Developing a Therapeutic Game Plan for the Management of Hepatocellular Carcinoma: Expert Insights From the Patient CaseBook.
•
1 like•51 views

Richard S. Finn, MD, Robin K. (Katie) Kelley, MD, and Amit Singal, MD, MS, prepared useful practice aids pertaining to the management of hepatocellular carcinoma for this CME/MOC activity titled "Developing a Therapeutic Game Plan for the Management of Hepatocellular Carcinoma: Expert Insights From the Patient CaseBook." For the full presentation, monograph, complete CME/MOC information, and to apply for credit, please visit us at PeerView.com/BXY865. CME/MOC credit will be available until March 5, 2020.

Recommended
Recommended
More Related Content
More from PVI, PeerView Institute for Medical Education
More from PVI, PeerView Institute for Medical Education (20)
Recently uploaded
Recently uploaded (20)
Developing a Therapeutic Game Plan for the Management of Hepatocellular Carcinoma: Expert Insights From the Patient CaseBook.
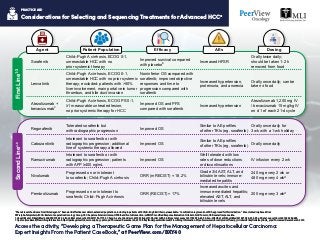
- 1. Considerations for Selecting and Sequencing Treatments for Advanced HCCa a Phase 3 level of evidence for all listed agents. b Real-world effectiveness data in extended populations, including in patients with Child–Pugh B cirrhosis, are available. c Combination regimen is not FDA approved for this indication. d Dose studied in phase 2 trial. AFP: alpha-fetoprotein; ECOG: Eastern Cooperative Oncology Group; HCC: hepatocellular carcinoma; HFSR: hand-foot skin reaction; mRECIST: modified Response Evaluation Criteria In Solid Tumors; ORR: overall response rate. 1. Llovet JM et al. NEnglJMed. 2008;359:378-390. 2. Kudo M et al. Lancet. 2018;391:1163-1173. 3. Cheng A-L et al. AnnOncol. 2019;30(suppl 9): Abstract LBA3. 4. Bruix J et al. Lancet. 2017;389:56-66. 5. Abou-Alfa GK et al. NEnglJMed. 2018;379:54-63. 6. Zhu AX et al. LancetOncol. 2019;20:282-296. 7. Opdivo (nivolumab) Prescribing Information. https://packageinserts.bms.com/pi/pi_opdivo.pdf. Accessed December 20, 2019. 8. Keytruda (pembrolizumab) Prescribing Information. https://www.merck.com/product/usa/pi_circulars/k/keytruda/keytruda_pi.pdf. Accessed December 20, 2019. PRACTICE AID Access the activity, “Developing a Therapeutic Game Plan for the Management of Hepatocellular Carcinoma: Expert Insights From the Patient CaseBook,” at PeerView.com/BXY40 Regorafenib Tolerated sorafenib but with radiographic progression Improved OS Similar to AE profiles of other TKIs (eg, sorafenib) Orally once daily for 3 wk with a 1-wk holiday Cabozantinib Intolerant to sorafenib or with radiographic progression; additional line of systemic therapy allowed Improved OS Similar to AE profiles of other TKIs (eg, sorafenib) Orally once daily Ramucirumab Intolerant to sorafenib or with radiographic progression; patients with AFP ≥400 ng/mL Improved OS Well tolerated with low rates of dose reductions or discontinuations IV infusion every 2 wk Nivolumab Progressed on or intolerant to sorafenib; Child–Pugh A cirrhosis ORR (mRECIST) = 18.2% Grade 3/4 AST, ALT, and bilirubin levels; immune- mediated hepatitis 240 mg every 2 wk or 480 mg every 4 wkd Pembrolizumab Progressed on or intolerant to sorafenib; Child–Pugh A cirrhosis ORR (RECIST) = 17% Increased ascites and immune-mediated hepatitis; elevated AST, ALT, and bilirubin levels 200 mg every 3 wkd Child–Pugh A cirrhosis, ECOG 0-1, unresectable HCC with no prior systemic therapy Improved survival compared with placebob Increased HFSR Orally twice daily; should be taken 1-2 h removed from food Lenvatinib Child–Pugh A cirrhosis, ECOG 0-1, unresectable HCC with no prior systemic therapy; excluded: patients with >50% liver