and develop such manpower by preparing short and long term plans; • Manage procurement and supply of drugs, equipment, instruments and other logistics at regional, district and below levels; • Co‐ordinate the activities and mobilize resources in the implementation of approved programs; • Manage the immediate solution of problems arising from natural disasters and epidemics; • Establish relationships with foreign countries and international institutions with the objective of enhancing effectiveness and developing health services and assist the Ministry of Health and Population in receiving and mobilizing foreign resources by clearly identifying the area of cooperation; • Create a conducive atmosphere to encourage the private sector, non‐governmental organizations and foreign institutions to participate in health services, maintain relation and coordination, control quality of health services by regular supervision and monitoring; DoHS, Annual Report 2067/68 (2010/2011) 2
- 25. • • Systematically maintain data, statements and information regarding health services, update and publish them as required; Human resource management and development as per rules and regulations and assigned authority; and Financial management of DoHS, RHDs, D/PHOs and settlement of irregularities. • There are five Centres with a degree of autonomy in personnel and financial management: National Health Training Centre (NHTC), National Health Education, Information and Communication Centre (NHEICC), National Tuberculosis Control Centre (NTC), National Centre for AIDS and STD Control (NCASC) and National Public Health Laboratory (NPHL). The NHTC coordinates all training programs of the respective Divisions and implements training by sharing common inputs and reducing the travelling time of care providers. Similarly, all IEC/BCC‐related activities are coordinated by NHIECC. These centres support the delivery of EHCS and work in close coordination with the respective Divisions. At the regional level there are five Regional Health Directorates (RHDs) providing technical backstopping as well as program supervision to the districts. The RHDs are directly under the MoHP. There are regional and zonal hospitals (15), which have been given decentralised authority through the formation of Hospital Development Boards. In addition, there are training centres, laboratories, TB centres (in some regions) and medical stores at the regional level. At the district level, the structure varies between districts. Sixty‐one districts are managed by the District Health Office (DHO) with support of the District Public Health Office (DPHO), whereas the remaining 14 are managed solely by the DPHO. The DPHOs and DHOs are responsible for implementing essential health care services (EHCS) and monitor activities and outputs of District Hospitals, Primary Health Care Centres (PHCCs), Health Posts (HPs) and Sub Health Posts (SHPs). The service delivery outlets in the country include 3,129 SHPs, 676 HPs, 209 PHCCs, 65 district hospitals, 10 zonal hospitals, 2 sub regional hospitals, 3 regional hospitals, and 8 central level hospitals. A sub‐health post is the first institutional contact point for basic health services. SHPs monitor the activities of FCHVs as well as community‐based activities by PHC outreach clinics and EPI clinics. The health post offers the same package of essential health care services plus birthing centres in the respective VDC and monitors the activities of the SHPs in their geographical area as well. However, a SHP also functions as the referral centre of the volunteer cadres of female community health volunteers (FCHVs) as well as a venue for community‐based activities such as PHC outreach clinics and EPI clinics. Each level above the SHP is a referral point in a network from SHP to Health Post (HP) to Primary Health Care Centre (PHCC), on to district, zonal and regional hospitals, and finally to tertiary level hospitals. This referral hierarchy has been designed to ensure that the majority of population receive public health and minor treatment in places accessible to them and at a price they can afford. Inversely, the system works as a supporting mechanism for lower levels by providing logistical, financial, supervisory, and technical support from the centre to the periphery. DoHS, Annual Report 2067/68 (2010/2011) 3
