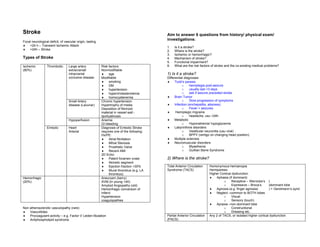
1. Stroke Aim to answer 6 questions from history/ physical exam/
Focal neurological deficit, of vascular origin, lasting
investigations:
♦ <24 h – Transient Ischemic Attack
1. Is it a stroke?
♦ >24h – Stroke 2. Where is the stroke?
3. Ischemic or hemorrhagic?
Types of Stroke 4. Mechanism of stroke?
5. Functional impairment?
Ischemic Thrombotic Large artery Risk factors: 6. What are the risk factors of stroke and the co-existing medical problems?
(80%) extracranial/ Nonmodifiable
intracranial ♦ age 1) Is it a stroke?
occlusive disease Modifiable Differential diagnoses:
♦ smoking ♦ Todd’s paresis
♦ DM o hemiplegia post-seizure
♦ hypertension o usually last <3 days
♦ hypercholesterolemia o ask if seizure preceded stroke
♦ homocystenemia ♦ Brain Tumor
Small Artery Chronic hypertension o Slow progression of symptoms
disease (Lacunar) Hypertrophy of media ♦ Infection (enchepalitis, abscess)
Deposition of fibrinoid o Fever + seizures
material in vessel wall - ♦ Hemiplegic migraine
lipohyalinosis o headache, usu <24h
Hypoperfusion Anemia ♦ Metabolic
GI bleeding o Hyponatremia/ hypoglycemia
Embolic Heart Diagnosis of Embolic Stroke ♦ Labyrinthine disorders
Arterial requires one of the following: o Vestibular neuronitis (usu viral)
Hx/PE: o BPPV (vertigo on changing head position)
♦ Atrial fibrillation ♦ Multiple sclerosis
♦ Mitral Stenosis ♦ Neuromuscular disorders
♦ Prosthetic Valve o Myasthenia
♦ Recent AMI o Guillian Barre Syndrome
2D Echo:
♦ Patent foramen ovale 2) Where is the stroke?
♦ Akinetic segment
♦ Ejection fraction <30% Total Anterior Circulation Homonymous hemianopia
♦ Mural thrombus (e.g. LA Syndrome (TACS) Hemiparesis
thrombus) Higher Cortical dysfunction
Hemorrhagic Aneurysm (berry) ♦ Aphasia (if dominant)
(20%) AVM (in young <40) o Receptive – Wernicke’s )
Amyloid Angiopathy (old) o Expressive – Broca’s )dominant lobe
Hemorrhagic conversion of ♦ Agnosia (e.g. finger agnosia) ) + Gerstmann’s synd
infarct ♦ Neglect –common to BOTH lobes
Hypertension o Visual
coagulopathies o Sensory (touch)
♦ Apraxia –non-dominant lobe
Non atherosclerotic vasculopathy (rare) o Constructional
♦ Vasculitides o Dressing etc.
♦ Procoagulant activity – e.g. Factor V Leiden Mutation Partial Anterior Circulation Any 2 of TACS, or isolated higher cortical dysfunction
♦ Antiphospholipid syndrome (PACS)
2. Lacunar Syndrome ♦ Pure motor o Intracranial Thrombosis
(LACS) ♦ Pure sensory ♦ No investigations, mainly from history, and when carotid Doppler
♦ Sensorimotor and 2D echo are unremarkable
♦ Ataxia-hemiparesis
o Variant is clumsy-hand dysarthria 5) Functional Impairment?
Posterior Circulation Drowsiness
Syndrome (POCS) Lower cranial nerve palsies ♦ Activities of Daily Living
Ataxia o Transferring
Crossed neurological signs o Feeding
Spastic paraparesis o Toileting/ Continence
Bilateral LL sensory loss o Bathing
o Grooming
3) Ischemic or Hemorrhagic? o Dressing
Ischemic Hemorrhagic
♦ Thrombotic ♦ history of coagulopathy 6) Risk factors of stroke?
o Old
o Hypertensive examination may reveal raised ICP ♦ Refer to investigations sections
o Smoking ♦ drowsiness
o Hypercholesterolemia ♦ vomiting
o DM ♦ papilledema
♦ Embolic
o AF, MS, Prosthetic valve
History and Physical Examination
Investigations
♦ CT scan Concise points not to be missed in history:
o mainly for excluding hemorrhagic stroke, esp if thrombolysis is being ♦ Handedness!!!
considered ♦ Weakness
o only half of infarcts seen o duration
♦ Numbness
♦ Upper limb and lower limb involvement
4) Mechanism of Stroke?
♦ Hemianopia
♦ Embolus, or
o Knocking into things?
