Lip and Tongue Lesion Guide
•Download as PPT, PDF•
26 likes•6,679 views

This document describes normal lip anatomy and various abnormalities that may present on the lip. It discusses the importance of taking a thorough history and performing an examination to determine if a swelling is diffuse or localized, its characteristics, and any associated symptoms. Further testing may be needed to identify underlying causes or deficiencies. Common conditions mentioned include angular chelitis, perioral dermatitis, allergic cheilitis, actinic cheilitis, and mucocele. The document also reviews tongue lesions such as fissured tongue, median rhomboid glossitis, hairy tongue, and geographic tongue, emphasizing the need to consider systemic factors.

Recommended
More Related Content
What's hot
What's hot (20)
Viewers also liked
Viewers also liked (13)
Similar to Lip and Tongue Lesion Guide
Similar to Lip and Tongue Lesion Guide (20)
Recently uploaded
Recently uploaded (20)
Lip and Tongue Lesion Guide
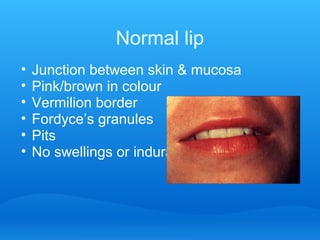
- 1. Normal lip • Junction between skin & mucosa • Pink/brown in colour • Vermilion border • Fordyce’s granules • Pits • No swellings or indurations
- 2. What can you SEE on the lip? What you need to KNOW & to DO for reaching a diagnosis?
- 3. 1- Swellings What you need to DO: • History: o Time first noticed o Any changes in size, consistency, colour,… o Any associated symptoms o Any discharge • Examination o Determine whether it is diffuse or localized o Determine it’s consistency o Determine it’s colour • Further investigations
- 4. 1- Swellings What you need to KNOW • Differential diagnoses … • More you know a longer list of differential diagnosis and better diagnosis
- 5. Diffuse lip swelling Angioedema (allergic / non-allergic)
- 6. Diffuse lip swelling Oedema caused by infection / trauma
- 7. Diffuse lip swelling • Healthy young girl • Swelling notices 6 years ago, increasing gradually • Previous treatment with steroid inj. unsuccessful
- 8. Diffuse lip swelling • Orofacial granulomatosis • Oral Crohn’s disease • Monosymptomatic Melkerson-Rosenthal syndrome
- 13. White lesions of the lip Actinic Cheilitis High risk High risk
- 14. White lesions of the lip Exfoliative chelitis • Excessive production of keratin • More common in females • Associated with stress & anxiety • Some improve by antidepressant/tranquilizers • Spontaneous remission
- 15. Lesions of the lip Allergic chelitis Perioral dermatitis
- 16. Allergic cheilitis Causes: • Allergic reaction to topical ointments/creams or lipstick • Tooth paste • Food • Medication Management: • Detailed history to identify allergen confirmed by patch testing eliminate • Topical steroid (short course)
- 17. Perioral dermatitis • Is a clinical entity with many etiological factors • Most common in females • Could be allergic / idiopathic • Some cases respond to long term tetracycline others to topical steroid (1% hydrocortisone) *DO NOT USE MORE POTENT STEROID ON FACE
- 18. Lesions of the lip Lick eczema • Mainly children are affected • Might not be aware of the habit • Heals by stopping the licking Management: • Appliance can be used to interfere with tongue
- 19. Lesions of the lip Lip fissures • Less common than angular cheilitis • Common in OFG and Down’s patients • Usually persist due to secondary infection (s.aurius or candida) • Management: o Remove pathogen by topical antibacterial / antifungal o Steroid ointment • Usually it recure
- 20. Lesions of the lip Cheilocandidosis Causes: 1.Candidal infection affecting unstable epithelium (Solar irritation) in healthy individual 1.Associated with IO candida Treatment: Early treatment by antifungal might lead to resolution
- 21. Lesions of the lip angles Angular chelitis Inflammation of the corners of the mouth
- 22. Angular chelitis is a multifactorial condition
- 23. How to determine causing factor? • History: o Generalized ill health o Xerogenic medication o Antibiotics / steroid therapy o Ill fitting denture / night wearing • Examination o Signs of anemia o Salivary gland swelling (xerostomia / diabetes) o Intraoral candidosis o Oral dryness o Signs of OFG o Lymphadinopathy o Ill fitting denture / reduced vertical dimension