- 26. Fig. 1.2: Organogram of Department of Health Services (DoHS) DEPARTMENT OF HEALTH SERVICES CENTRE FCHV 48680 CENTRAL HOSPITALS ‐8 ZONAL HOSPITAL ‐ 10 DISTRICT HOSPITAL ‐ 65 REGIONAL TB CENTRE ‐ 5 REGIONAL MEDICAL STORE ‐ 5 DISTRICT PUBLIC HEALTH OFFICE ‐ 15 REGIONAL TRAINING CENTRE ‐5 SUB‐REGIONAL HOSPITAL ‐ 2 REGIONAL HOSPITAL ‐ 3 REGIONAL HEALTH DIRECTORATE ‐ 5 NTC PHCRD EDCD LCD CHD MD LMD FHD DIVISION NHEICC NPHL NHTC NCSAC MINISTRY OF HEALTH AND POPULATION DISTRICT HEALTH OFFICE ‐ 60 PRIMARY HEALTH CARE CENTRE/HEALTH CENTRE ‐ 209 HEALTH POST ‐ 676 SUB‐HEALTH POST ‐ 3129 PHC/ORC CLINIC 12790 EPI OUTREACH CLINIC 16579 DoHS, Annual Report 2067/68 (2010/2011) 4
- 27. 1.3 SOURCES OF INFORMATION Sources of health sector information in Nepal include management information systems (MIS), disease surveillance, vital registration, census, sentinel reporting, surveys, rapid assessments, and research (Figure 1.3). The MIS within the health sector include the Health Management Information System (HMIS); Logistical Management Information System (LMIS); Financial Management Information System (FMIS); Health Infrastructure Information System (HIIS); Planning and Management of Assets in Health Care System (PLAMAHS); Human Resource Information System (HuRIS); Training Information Management System (TIMS); Aayurveda Reporting System (ARS); and Drug Information Network (DIN). The Health Sector Information System (HSIS), being piloted in three districts (Rupandehi, Parsa and Lalitpur) proposes to integrate all of the MIS. Fig. 1.2: Sources of Health Sector Information in Nepal H e a l t h S e c t o r I n f o r m a t io n S y s t e m H M IS L M IS F M IS H I IS H u R IS T IM S ARS H e a lth M anagem ent In fo r m a t io n S y s te m L o g is tic a l M anagem ent In fo r m a t io n S y s te m F in a n c ia l M anagem ent In f o r m a tio n S y s te m H e a lth I n fr a s tr u c t u r e In f o r m a tio n S y s te m H um an R e s o u rc e In f o r m a tio n S y s te m T r a in in g In fo r m a t io n M anagem ent S y s te m A a y u rv e d a R e p o r tin g S y s te m PLAM AH S P la n n in g & M anagem ent o f A s s e ts in H e a lth C a re S y s te m D IN D ru g In fo r m a t io n N e tw o rk R o u tin e H e a lth In fo rm a tio n S y s te m s C O M P R E H E N S IV E H E A L T H S E C T O R IN F O R M A T IO N S Y S T E M D i s e a s e S u r v e i l la n c e V i t a l R e g is t r a t i o n P o p u la t i o n B a s e d I n f o r m a t i o n • • • • • C ensus S e n t i n e l R e p o r t in g S u rv e y s R a p id A s s e s s m e n t s R e s e a rc h National Health Policy (NHP) 1991 and Second Long Term Health Plan (SLTHP) 1997 – 2017, recognized the need for a comprehensive health sector information system (HSIS) to achieve the health sector’s objectives. The Health Sector Strategy: An Agenda for Change, 2002, therefore, proposed the establishment of HSIS, and this was one of the primary objectives for the NHSP‐IP 2004‐2009. The HSIS National Strategy was developed in 2005 with the following aims: 1. Develop an integrated information system An integrated system simply refers to all MIS utilizing a uniform coding system, thus enabling data from different systems to be linked, and for all MIS to feed in to a District Health Information Bank (DHIB). 2. To provide comprehensive information from all health facilities HSIS aims to collect data from public health facilities, private health facilities, and NGO run health facilities. 3. To generate disaggregated information HSIS aims to produce data disaggregated by caste/ethnicity and geography. 4. To generate data at all levels DoHS, Annual Report 2067/68 (2010/2011) 5