♦ Extracranial thrombosis, or
♦ Cranial nerves
♦ Intracranial thrombosis? o Diplopia
o Facial asymmetry
♦ History o Dysphagia
♦ Physical Exam o Dysarthria
o AF, MS suggest embolus ♦ Cerebellar
o Carotic bruit suggest thrombosis o Gait, balance
♦ Investigations ♦ Functional impairment
o Transthoracic/ transesophageal echo may give info suggesting embolus ♦ Risk factors
♦ Patent foramen ovale o Ischemic
♦ Akinetic segment ♦ Age
♦ Poor ejection fraction <30% ♦ Smoking
♦ Mural thrombus ♦ DM
o Duplex Doppler of carotids if suspect extracranial thrombosis ♦ HTN
♦ Only for patients with non-disabling PACS who is fit for operation ♦ Cholesterol
and agreeable to endarterectomy o Hemorrhagic
♦ Cerebral angiogram ♦ Family history aneurysms
• To quantify degree of carotid stenosis and status of ♦ Personal history of coagulopathies
intracranial circulation
3. Concise points not to be missed in physical examination ♦ Investigations (to answer all 6 questions)
♦ Full neurological examination Bloods FBC Anemia
♦ Higher cortical function assessment Polycythemia
o Receptive and expressive aphasia PT/aPTT Coagulopathies
o Neglect Fasting lipids
o Apraxia Fasting glucose
o Gerstmann’s syndrome HbA1c
Acalculia, agraphia ANA Lupus/ APS
Left-right disorientation Radiology CT scan To exclude hemorrhagic stroke
Finger agnosia Only 50% infarcts ever become visible
♦ CVS After 7 days, hemorrhages are indistinguishable from
o AF/ murmurs infarcts
o Carotid bruit MRI To posterior fossa lesions, esp if want to exclude tumor
For late presentation of stroke (>7 days)
REMEMBER TO TRY TO ANSWER ALL 6 QUESTIONS AFTER HISTORY AND TTE/TEE For evidence of embolic stroke
PHYSICAL EXAMINATION Carotid Establish carotid thrombosis/stenosis
ultrasound There is a place for carotid endarterectomy if
♦ Symptomatic (TIA/stroke of anterior circulation-
type), and
♦ >70% stenosis of relevant carotid artery
No point doing if it is POCS since posterior circulation
Management and Investigations not by carotid
Transcranial
♦ Acute management of all strokes: Doppler u/s
Vital Hourly heart rate, respiratory rate, Others ECG Document atrial fibrillation
parameters conscious level
Oxygen Supplement if indicated
IV fluids Avoid dextrose and excessive fluid ♦ Specific management:
IV isotonic saline at 50 ml/h unless o Cerebral infarction
otherwise indicated Aspirin Initiate ASAP (within 48 hrs) – safe even
Nil by mouth NBM initially; aspiration risk is during acute phase of stroke
great, avoid oral swallowing until Reduces recurrence of stroke
swallowing assessed. 30ml sip test can be done by HO, unless Reduces
♦ Massive hemorrhagic stroke Thrombolysis IV r-tPA (within 3 hrs) or intra arterial
♦ Brainstem stroke prourokinase (within 6 hrs)
♦ Pseudobulbar palsy Streptokinase is contraindicated in view of
If any of these, get speech therapy to assess swallowing lack of beneficial effect
Hyperthemia Avoid hyperthermia, oral or rectal However, thrombolysis runs the risk of
acetaminophen as needed catastrophic ICH. Since it is difficult to
predict who is at risk of ICH and who
Hypoglycemia Treat hypoglycemia with D50 might benefit, thrombolysis Rx should
Treat hyperglycemia with insulin if serum glucose >300 mg/dL not be routinely used.
Hypertension Do not lower too rapidly, or stroke may be exacerbated due to global
hyperperfusion. Management is same as in hypertensive o Haemorrhage (excluding SAH)
urgency/emergency: Correct coagulation defects, esp for PTs on anticoagulant /
♦ If SBP>220/130, thrombolytics Rx, and those with bleeding diatheses.
o IV nitroprusside or IV labetalol (avoid oral nifedipine Stop all thrombolytics, Antiplatelet agents and anticoagulants
as effect is highly unpredictable)
o Aim to lower BP by 10-20% over 2 hours o Neurosurgical Intervention
o Then aim to lower BP to 160/100 over ~days Intraparenchymal haematomas: surgical evacuation if
haematoma is causing clinical deterioration
4. Secondary Prevention of Stroke
1) Anti-platelet therapy Long term Antiplatelet Rx reduces risk of serious vascular
events (recurrent stroke, MI, vascular death)
Aspirin 75-150 mg/day
Alternatives (when aspirin is CI or fails): Ticlopidine,
clopidogrel, dipyridamole
2) Anticoagulants Warfarin
Indications: AF, valvular heart disease, recent MI
Target INR: 2-3
SE: hemorrhagic transformation
3) Carotid For moderate to severe carotid artery stenosis (>60%) with
endarterectomy ipsilateral carotid territory TIA or non-disabling ischaemic
stroke
Only for surgically fit patients, and under experienced
surgeons.
