
Recomendados
Más contenido relacionado
La actualidad más candente
La actualidad más candente (20)
Similar a Collagen cross linking ppt.pptx
Similar a Collagen cross linking ppt.pptx (20)
Último
Último (20)
Collagen cross linking ppt.pptx
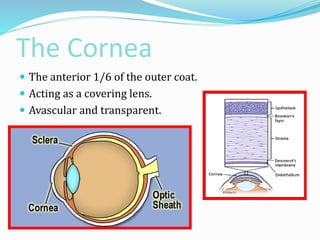
- 1. The Cornea The anterior 1/6 of the outer coat. Acting as a covering lens. Avascular and transparent.
- 2. The Cornea
- 3. BIOCHEMISTRY EPITHELIUM High activities of enzymes of glycolysis. Kreb’s cycle and ATPase pump. High concentration of acetyl choline and choline esterases .
- 4. BIOCHEMISTRY STROMA Low enzymatic activity Collagen fibrils. Glycosaminoglycans occupy the interfibrillar space.
- 5. ENDOTHELIUM Assessment of function 1-Pachymetry Measurement of corneal thickness 2-Specular microscopy Studying number and shape of cells BIOCHEMISTRY
- 7. Keratoconus The disease is characterised by thinning and conus like protrusion of the cornea.
- 10. In progressing / advancing cases of Keratoconus rigid contact lenses can improve visual acuity, yet they can not stop the process. corneal transplantation (penetrating keratoplasty) to achieve better vision. Recently a new procedure has been developed which is supposed to stop the progression of keratoconus.
- 11. A non-invasive treatment C3-R® (corneal collagen cross- linking riboflavin) (CXL) treatment has been proven to strengthen the weak corneal structure. This method works by increasing collagen cross-linking, which are the natural "anchors" within the cornea. These anchors are responsible for preventing the cornea from bulging out and becoming steep and irregular (which is the cause of keratoconus). This procedure stops the progression of the Keratoconus and therefore the need for penetrating keratoplasty could be significantly reduced in the future.
- 12. The first landmark article on this therapy, published 5 years ago, demonstrated clinically significant stiffening of the corneal stroma after CXL in patients with keratoconus. reporting a mean keratometric regression of 2 D over the course of 23 months after 30 minutes of exposure to ultraviolet A (UVA) light and topical application of riboflavin. Potential applications of the CXL technique include the treatment of keratoconus, post-LASIK ectasia and refractory, non healing corneal ulcerations.
- 13. Crosslinking Pharmacokinetics Experimental evidence has shown that the photosensitizer riboflavin and UVA lead to corneal tissue strengthening by increasing collagen covalent bonds, similar to photopolymerization in polymers. CXL induces an increase in the formation of intra- and interfibrillar covalent bonds by photosensitized oxidation, which leads to a biomechanical stabilization of the cornea. The basis of the idea came from scientific evidence that the natural crosslinking effect of glucose increases corneal resistance in young diabetic patients. Interestingly, in these conditions, keratoconus rarely occurs.
- 19. To stabilize the cornea. To stop the progression of the disease. What are the main goals of the UV - cross linking treatment with respect to the named indications?
- 20. The Corneal Cross Linking is relatively easy and low in costs. The main structure of the corneal tissue (stroma) consists of single collagen fibers which are linked - inter connected. The treatment is based on a significant stiffening of the corneal stroma due to photochemical cross linking of the single collagen fibers. Therefore the single fibers form a "denser network" which leads to an increase in the overall stability of the cornea.
- 21. • Which diagnostic tools can be used to rate the efficacy of the treatment? Corneal topography Best-corrected visual acuity Corneal thickness Slit lamp examination of keratoconus level and classification
- 22. • What are the treatment steps ? Local anaesthesia. Manual epithelial removal 6-8 mm OR 30 seconds of application of 20% alcohol. Drop riboflavine 0.1% solution in the glucose polymer Dextran T500 20% solution As a photosensitizer, (every 3 min for approx. 30 min) Observe clear fluorescence within the anterior chamber seen by slit lamb (blue light). Irradiate the cornea with UV-X for 30 min. Drop riboflavin solution every 5 min. Apply every 2 minutes BSS to moisten the cornea. The treatment must always be visually controlled
- 25. • Exclusion criteria: Hazy cornea Pachymetry <400μ Age >40 and <18 years Pregnancy or Nursing Previous anterior segment surgery Systemic Collagen pathology Associated Corneal pathology Severe dry eye
- 26. • How do I check the light intensity ? The nominal value for correct irradiance is 3.0 0.3 mW/cm² (2.7 – 3.3 mW/cm²).
- 27. • How do I have to position the patient ?
- 28. • How much UV – light gets into the eye ? 0.65 J/cm2 70 J/cm2 70 J/cm2 7.7 J/cm2 Damage thresholds 0.46 J/cm2 (9 %) 0.33 J/cm2 (7 %) 0.14 J/cm2 (2.1%) 0.12 J/cm2 (1.9%) Radiant exposures 5.4 J/cm 2
- 29. • Where do I get Riboflavin ?
- 30. provided that the time of application of riboflavin is increased and the presence of riboflavin in the anterior chamber is confirmed by the presence of a yellow flare during slit lamp examination prior to the application of UVA light. Using a UV-X radiation system (Peschke Med, Huenenberg, Switzerland). 370 nm UVA light is applied at a 5-cm working distance for 30 minutes using a 3 mW/cm2 irradiance (approximately 5.4 J/cm2)
- 31. UVA light is applied in precise amounts using a specialized goggle with LED lights
- 32. After the treatment, an antibiotic eye drop is applied, and a bandage contact lens is fitted to the corneal surface until re epithelialization. Combination of a steroid and antibiotic drop is prescribed. During the follow up of eyes so far treated with collagen cross linking very few of the patients showed any more progression
- 34. Clinical Side Effects To date, no remarkable clinical side effects or complications have been noted during clinical trials and studies performed at multiple centers. longer follow up data is needed.
- 35. Mild transient edema is usual in eyes, with a mild cotton-like hazy appearance within the corneal stroma, which usually resolves after 4 to 6 weeks with treatment. A delay in re epithelization had been noted in an eye receiving corticosteroid medication during the period of epithelization and bandage soft contact lens wear. Following withdrawal of the corticosteroid medication, re epithelization was complete within 24 hours