- 28. HSIS aims to generate data at all levels (facility, ilaka, district and central). 5. To establish a District Health Information Bank (DHIB) 5. To exploit modern technologies including GIS. The Health Management Information System (HMIS) is based in the MIS Section in the Management Division, Department of Health Services (DoHS) and has been in operation since 1994. It includes information relating to the provision of health services, health status and program performance. The HMIS data is monthly compiled, reported, and reviewed at Ilaka, district, regional and national level. Data Collection and Reporting Process within HMIS FCHVs are volunteers who provide services at the community level, and maintain a pictorial HMIS 27 FCHV register. Each month they are visited by the VHW or MCHW (to re‐supply family planning commodities and other drugs) who collects the register. The VHWs/MCHWs submit a HMIS 31 VHW/MCHW Reporting Form monthly to their assigned health facility (either a sub‐health, health post or PHCC). This collates data from the FCHV registers and their outreach services. Sub‐health post and non‐ilaka health posts compile a HMIS 32 PHC/HP/SHP Reporting Form and submit it on a monthly basis to the ilaka health post or ilaka PHCC. This also collates data for its own coverage including VHW / MCHW reporting forms and FCHVs registers. The Ilaka HP and PHCCs compile a HMIS 32 PHC/HP/SHP Reporting Form and submit it on a monthly basis to the District/Public Health Office (D/PHO). This collates data from the facility, any SHPs and non‐Ilaka HPs under that facility. District, Zonal, Sub‐regional, Regional and National level hospitals and including ‘Other public’ and non‐public hospitals submit HMIS 34 Hospital Based Reporting Form to the D/PHO every month. Some hospitals enter data electronically, but as there is no uniform system developed for this, databases vary. However, in reality most of the higher level hospitals submit reports directly to the HMIS Section and a large number of non‐public hospitals reports are not covered to HMIS till date. D/PHO compiles all the reports received from health facilities and submits the HMIS 33 District Reporting Form to the Regional Health Directorate and the MIS Section, Management Division, DoHS each month. Regional Health Directorates monitor and supervise district public health programs; ensure timely reporting from D/PHOs and hospitals to the centre; participate in district and other reviews and perform regional review based on analyzed data received from the centre. MIS Section at the central level enters the monthly reports received from the D/PHOs and hospitals into an electronic HMIS database that can be accessed via the internet and LAN. The internet access is restricted and needs a password to access the HMIS data. The MIS Section provides monthly compiled data to all program divisions and centres, RHDs and D/PHOs through online access for planning and monitoring purposes. DoHS, Annual Report 2067/68 (2010/2011) 6
- 29. Fig. 1.2: Information flow in HMIS DEPARTMENT OF HEALTH SERVICES Management Information Section DPHO Regional Health Directorate HMIS 33a District Reporting Form (DPHO) Regional / Zonal Hospitals HMIS 34 Hospital Based Reporting Form (Medical Recorder) District Hospitals HMIS 34 Hospital Based Reporting Form (Medical Recorder) Ilaka HP / PHC HMIS 32 PHC/HP/SHP Reporting Form ( SAHW or HA) Sub HP / Non -Ilaka HP HMIS 32 PHC/HP/SHP Reporting Form (AHW,VHW, or MCHW) VHW / MCHW HMIS 31 VHW / MCHW Reporting Form FCHV HMIS 27 FCHV Register 1.4 STRUCTURE OF THE REPORT This report has 8 chapters. Chapter 1, this chapter, briefly presented the background to the practice of annual report preparation, organogram of the DoHS, and sources of information