- 24. How to determine causing factor? • Special investigations o Swab & smear o Blood test (CBC, B12, ferritin, folate) o Blood glucose • when blood testing should by performed? o If suspecting an underlying systemic factor o If local therapeutic measures fail
- 25. Management of angular chelitis 1.Eliminate predisposing factor 2.Correct deficiencies 3.Antifungal / anti bacterial
- 26. Tongue lesions
- 27. The Tongue • Only will consider lesions specific to the tongue NOT ones which are presentation of systemic conditions • Mobile organ • Specialized epithelial lining • Rich in sensory nerve endings
- 28. Developmental abnormalities of the tongue ankyloglossia
- 29. Lesions of the tongue Fissured tongue (scrotal tongue)
- 30. Lesions of the tongue Crenated tongue
- 31. Lesions of the tongue Median rhomboid glossitis
- 32. Lesions of the tongue Coated Tongue • Induced by: o General ill health o Reduced saliva o Painful lesion in tongue o Tobacco & alcohol consumption • Management o Tongue brushing o Mouthwashes containing ascorbic acid
- 33. Lesions of the tongue Hairy tongue Black hairy tongue
- 34. Lesions of the tongue Geographic tongue
- 35. Lesions of the tongue Atrophy of the lingual epithelium • Tongue usually sore • Always look for: o haematinic deficiency o Diabetes o Salivary hypofunction
Editor's Notes
- Non allergic angioedema is the most common and it s idiopathic. Usually it is intermittent and patient should be checked for C1 esterase inhibitor deficiency which lead to uncontrolled complement system activity. Deficincy in C1 esterase inhibitor can be heridetary of aquired Allergic angioedema is an acute state (type I hypersensitivity) could distribute to face, and airways. caused by allergens like food stuff (nuts), medication (ACE inhibitor, NSAID’s, penicillin) rubber latex
- In some oral medicine book consider haemangioma and vascular malformation are the same thing, in fact histologically they are slightly different Haemangioma Vascular malformation varix haematoma DefinitionProliferation of endothelial cells Widening of blood vessels (venous, capillary, arterial) Pathological widening of blood Rupture of blood vessel and collection vessel due to loss of muscular support blood under mucosa aetiologyDevelopmental/congenital Developmental/congenital Usually trauma Acute trauma Onset Start at birth and increase rapidly in the first few months Start at birth Start at older age Immediately after trauma ResolutionDecrease with age and most of them resolve at 9 years Persist throughout life become darker in colour Once established size does not regress Reduce in size and heal Examples Port –wine stainSturg-weber synderom Clinical features Pulsatile if superfecial Blanch if not thrombosed Blanch if not thrombosed or calcified Could be intra-bony
- Also known as self healing carcinoma, could be considered as well differentiated squamous cell carcinoma, it is a skin lesion (does not occur intra orally) suggested that it arises from hair follicle and sun exposure and virus are of suggested etiological factors. Can regress spontaneously in few weeks time, note the centre containing a keratin plug
- More common in females Associated with stress and anxiety Only excessive production of keratin
- )
- Mainly children are affected Might not be aware of the habit Heals by stopping the licking Appliance can be used to interfere with tongue which might help the patient to stop the habit
- Usually persist due to secondary infection (s.aurius or candida) treated by topical application of antibacterial/antifungal + steroid ointment Usually it recur common in OFG and Down patients
- CHX mouth wash is useful in symptomatic fissured tongue
- Usually an indication of bruxism
- Some cases induced by antibiotic use and resolve after completing the course Mucous solvent mouth washes, chemical cauterization and tongue brushing all been tried and usually not effective