
Recomendados
Más contenido relacionado
La actualidad más candente
La actualidad más candente (20)
Similar a Lumbar Puncture.pptx
Similar a Lumbar Puncture.pptx (20)
Último
Último (20)
Lumbar Puncture.pptx
- 2. Objectives • To know the indication and contraindication for lumber puncture. • To know the technique of insertion of the lumber puncture. • To know the complications of lumber puncture.
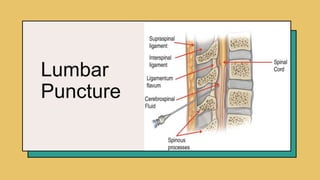
- 3. Introduction A lumbar puncture (spinal tap) is a test used to diagnose certain health conditions. It's performed in your lower back, in the lumbar region. During a lumbar puncture, a needle is inserted into the space between two lumbar bones (vertebrae) to remove a sample of cerebrospinal fluid(CSF). This is the fluid that surrounds your brain and spinal cord to protect them from injury. A lumbar puncture can help diagnose serious infections, such as meningitis; other disorders of the central nervous system, such as Guillain-Barre syndrome and multiple sclerosis; bleeding; or cancers of the brain or spinal cord. 3
- 4. Indications • Measure cerebrospinal fluid (CSF) pressure • diagnosis of suspected CNS infections (bacterial or viral meningitis, meningoencephalitis), intracranial or subarachnoid hemorrhage, and some malignant disorders • Evaluate and diagnose demyelinating or inflammatory CNS processes such as Multiple Sclerosis, Guillan-Barré Syndrome (GBS), Acute Disseminated Encephalomyelitis (ADEM) • Infuse medications which include spinal anaesthesia before surgery, contrast material for diagnostic imaging such as CT-myelography, and chemotherapy drugs directly into the spinal canal • Treat normal pressure hydrocephalus, cerebrospinal fistulas, and idiopathic intracranial hypertension (IIH). 4
- 5. Contraindications • Increased intracranial pressure due to a brain tumor. Cerebral or cerebellar herniation with severe neurological deterioration may occur after the withdrawal of CSF fluid. • Skin infection near the puncture site. The presence of skin infection near the site of the lumbar puncture increases the risk of contamination of infected material into the CSF. • Severe degenerative vertebral joint disease. There will be difficulty in passing the needle through the degenerated arthritic interspinal space. • Severe coagulopathy. Due to the significant risk of epidural hematoma formation. 5
- 6. Equipment • Consent form (Signed) • Lab request forms and specimen bottles • Sterile gloves, Sterile drapes and procedure tray,Sterile gauze pads • Aseptic solution: povidone-iodine solution (Betadine) • Local anaesthetic: Lidocaine 1% solution • 20G and 25G needle,10ml syringe (1) • Spinal needle with stylet (size 22G or 25G) • CSF tube (2 to 4), • Manometer with three-way stopcock 6 20XX
- 7. Procedure • Explain the procedure to the patient or attendant and get informed consent. • Asepsis should be observed during the procedure. • Use local anaesthetic agents to anaesthetise the skin. • Access the subarachnoid space through L2-L3,L3-L4 or L4-L5 intervertebral spaces (L4 can be located between the iliac crests) • Perform manometry. • Collect at least 10 drops of CSF in each of the 4 test tubes. • Apply sterile dressing at the site of the puncture • Place patient in supine position. • Draw serum glucose to compare CSF glucose 7 20XX
- 8. 8 Presentation title 20XX
- 9. interventions and care Before the Procedure Explain the procedure to the patient. Obtain informed consent. Reinforce diet. Promote comfort. Establish a baseline assessment data. Place the client in a lateral decubitus position. Instruct to remain still. After the procedure Apply brief pressure to the puncture site. Place the patient flat on bed. Monitor vital signs, neurologic status, and intake and output. Monitor the puncture site for signs of CSF leakage and drainage of blood. Encourage increased fluid intake. Label and number the specimen tube correctly. Administer analgesia as ordered. 9 Presentation title 20XX
- 10. Post-procedure • Check for headache and ensure PRN simple analgesia prescribed • Advise on good hydration and taking a caffeine-containing drink to decrease headache • Conventionally the patient should lie flat for at least one hour post-procedure though there is no good evidence that this reduces headache • Remember to take blood samples for glucose +/- oligoclonal bands immediately post-LP 10 Presentation title 20XX
- 11. Complications • Post-lumbar puncture headache. The most common complications of LP that occurs due to the leakage of CSF from the puncture site or into the tissues around it. The pain is aggravated while sitting, standing, or coughing and resolves after lying down. • Back pain. A pain or discomfort in the lower back may happen as a result of trauma to the local soft tissue. • Pain or numbness. A feeling of tingling sensation and numbness in the lower back and legs is felt temporarily. • Bleeding. Bleeding is usually noted in the area of the punctured site, or in some rare cases into the subarachnoid, subdural or epidural space. • Brainstem herniation: The increased pressure caused by the removal of CSF during LP will cause sudden shifting of brain tissue 11 Presentation title 20XX
- 12. References • https://nurseslabs.com/ • Wikipedia • Centre for Global Health, Institute of Infection and Immunity,St. George’s, University of London • Oxford Medical Education • The New England Journal of Medicine 12 Presentation title 20XX
- 13. Thank you