in health sector in Nepal. Chapter two to six cover the different programs within the DoHS; chapter seven presents' programs of other departments within the Ministry of Health and Population; and chapter eight presents a brief summary of development partners contributing to health sector in Nepal. Chapter two to seven contain five sections in each chapter: Section one gives a brief background to the program; section two presents major activities within the program; section three analyses the achievements of the program in the last three years; section four presents problems/constrains of the program as discussed in the regional and national reviews; and the last section presents targets for the next fiscal year. Annex one presents the target vs. achievement of the activities carried out in the last fiscal year by different programs; Annex two lists the HMIS Indicators used to monitor different programs; and Annex three provides the raw and analyzed data of different programs disaggregated by ecological regions and districts. DoHS, Annual Report 2067/68 (2010/2011) 7
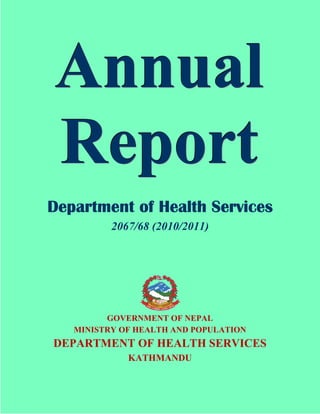
- 30. Measles Vaccination and Coverage Fiscal Year 2067/68 (2010/2011) No. of infants immunized Kath man d u Jh ap a Mo ran g Ru p an d eh i Dh an u sh a Sarlah i Sirah a Rau tah at Bara Su n sari Mah o ttari Kailali Sap tari Dan g Kap ilvastu Naw alp arasi Parsa Ch itw an Ban ke Kaski Kan ch an p u r Su rkh et Makaw an p u r Dh ad in g L alitp u r Bard iya Kavre Ach h am Dailekh Ud ayp u r G u lmi Pyu th an Syan g ja T an ah u Ilam Bag lu n g Ro lp a Baitad i Salyan Do ti Sin d h u li Sin d h u p alch o w k Nu w ako t Palp a Ru ku m G o rkh a Jajarko t Bajh an g Bh aktap u r Arg h akh an ch i Pan ch th ar Kh o tan g Do lkh a Ramech h ap L amju n g Bh o jp u r Baju ra Dad eld h u ra Dh an ku ta San kh u w asab h a Kaliko t Darch u la T ap leju n g Parb at O kh ald h u n g a Myag d i Ju mla So lu kh u mb u T eh arth u m Hu mla Mu g u Rasu w a Do lp a Mu stan g Man an g 25,952 Jajarko t 24,648 Baju ra 21,011 Ach h am 19,669 Pyu th an 17,232 Mu g u 16,969 Rau tah at 16,626 Dailekh 16,241 Mah o ttari 15,924 Sirah a 15,760 Jh ap a 15,175 Kaliko t 15,125 Bajh an g 14,107 Bara 13,042 Ro lp a 12,979 Ju mla 12,683 Dad eld h u ra 11,472 Sarlah i 9,658 Dh an u sh a 9,552 Do ti 9,223 Kap ilvastu Salyan 8,738 8,401 Do lp a 8,293 Ru ku m Su rkh et 8,054 8,016 Ru p an d eh i 7,967 Sap tari Darch u la 7,928 7,634 Dan g 7,007 Baitad i Hu mla 7,000 Kath man d u 6,967 6,849 Ud ayp u r 6,516 Rasu w a 6,366 Dh ad in g 6,266 Parsa G u lmi 6,163 T ap leju n g 6,077 Ban ke 5,953 Myag d i 5,898 Su n sari 5,725 Mo ran g 5,675 5,525 Pan ch th ar 5,449 Arg h akh an ch i So lu kh u mb u 5,443 San kh u w asab h a 5,322 Kailali 5,227 Do lkh a 5,081 Bag lu n g 4,764 L amju n g 4,739 Kaski 4,661 Naw alp arasi 4,476 Kan ch an p u r 4,144 Makaw an p u r 4,117 Sin d h u li 3,888 Ilam 3,807 Syan g ja 3,775 Ramech h ap 3,702 Dh an ku ta 3,691 Palp a 3,498 Kavre 3,482 Bh o jp u r 3,349 T an ah u 3,163 Nu w ako t 3,144 Kh o tan g 2,898 T eh arth u m 2,716 L alitp u r 2,695 Bard iya 2,578 Sin d h u p alch o w k 2,295 O kh ald h u n g a 2,174 G o rkh a 1,410 Parb at 1,302 Ch itw an 1,017 Bh aktap u r 791 Mu stan g 192 Man an g 102 Source: HMIS/MD, DoHS Coverage 132 132 123 117 115 112 111 110 110 109 109 106 105 105 105 104 102 101 101 100 99 98 97 96 95 93 92 92 92 91 90 87 86 86 86 85 85 84 84 83 81 81 81 80 80 80 79 78 78 77 76 76 75 74 74 74 73 73 72 72 70 70 70 69 N A TION A L 69 69 EA STER N 68 67 C EN TR A L 67 67 W ESTER N 65 64 MID - W ESTER N 61 50 34 FA R W ESTER N 88 88 87 81 96 93