involvement, main portal vein tumor thrombus, and bile duct invasion Noninferior OS compared with sorafenib; improved objective responses and time to progression compared with sorafenib Increased hypertension, proteinuria, and anorexia Orally once daily; can be taken ± food Atezolizumab + bevacizumabc Child–Pugh A cirrhosis, ECOG PS 0-1, ≥1 measurable untreated lesion, no prior systemic therapy for HCC Improved OS and PFS compared with sorafenib Increased hypertension Atezolizumab 1,200 mg IV / bevacizumab 15 mg/kg IV on d 1 of each 21-d cycle Sorafenib FirstLine1-3SecondLine4-8 EfficacyAgent Patient Population AEs Dosing
- 2. Access the activity, “Developing a Therapeutic Game Plan for the Management of Hepatocellular Carcinoma: Expert Insights From the Patient CaseBook,” at PeerView.com/BXY40 Selected Ongoing Clinical Trials in HCC1 PRACTICE AID Immunotherapeutic Agents HIMALAYAa (NCT03298451) IMbrave150 (NCT03434379) 3 3 Durvalumab ± tremelimumab vs sorafenib Atezolizumab + bevacizumab vs sorafenib First-LineAdvancedHCC COSMIC-312 (NCT03755791) LEAP-002 (NCT03713593) 3 3 Cabozantinib ± atezolizumab vs sorafenib Pembrolizumab + lenvatinib vs placebo + lenvatinib NCT03412773a Tislelizumab (BGB-A317) vs sorafenib 3 CheckMate -9DX (NCT03383458) KEYNOTE-937 (NCT03867084) 3 3Nivolumab (adjuvant) vs placebo Pembrolizumab (adjuvant) vs placebo Resectedor LocallyAdvancedHCC EMERALD-1 (NCT03778957) EMERALD-2 (NCT03847428) 3 3 Durvalumab ± bevacizumab + TACE vs placebo + TACE Durvalumab ± bevacizumab vs placebo IMbrave050 (NCT04102098) Atezolizumab plus bevacizumab (adjuvant) vs active surveillance 3 NCT03916627 Cemiplimab 2 CheckMate -9DW (NCT04039607) 3 Nivolumab + ipilimumab vs sorafenib or lenvatinib NCT03638141 2 TACE + durvalumab + tremelimumab Intermediate HCC IMMUTACE (NCT03572582) 2Nivolumab + TACE NCT03347292 1Regorafenib + pembrolizumab Trial Name Trial Arms Phase NCT03841201 2Nivolumab + lenvatinib
- 3. Access the activity, “Developing a Therapeutic Game Plan for the Management of Hepatocellular Carcinoma: Expert Insights From the Patient CaseBook,” at PeerView.com/BXY40 Selected Ongoing Clinical Trials in HCC1 PRACTICE AID a Active, not recruiting. HCC: hepatocellular carcinoma; SBRT: stereotactic body radiation therapy; TACE: transarterial chemoembolization; TTFields: tumor treating fields. 1. https://clinicaltrials.gov. Accessed January 13, 2020. Other Treatment Modalities and Strategies ResectedorLocally AdvancedHCC NCT02762266 SBRT vs TACE 3 NCT02182687 SBRT vs TACE 2 Trial Name Trial Arms Phase Intermediateand AdvancedHCC NCT01730937 SBRT + sorafenib vs sorafenib 3 HEPANOVA (NCT03606590) TTFields + sorafenib 2
- 4. Clinical Monitoring Recommendations for Advanced HCC Treatments1 Access the activity, “Developing a Therapeutic Game Plan for the Management of Hepatocellular Carcinoma: Expert Insights From the Patient CaseBook,” at PeerView.com/BXY40 PRACTICE AID Complete Blood Count (CBC) Comprehensive Metabolic Panel • Sorafenib: B/L, every 2 wk for 2 mo, then mo • Lenvatinib: B/L, every 2 wk for 2 mo, then mo • Regorafenib: B/L, every 2 wk for 2 mo, then mo • Cabozantinib: B/L, every 2 wk for 2 mo, then mo • Ramucirumab: Every 2 wk • Nivolumab: B/L, every 2-4 wk during Tx • Pembrolizumab: B/L and every 3 wk during Tx Thyroid-Stimulating Hormone Sorafenib: B/L, then every 2-3 mo Lenvatinib: B/L, then mo Regorafenib: B/L, then every 2-3 mo Cabozantinib: B/L, then every 2-3 mo Ramucirumab: — Nivolumab: B/L, every 4-6 wk on Tx, every 6-12 wk after Tx Pembrolizumab: B/L, every 4-6 wk on Tx, every 6-12 wk after Tx Clinical Evaluation While on Therapy • Sorafenib: Every 1-2 wk for 6 wk, then mo • Lenvatinib: Every 1-2 wk for 6 wk, then mo • Regorafenib: Every 1-2 wk for 6 wk, then mo • Cabozantinib: Every 1-2 wk for 6 wk, then mo • Ramucirumab: Every 2-4 wk • Nivolumab: Every 2-4 wk • Pembrolizumab: Every 3-6 wk • Sorafenib: B/L, at 2 wk, then mo • Lenvatinib: B/L, at 2 wk, then mo • Regorafenib: B/L, at 2 wk, then mo • Cabozantinib: B/L, at 2 wk, then mo • Ramucirumab: Every 2 wk • Nivolumab: Every 2-4 wk • Pembrolizumab: Every 3 wk
