Errors 2
•Download as PPTX, PDF•
6 likes•355 views

Undergraduate ophthalmology lectures

Recommended
More Related Content
What's hot
What's hot (20)
Similar to Errors 2
Similar to Errors 2 (20)
More from faculty of medicine -benha university
More from faculty of medicine -benha university (20)
Recently uploaded
Recently uploaded (20)
Errors 2
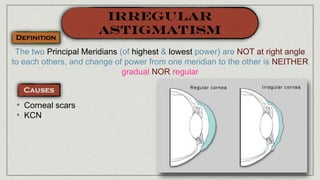
- 1. The two Principal Meridians (of highest & lowest power) are NOT at right angle to each others, and change of power from one meridian to the other is NEITHER gradual NOR regular • Corneal scars • KCN
- 2. • Accommodative asthenopia; continuous attempts of the ciliary muscle to compensate the error • Blurred vision; near & far • Running letters • Distorted objects
- 3. • Cornea: scars, stitches, … • Lens: subluxation • Retina: Staphyloma • e.g. Oil droplet in KCN (Charleux) • Oval optic disc (different refraction along the two principal meridians) • Tilted optic disc (Retinal astigmatism)
- 4. • Scissoring reflex in KCN • Different dioptric power in the two principal meridians • Measure Objectively the refractive error of the eye • Measures the corneal curvature & dioptric power
- 5. • Irregular corneal circles • Pseudo-colour mapping of corneal curvature, power & thickness
- 6. • The patient sees the line in one meridian sharper than that on the perpendicular meridian
- 7. Cylindrical Lenses With its axis perpendicular to the ocular axis to be corrected
- 8. Sphero-Cylindrical Lenses The spherical lens renders the error as simple astigmatism The cylindrical lens corrects the residual astigmatic error
- 9. For low astigmatic errors In KCN
- 10. • A corneal flap is fashioned by an automated keratome • Excimer laser is used to ablate the steep corneal meridian • The flap is re-positioned
- 11. • Partial thickness corneal incisions at the steeper corneal meridian • Applied in low astigmatic errors
- 13. A mark on the IOL denotes the axis of astigmatism to be corrected
- 14. Using a toric IOL
- 15. • Physiological recession of near point of accommodation • Increased lens stiffness • Weak ciliary muscle
- 16. • Usually starts around the age of 40 years (earlier in hyperopes) • Poor near vision e.g reading, sewing • Good far vision • Accommodative asthenopia
- 17. • Monfocal: Reading glasses separate from distant glasses Convex Lens
- 18. • Bifocal glasses • Progressive Addition Lenses (PALs)
- 19. • 1st Correct vision for FAR • Measure the Near Point of Accommodation (PP) • Calculate Amplitude of Accommodation; (1 / PP) • Keep 1/3 accommodation as reserve to give the presbyope range for reading • Correct only the remaining 2/3 • Measure the working distance (usually 33 cm) • Calculate lens power needed to focus at the working distance (1/0.33 = 3D) • Determine the power of the lens needed for correction of Presbyopia (Power at working distance - Power at PP) • Add this power to the power needed for far correction RAF Rule
- 20. • A 45 year old presbyope with + 2D for far • PP at 40 cm • Amplitude of Accommodation = 1/0.40 = 2.5D • 1/3 is kept as reserve i.e 1/3 2.5 = 0.75 D) • Correct only the remaining 2/3 (2.5 - 0.75 = 1.75 D) • Measure the working distance (usually 33 cm) • Calculate lens power needed to focus at the working distance (1/0.33 = 3D) • Determine the power of the lens needed for correction of Presbyopia (3 - 1.75 = 1.25 D)) • Add this power to the power needed for far correction (1.25 + 2 = 3.25 D)
- 22. Convex Lens • Bifocal lenses
- 23. • Excimer laser is used to changes the shape of the cornea to create different power zones for seeing at varying distances
- 24. • Partial thickness scleral pockets are made in each of the 4 eye quadrants • PMMA (PolyMethyl MethaAcrylate) bands are injected into theses pockets • The aim is to expand the scleral ring at the zone of ciliary body, thus stretching the zonules
- 26. • Absence of the crystalline lens • Rare • Trauma • Post operative
- 27. • Defective far vision; because of hypermetropia • Defective near vision; due to loss of accommodation • History of surgery or trauma