- 31. Chapter 2 Child Health: Immunization CHILD HEALTH 2.1 IMMUNIZATION 2.1.1 Background The National Immunization Program (NIP) is a high priority program (P1) of Government of Nepal. Immunization is considered as one of the most cost‐effective health interventions. NIP has helped in reducing the burden of vaccine preventable diseases (VPDs) and child mortality and has contributed in achieving the Millennium Development Goal on child mortality reduction (MDG4). Currently NIP provides vaccination against TB (BCG), diphtheria‐pertussis‐tetanus‐hepatitis B and haemophilus influenza (DPT‐HepB‐HiB), poliomyelitis (OPV) and measles throughout the country and JE vaccine in high risk post campaign districts through routine immunization. TT vaccination is provided to all pregnant women. The routine immunization services are provided through health facilities (fixed clinic), private, NGO or INGO clinics, urban clinics, outreach session and mobile team in geographical inaccessible areas. All vaccines under NIP are provided free of cost. Since the past decades new vaccines are available in the markets, and the Government is keen to provide all available vaccines to reduce morbidity and mortality. Since last 10 years several new vaccines (hepatitisB, Hib and JE) were introduced into routine immunization. In addition to routine immunization services NIP carries out several supplementary immunization activities either to eradicate, eliminate or control vaccine preventable diseases (VPDs). The NIP has comprehensive multiyear (5 year) immunization plan (cMYP) which outlines goal, objectives, activities with milestones and financial plan. The current cMYP runs from 2007‐2011. NIP is also guided by NHSP 2. The National Immunization Program under the Child Health Division has a lead role in all immunization related activities at the national level. The NIP works closely in coordination with other divisions of DoHS, Regional Health Directorates and Districts. The Regional Health Directorate (RHD) acts as a facilitator between the centre and the districts and carries out periodic review of district performances and conduct supportive supervision to strengthen immunization services. It is the responsibility of the D/PHO to ensure that a successful immunization program is implemented at the district and below level. PHCCs, HPs, and SHPs implement immunization programs in their respective municipalities and Village Development Committees (VDCs) ensuring all target children receive immunization services especially marginalized and hard‐to‐reach population. Immunization data generated at the service level are reported to the district, region and the central level (HMIS) on monthly basis. The information received is verified, analyzed followed by corrective actions at different levels. Based on immunization data received from HMIS, NIP monitors the coverage by antigens, dropout rate for different antigens (DPT‐HepB‐Hib1 vs DPT‐HepB‐HIb3, and BCG vs Measles) and vaccine wastage rate (particularly for MDVP vaccines ‐ DPT‐HepB‐Hib, OPV, TT) by districts and provides feedback. In addition to HMIS, surveillance data on certain vaccine preventable diseases (AFP, Measles like illnesses, MNT, pneumonia for AI and AES) are reported through integrated Acute Flaccid Paralysis (AFP) surveillance system from weekly zero reporting sites supported by WHO/IPD. Similarly outbreaks of VPDs are reported through both the HMIS and integrated AFP network. DoHS, Annual Report 2067/68 (2010/2011) 9
- 32. Child Health: Immunization Several activities were carried out in achieving objectives and milestones set in cMYP (2007‐2011) and NHSP2. Vaccination of every eligible child is important especially marginalized and hard‐to‐reach children. Access to routine vaccination has improved in villages and municipalities through REC micro planning, advocacy and social mobilization activities, capacity building trainings, logistics supply, data analysis review meeting at various level etc. Supplementary immunization activities were carried out to achieve or sustain eradication (polio), elimination (MNT) or control (measles & JE) of targeted VPDs. Several rounds of polio campaigns were carried out in high risk districts and