- 5. Clinical Monitoring Recommendations for Advanced HCC Treatments1 a Use caution about applicability of data, because these agents, except for nivolumab, have not formally been tested in patients with Child–Pugh B scores. B/L: baseline. 1. Grieb BC et al. AmSocClinOncolEducBook. 2019;39:248-260. Access the activity, “Developing a Therapeutic Game Plan for the Management of Hepatocellular Carcinoma: Expert Insights From the Patient CaseBook,” at PeerView.com/BXY40 PRACTICE AID Dose Adjustment in Child–Pugh Ba Urinalysis Electrocardiogram (ECG) Blood Pressure • Sorafenib: Every 1-2 wk for up to 8 wk, then mo • Lenvatinib: Every 1-2 wk for up to 8 wk, then mo • Regorafenib: Every 1-2 wk for 6 wk, then mo • Cabozantinib: Every 1-2 wk for up to 8 wk, then mo • Ramucirumab: Every 2 wk • Nivolumab: — • Pembrolizumab: — • Sorafenib: Regularly • Lenvatinib: Regularly • Regorafenib: Regularly • Cabozantinib: Regularly • Ramucirumab: Regularly • Nivolumab: — • Pembrolizumab: — • Sorafenib: B/L, 2-4 wk after start, then every 3 mo • Lenvatinib: B/L, 2-4 wk after start, then every 3 mo • Regorafenib: B/L, 2-4 wk after start, then every 3 mo • Cabozantinib: B/L, 2-4 wk after start, then every 3 mo • Ramucirumab: B/L, 2-4 wk after start, then every 3 mo • Nivolumab and pembrolizumab: — • Sorafenib: None • Lenvatinib: 8 mg daily • Regorafenib: No dose adjustment for bilirubin ≤3 ULN • Cabozantinib: Dose reduce with caution • Ramucirumab: Not indicated; increased hepatic toxicity • Nivolumab: None • Pembrolizumab: No data
- 6. Therapeutic Options in HCC: A Patient Casebook for Physicians PRACTICE AID Access the activity, “Developing a Therapeutic Game Plan for the Management of Hepatocellular Carcinoma: Expert Insights From the Patient CaseBook,” at PeerView.com/BXY40 HCC in Cirrhotic Liver1 Solitary 2-3 nodules 3 cm tnalpsnarT candidate Resection No Yes No tnalpsnarT Ablation Chemoembolization Systemic therapyAblation BSC Optimal surgical candidate Yes Very early stage (0) Single <2 cm Preserved liver function PS 0 Early stage (A) 3-2roelgniS nodules <3 cm Preserved liver function PS 0 Intermediate stage (B) ,raludonitluM unresectable Preserved liver function PS 0 Advanced stage (C) Portal invasion/ extrahepatic spread Preserved liver function PS 1-2 Terminal stage (D) Not transplantable egats-dnE liver function PS 3-4 HCC Patient Cases
- 7. Therapeutic Options in HCC: A Patient Casebook for Physicians PRACTICE AID Access the activity, “Developing a Therapeutic Game Plan for the Management of Hepatocellular Carcinoma: Expert Insights From the Patient CaseBook,” at PeerView.com/BXY40 Case 1 Therapy Considerations for Early-Stage HCC Clinical Presentation and Testing Early-Stage (BCLC A) HCC2-11 • 32-year-old man with chronic HBV, on tenofovir, and with compensated cirrhosis • Undergoing HCC surveillance and found to have liver mass • MRI shows 3.5-cm LR-5 lesion in segment VI • Child–Pugh A: Bili 0.7, Alb 4.0, INR 1.0 • PLT: 217 • ECOG 0 • Patient undergoes robotic liver resection without complication • Returns to clinic, at which time, you reinforce risk of recurrence and need for continued surveillance • Recurrence: 70%-80% at 5 years • No proven adjuvant therapy to decrease HCC recurrence • Ongoing phase 3 trials are testing adjuvant immunotherapy monotherapy and combinations (eg, CheckMate -9DX, KEYNOTE-937, EMERALD-2, IMbrave050)