4) HPT control For all stroke patients, regardless of type of stroke or pre-
stroke BP status
Start only after acute phase of stroke
5) Lipid Statins to reduce lipid levels
6) Stop cigarette smoking
7) Ctrl DM risk factors
Service Delivery
1) Manage within specialised stroke unit if possible
Reduced M&M
Reduced secondary complications of stroke
Reduced need for institutional care thru reduction in disability.
2) Multidisciplinary care
PT/OT
Speech therapist assessment of swallowing function
3) Assess all patients with TIA/minor stroke ASAP
These patients have increased risks of stroke in the period immediately after the
TIA.
Need to assess and perform investigations (ECG, CT head, carotid Doppler)
ASAP
4) Rehabilitation
Early intervention improves physical and functional outcomes. Start ASAP
Rehab preferably done at dedicated stroke rehab unit. If not, perform rehab at a mixed
rehab unit.
5. Acute Management of Stroke 2) Anticoagulants Warfarin
Indications: AF, valvular heart disease, recent MI
Target INR: 2-3
A) Principles of Management of Cerebral infarction SE: hemorrhagic transformation
3) Carotid For moderate to severe carotid artery stenosis (>60%) with
1) Aspirin Initiate ASAP (within 48 hrs) – safe even during acute phase of stroke endarterectomy ipsilateral carotid territory TIA or non-disabling ischaemic stroke
Reduces recurrence of stroke Only for surgically fit patients, and under experienced surgeons.
Reduces 4) HPT control For all stroke patients, regardless of type of stroke or pre-stroke BP
2) Thrombolysis IV r-tPA (within 3 hrs) or intra arterial prourokinase (within 6 hrs) status
Streptokinase is contraindicated in view of lack of beneficial effect Start only after acute phase of stroke
However, thrombolysis runs the risk of catastrophic ICH. Since it is 5) Lipid Statins to reduce lipid levels
difficult to predict who is at risk of ICH and who might benefit, 6) Stop cigarette smoking
thrombolysis Rx should not be routinely used. 7) Ctrl DM risk factors
3) BP control Do no lower BP unless severely hypertensive. A/w worse outcomes.
4) Other therapies Heparin, steroid, neuroprotectants and haemodilution (plasma
volume expanders) have not been found to be beneficial and should
be avoided. Service Delivery
B) Principles of Management of Haemorrhage (excluding SAH) 1) Manage within specialised stroke unit if possible
Correct coagulation defects, esp for PTs on anticoagulant / thrombolytics Rx, and those Reduced M&M
with bleeding diatheses. Reduced secondary complications of stroke
Stop all thrombolytics, Antiplatelet agents and anticoagulants. Reduced need for institutional care thru reduction in disability.
C) Neurosurgical Intervention 2) Multidisciplinary care
Intraparenchymal haematomas: surgical evacuation if haematoma is causing clinical • PT/OT
deterioration • Speech therapist assessment of swallowing function
Hydrocephalus: due to compression of aqueduct of Sylvius by blood or oedema. a/w
cerebellar strokes. Consider ventricular shunting and decompression Sx. 3) Assess all patients with TIA/minor stroke ASAP
These patients have increased risks of stroke in the period immediately after the TIA.
D) Medical Intervention Need to assess and perform investigations (ECG, CT head, carotid Doppler) ASAP
Hyperthermia:
- a/w with exacerbation of ischaemic neuronal injury, increased morbidity and 4) Rehabilitation
mortality. Early intervention improves physical and functional outcomes. Start ASAP
- Manage hyperthermia and investigate for infections – treat with ABx as necessary Rehab preferably done at dedicated stroke rehab unit. If not, perform rehab at a mixed
Hyperglycaemia: rehab unit.
- Diabetics: require sliding scale insulin coverage on top of regular insulin
- Non-diabetics: a/w increased mortality and poorer functional outcome. No data on
optimal glycaemic control, but maintain reasonable glycaemic control.
Secondary Prevention of Stroke
Digitally signed by DR WANA HLA SHWE
1) Anti-platelet therapy Long term Antiplatelet Rx reduces risk of serious vascular events DN: cn=DR WANA HLA SHWE, c=MY,
o=UCSI University, School of Medicine,
(recurrent stroke, MI, vascular death) KT-Campus, Terengganu, ou=Internal
Aspirin 75-150 mg/day Medicine Group, email=wunna.
hlashwe@gmail.com
Alternatives (when aspirin is CI or fails): Ticlopidine, clopidogrel, Reason: This document is for UCSI year 4
dipyridamole students.
Date: 2009.02.22 15:09:19 +08'00'