JE campaign in 4 districts in this FY. Only one wild poliovirus was detected in last FY in Rauthaut district with date of onset in August 2011. Nepal continue to sustain MNT elimination status, has achieved the objective of reducing measles mortality by 90 percent compared to 2003 data by 2009, has reduced mortality from JE. The issues, challenges and recommendations made by the districts during the regional performance review meeting has guided NIP to better organized immunization related activities in order to achieve its goal and objectives. Goal The goal of National immunization Program is to reduce child morbidity, mortality and disability associated with vaccine‐preventable diseases. Objectives The objectives of the National Immunization Program are as follows: • Achieve and sustain 90 percent coverage of DPT3 by and of all antigens • Maintain polio free status • Sustain MNT elimination status • Initiate measles elimination • Expand vaccine preventable disease (VPDs) surveillance • Accelerate control of other vaccine preventable diseases through introduction of new vaccines • Improve and sustain immunization quality • Expand immunization services beyond infancy NHSP2 targets to achieve 85 percent of children under 12 months of age immunized against DPT3 and measles. Table 2.1.1 presents the immunization schedule of NIP. The target population for NIP include: • All infants (under 12 months) for BCG, DPT‐HepB‐Hib, OPV, and measles vaccines and 12‐23 months children for JE vaccine • All pregnant women for TT vaccine • All grade 1 student for School TT immunization Table 2.1.1: Immunization Schedule of National Immunization Program Type of Vaccine BCG OPV DPT ‐ Hep B ‐ Hib Measles TT TT (School immunization) JE Number of Doses 1 3 3 1 2 1 1 DoHS, Annual Report 2067/68 (2010/2011) Recommended Age At birth or on first contact with health institution 6, 10, and 14 weeks of age 6, 10, and 14 weeks of age 9 months of age Pregnant women Grade 1 students 12‐23 months of age 10
- 33. Child Health: Immunization The key strategies to achieve the above objectives are: 1. Strengthen routine immunization through RED strategies • RED micro planning in all districts • Supportive supervision and monitoring • Increase and promote public awareness and demand through social mobilisation for immunisation services and IEC/BCC interventions • Partnership with private, CBOs, NGOs and others 2. Strengthen municipality immunization services • Fulfil vacant post of vaccinators • Ensure availability of vaccine and other logistics • Supportive supervision and monitoring 3. Conduct supplementary immunization activities and surveillance for eradication of poliomyelitis and control of measles and JE. 4. Sustain Maternal and Neonatal Tetanus elimination status through expansion of school TT immunization program and high TT coverage. 5. Strengthen and expand integrated surveillance of VPDs built on AFP Surveillance (AFP, Measles, Neonatal Tetanus and Japanese Encephalitis) and initiate disease burden study of other vaccine preventable diseases like Hib and Rubella, Pneumococcal and Rota. 6. Conduct periodic meetings of National Committee for Immunization Practices (NCIP), Adverse Event Following Immunization (AEFI) and Inter‐agency Coordination Committee (ICC) committee. 7. Conduct capacity building for relevant health staff (MLM, refresher training, cold chain and vaccine management, maintenance training, in‐country observation tour by EPI staff). 8. Control outbreak of VPDs through appropriate reporting, investigation and response. 9. Improve quality of immunization services practicing injection safety policy. 10. Introduction of new and underused vaccines based on disease burden. 2.1.2 Major Activities The following were the major activities carried out during FY 2067/68. Achievement status of the major activities is presented in Annex 1. 