- 8. Therapeutic Options in HCC: A Patient Casebook for Physicians PRACTICE AID Access the activity, “Developing a Therapeutic Game Plan for the Management of Hepatocellular Carcinoma: Expert Insights From the Patient CaseBook,” at PeerView.com/BXY40 Case 2 Therapy Considerations for Intermediate- Stage HCC Clinical Presentation and Testing Intermediate-Stage (BCLC B) HCC12-13 • AASLD guidance: TACE (level 1 evidence) • Suboptimal long-term survival, particularly in patients with larger tumor burden; offers opportunity for combinations with systemic therapies • Ongoing trials are testing immunotherapy in combination with LRT (eg, phase 3 trial EMERALD-1) • Consideration of transition to systemic therapy is important if patient fails TACE multiple times • 64-year-old man with NASH and compensated cirrhosis • Found to have incidental liver mass on imaging • MRI shows 6.5-cm LR-5 lesion with two satellite nodules • No vascular invasion and no metastatic disease • Child–Pugh A: Bili 0.9, Alb 3.7, INR 1.0 • ECOG 0
- 9. Therapeutic Options in HCC: A Patient Casebook for Physicians PRACTICE AID Access the activity, “Developing a Therapeutic Game Plan for the Management of Hepatocellular Carcinoma: Expert Insights From the Patient CaseBook,” at PeerView.com/BXY40 Case 3 Appropriate First-Line Options for Newly Diagnosed Advanced HCC Clinical Presentation and Testing Newly Diagnosed Advanced (BCLC C) HCC14-20 • 59-year-old man with NASH cirrhosis • Child–Pugh A; AFP 178 ng/mL • No ascites or encephalopathy • ECOG-PS 0 • Previously treated with two rounds of TACE • Follow-up MRI shows multifocal HCC (LR-5) with three lesions, largest 6.5 cm, with invasion into the right portal vein • Sorafenib • Lenvatinib • Emerging option: atezolizumab/bevacizumab (IMbrave150 results) • Phase 3 clinical trials Checkpoint inhibitor + TKI (ie, LEAP-002, COSMIC-312) PD-1/L1 inhibitor + CTLA-4 inhibitor (ie, CheckMate -9DW, HIMALAYA)
- 10. Therapeutic Options in HCC: A Patient Casebook for Physicians PRACTICE AID Access the activity, “Developing a Therapeutic Game Plan for the Management of Hepatocellular Carcinoma: Expert Insights From the Patient CaseBook,” at PeerView.com/BXY40 Case 4 Selecting a Second-Line Targeted Therapy Option Clinical Presentation and Testing Previously Treated Advanced (BCLC C) HCC21-23 • Consider AE profile, AFP levels, liver function, comorbidities, and prior treatment history Regorafenib Did not receive prior sorafenib Ramucirumab AFP levels <400 ng/mL Cabozantinib Allowed up to two lines of prior therapy Favorable data in patients with HBV • 54-year-old Asian woman with chronic HBV on entecavir with undetectable viral load • Treated with TACE for a 6-cm right lobe liver tumor 6 months ago • MRI now shows enlarging 8-cm right lobe tumor, HCC (LR-5), with two satellite lesions and new right branch portal vein tumor thrombus • Child–Pugh A; ECOG-PS 0; AFP level 142 ng/mL • Started on lenvatinib 12 mg daily Required dose reduction to 8 mg/d for fatigue and HTN Demonstrated initial tumor regression on restaging imaging for 6 months Developed lung metastases after 6 months; AFP has risen to 233 ng/mL