- 28. • Scar of cataract extraction surgery • Scar of ruptured globe • Only two Purkinje Sanson images absence of the two Purkinje Sanson images formed by anterior & posterior surfaces of the lens
- 29. • Deep AC
- 30. • Tremulous (Loss of support by the lens), Iridodonesis
- 31. • Jet black colour (Normally a greyish hue appears in phakic clear lenses)
- 32. • High hypermetropia (+ 10 D or more) • Astigmatism Against the rule (Because of contraction of the corneal scar at 12 o’clock position, causing flattening of the vertical meridian) • Anisometropia (In unilateral aphakia)
- 33. Convex Lenses In Bilateral aphakia Prescribe separate glasses for distant & near correction or use bifocals or PALs Convex Lenses In Bilateral or Unilateral aphakia Prescribe Bifocal Lenses, or Monofocal lenses with reading glasses
- 34. It is the best option (Least image magnification) Might be used in Unilateral or Bilateral aphakia Implant monofocal IOLs with additional reading glasses, or implant multifocal IOL
- 35. • Reading ADD in aphakic eyes is + 3D (Accommodation is lost) • Disadvantages of Glasses in correction of Aphakia: 1. Image magnification (30%); Anisometropia in unilateral cases 2. Peripheral abberation 3. Visual field constriction 4. Thick heavy lenses with poor cosmoses
- 36. • A difference of refractive power between the two eyes of 4 D or more • Common • Aphakia
- 37. Anis-eiokonia Different image size in both eyes (>30%)
- 39. • Causes less change in image size (10%) • LASIK • IOL Implantation (1% change in image size)
- 40. • Objective method for assessment of refractive state of the eye by: Illuminating the eye Observation of the direction of movement of red reflex
- 42. • Put Cycloplegic E.D • Back of the eye is illuminated with a streak light coming out of the retinoscope • The Examiner moves the retinoscope from side to side & up and down, observing the red reflex • WITH movement indicates Hyperopia (Put plus lenses) • AGAINST movements indicates Myopia (Put minus lenses) • NO movement indicates emmetropia (Neutral Point) • Subtract Working distance at the end
- 43. + 0.5 DS, + 2.00 DC, Axis 180 + 1.5 DS, - 5.00 DC, Axis 90 - 3.5 DS, + 5.00 DC, Axis 180
- 44. • Automated, Objective method for assessment of refractive state of the eye • Myopia: Prescribe the lowest minus lens that gives the best VA • Hyperopia: Prescribe the highest plus lens that gives the best VA • Astigmatism: High cylinder lenses causes image distortion • Reading Correction is added to the spherical component only
- 45. • Automated, Objective method for assessment of refractive power, Curvature & thickness of the cornea
- 46. ASSESSME NT OF REFRACTIV E ERRORSMOHAMED ABDELZAHER MD, FRCS
- 48. Diminution of vision Defective night vision Difficult near vision Headache Running letters Frowning to see better Ocular Deviation
- 49. History Age
- 50. History Systemic Diseases Drugs The prescription of spectacles should be delayed until a stable refraction is obtained, if possible. Chronic hyperglycaemia myopia Chronic hypoglycemia hyperopia Acute changes in plasma glucose level hyperopia Fukimi O et al Refractive changes in diabetic patients during intensive glycemic control. Br J Ophthalmol 2000;84:1097–1102.
- 52. Exam UAVA
- 53. Exam UAVA
- 54. WHY IS THE PATIENT COMPLAINING?!! 😏 To Declare that the patient is seeing a line, he must read at least ½ of the line correctly.
- 55. More evident in Amblyopia
- 56. Pin Hole Vision improves Vision worsensNo changeRefractive error Corneal opacity Cataract Vitreous hemorrhage Macular lesion
- 58. • Objective method for assessment of refractive state of the eye by: Illuminating the eye Observation of the direction of movement of red reflex
- 59. • Automated, Objective method for assessment of refractive state of the eye • Myopia: Prescribe the lowest minus lens that gives the best VA • Hyperopia: Prescribe the highest plus lens that gives the best VA • Astigmatism: High cylinder lenses causes image distortion • Reading Correction is added to the spherical component only View through an autorefractor
- 63. Transposition + 0.50 DS, - 0.50 DC / 85 0.00 DS, + 0.50 DC / 175 Equals
- 65. If you are not willing to learn, No one can help you. If you are willing to learn, No one can stop you.