1. Provision of routine immunization services delivery either through fixed sites or outreach sessions: 3‐5 session/month/VDC as per micro plan, conducted RED micro planning in districts of EDR 2. Supported strengthening of municipal immunization through micro planning in 4 municipalities, Kathmandu metro and review of implementation of micro plan in 16 municipalities 3. Conducted review of immunization services as an integrated child health in 5 regions, at VDC level and review by international team 4. Conducted capacity building trainings (ToT on cold chain repair and maintenance for 2 batches, AEFI ToT (20 persons) and RRT in 37 districts, MLM (1 batch), new vaccinators (VHW,MCHW)‐ 8,000 persons) 5. Conducted meetings of NCIP, ICC and AEFI committees 6. Conducted supplementary immunization activities (JE campaign in 4 districts, NID in 75 districts, 7 rounds of responsive Mop‐up (1R in 18 districts, 3R in 8 districts and 3R in 3 districts) 7. Continued school TT immunization program in 12 districts 8. Continued integrated vaccine preventable diseases surveillance (AFP, Measles, NT, AES, pneumonia for AI and Hib), measles case‐based surveillance expanded, outbreaks of suspected measles investigated and responded followed by lab confirmation 9. Continued cross border meeting with Indian counterpart to improve coordination and cooperation for SIAs and AFP surveillance DoHS, Annual Report 2067/68 (2010/2011) 11
- 34. 10. 11. 12. Child Health: Immunization Conducted joint supervision and monitoring in poor performing districts Celebrated "immunization month" Conducted in country exchange visits by EPI staff for sharing of experiences and monitoring of EPI program 2.1.3 Analysis of Achievement Year 2065/66 2008/09 2066/67 2009/10 2067/68 2010/11 DPT‐ HepB‐ Hib 3 2065/66 2008/09 coverage 2066/67 2009/10 2067/68 2010/11 Polio3 2065/66 2008/09 coverage 2066/67 2009/10 2066/67 2009/10 Measles 2065/66 2008/09 coverage 2066/67 2009/10 2067/68 2010/11 TT2 & TT 2+ coverage 2065/66 2008/09 (Pregnant women) 2066/67 2009/10 2067/68 2010/11 EDR 87.4 90.4 92.9 83.3 80.1 92.2 82.9 82.0 90.9 78.0 83.8 87.7 65.6 86.0 82.7 CDR 89.8 96.9 100.7 83.2 82.0 97.0 83.2 82.7 96.0 75.9 86.0 87.0 57.2 76.0 74.9 Region WDR MWDR 78.5 85.7 86.1 104.7 90.7 104.4 76.6 83.5 75.8 88.1 88.0 104.5 75.7 83.7 76.7 92.2 88.0 104.3 69.5 80.8 80.2 97.4 80.9 96.1 57.0 66.7 77.7 80.2 83.7 76.5 FWDR 77.2 99.1 99.4 76.1 86.5 103.3 76.1 89.4 103.2 71.7 91.5 92.8 51.8 66.9 67.6 75 88 86 95 83 81 81 Indicators BCG coverage 82 96 97 85 94 Routine Immunization The overall national immunization coverage for all Routine Immunization Coverage Fig 2.1.1 FY 2065/66 to 2067/68 antigens during the FY 2067/68 compared to 110 previous years is high. BCG coverage is 97 percent, 100 DPT‐Hep B‐Hib3 ‐ 95.8 percent, OPV3 ‐ 95 percent and Measles ‐ 88 percent and JE coverage of 27 90 districts ‐ 54 percent. Coverage of all antigens is in 80 increasing trend compared to last two years (Table 70 2.1.2 and Figure 2.1.1). However teh coverage is not uniform throughout the country and does not 60 BCG DPT3 OPV3 meet target of achieving 90 percent coverage for all antigens. Only 31 districts (41%) have >90 2065/66 2066/67 Source: HMIS/MD, DoHS percent coverage for all antigens and 36 districts (48%) have <90 percent coverage of DPT3. Table 2.1.2: Immunization Coverage, by Region, FY 2065/66 to 2067/68 Measles 2067/68 National 84.9 94.5 97.2 81.2 81.6 95.7 80.9 83.3 95.0 75.4 86.4 87.7 59.8 78.4 78.0 Source: HMIS/MD, DoHS 1. Access and Utilization of Immunization Services Evaluation of access of immunization services are based on first dose of DPT‐HepB‐Hib coverage (>80% as good access), while utilization of immunization services are evaluated against drop‐out rate DPT‐HepB‐Hib1 against DPT‐HepB‐Hib3 (<10% drop‐out as good utilization). Number of un‐ vaccinated children is another important indicator of immunization performance. Districts and VDC DoHS, Annual Report 2067/68 (2010/2011) 12