- 11. Therapeutic Options in HCC: A Patient Casebook for Physicians PRACTICE AID Access the activity, “Developing a Therapeutic Game Plan for the Management of Hepatocellular Carcinoma: Expert Insights From the Patient CaseBook,” at PeerView.com/BXY40 Case 5 Clinical Presentation and Testing Previously Treated Advanced (BCLC C) HCC • 69-year-old man with chronic HCV was treated and cured with direct-acting antiviral therapy 2 years ago • He then presents to his PMD with right upper quadrant pain • He was found to have an 8-cm mass and satellite lesions in the right lobe; he was hypervascular with delayed washout, and he has right portal vein thrombosis • Hb 12.3; MCV 90; PLT 95; bili 1.8; Alb 3.1; Cr 0.9; AFP 78 ng/mL • History: HCV, T2DM, HTN • No ascites; no encephalopathy; PS 1 • Staging: no extrahepatic disease; BCLC C • Started on sorafenib 400 mg twice daily; dose reduced to 400 mg daily after 3 weeks because of fatigue, weight loss, and anorexia • Continued for 2 months but developed worsening pain and rising AFP, prompting restaging imaging Tumors found on the left lobe, and the right lobe masses are larger Extension of PVT
- 12. Therapeutic Options in HCC: A Patient Casebook for Physicians AFP: alpha-fetoprotein; Alb: albumin; BCLC: Barcelona Clinic Liver Cancer staging system; Bili: bilirubin; Cr: creatinine; ECOG-PS: Eastern Cooperative Oncology Group performance status; Hb: hemoglobin; HTN: hypertension; INR: international normalized ratio; MCV: mean corpuscular volume; NASH: nonalcoholic steatohepatitis; PLT: platelets; PMD: primary medical doctor; T2DM: type 2 diabetes mellitus; TACE: transarterial chemoembolization; TKI: tyrosine kinase inhibitor 1. Galle PR et al. J Hepatol. 2018;69:182-236. 2. Ikai I et al. Cancer. 2004;101:796-802. 3. Vauthey JN et al. J Clin Oncol. 2002;20:1527-1536. 4. Shi M et al. Ann Surg. 2007;245:36-43. 5. Katz SC et al. Ann Surg. 2009;249:617-623. 6. Tabrizian P et al. Ann Surg. 2015;261:947-855. 7. Bruix J et al. Lancet Oncol. 2015;16:1344-1354. 8. https://clinicaltrials.gov/ct2/show/NCT03383458. Accessed January 23, 2020. 9. https://clinicaltrials.gov/ct2/show/NCT03867084. Accessed January 23, 2020. 10. https://clinicaltrials.gov/ct2/show/NCT03847428. Accessed January 23, 2020. 11. https://clinicaltrials.gov/ct2/show/NCT04102098. Accessed January 23, 2020. 12. Marrero JA et al. Hepatology. 2018;68:723-750. 13. https://clinicaltrials.gov/ct2/show/NCT03778957. Accessed January 23, 2020. 14. Llovet JM et al. N Engl J Med. 2008;359:378-390. 15. Kudo M et al. Lancet. 2018;391:1163-1173. 16. Cheng A-L et al. ESMO Asia 2019. Abstract LBA3. 17. https://clinicaltrials.gov/ct2/show/NCT03713593. Accessed January 23, 2020. 18. https://clinicaltrials.gov/ct2/show/NCT03755791. Accessed January 23, 2020. 19. https://clinicaltrials.gov/ct2/show/ NCT04039607. Accessed January 23, 2020. 20. https://clinicaltrials.gov/ct2/show/NCT03298451. Accessed January 23, 2020. 21. Bruix J et al. Lancet. 2017;389:56-66. 22. Abou-Alfa G et al. N Engl J Med. 2018;379:54-63. 23. Zhu AX et al. Lancet Oncol. 2019;20:282-296. 24. El-Khoueiry AB et al. Lancet. 2017;389:2492-2502. 25. Zhu AX et al. Lancet Oncol. 2018;19:940-952. PRACTICE AID Access the activity, “Developing a Therapeutic Game Plan for the Management of Hepatocellular Carcinoma: Expert Insights From the Patient CaseBook,” at PeerView.com/BXY40 Case 5 Consider Checkpoint Inhibitor Immunotherapy as Second- or Third-Line Therapy Previously Treated Advanced (BCLC C) HCC (Cont’d)24,25 When to consider checkpoint inhibitor therapy as a treatment option: • Patients who have not received immunotherapy in first line • If rapid progression and/or intolerance to TKI first-line therapy • If increasing degrees of hepatic dysfunction Prospective cohort and retrospective case series show acceptable safety and efficacy of nivolumab in patients with Child–Pugh B HCC • If contraindications to antiangiogenic therapy (eg, nonhealing wounds, active venous thromboembolism, bleeding complications)