
Recomendados
Más contenido relacionado
La actualidad más candente
La actualidad más candente (20)
Similar a Dental Anatomy
Similar a Dental Anatomy (20)
Último
Último (20)
Dental Anatomy
- 1. By
- 2. OUTLINE Introduction Definition Tissue of the oral cavity Hard tissues Soft tissues Significances of oral cavity Tooth abnormalities References Abukhaleed 2
- 4. INTRODUCTION Oral anatomy: Is a fundamental of dental sciences on which the oral health care provider is based. The oral cavity is the first area in which digestion of the food we eat begins. All of surrounding and supporting structures in the mouth contribute to the digestive process in one way or another. Abukhaleed 4
- 5. INTRODUCTION CONT. D… The major structures that are found in and around the oral cavity include the 1) Lips, 2) Cheeks, 3) Tongue, 4) Hard palate, 5) Soft palate, 6) Teeth, 7) Gums, 8) Salivary glands 9) U/L jaws Maintaining the teeth in a state of health is of utmost importance for complete digestion and nutrition. Abukhaleed 5
- 6. DEFINITION Is the sciences that deal with the anatomical study of teeth and its related structure within the oral cavity. Abukhaleed 6
- 7. TISSUES OF THE ORAL CAVITY HARD TISSUES Teeth Alveolar bone Hard palate Mandible Maxilla SOFT TISSUES Gums Periodontal ligament Tongues Tonsils Lips Cheeks Uvula Soft palate Abukhaleed 7
- 8. HARD TISSUES Teeth/ Tooth Alveolar bone Hard palate Soft palate Mandible Maxilla Abukhaleed 8
- 9. TEETH It’s the hardest, most calcified structure found within the oral cavity. Crown Root TOOTH Abukhaleed 9
- 10. CROWN - CLINICAL CROWN (corona clinica): the treatable portion of the part visible at that time. – ANATOMICAL CROWN (corona anatomica): the part of the tooth covered with enamel. Thus, the clinical crown and root differ in length from the anatomical crown and root, depending on the patient’s age or the position of the gingival margin. Abukhaleed 10
- 11. BASIC TERMINOLOGY OF DENTAL ANATOMY Human Dentition The teeth that are located in the upper and lower jaws are collectively referred to as the human dentition. Humans have two dentitions throughout life Abukhaleed 11
- 12. TERMINOLOGY CONT.…. Maxillae – The upper jaw is known as the Maxillae. Maxillary Teeth – The teeth located in the maxillae form an arch and are referred to as maxillary teeth. Mandible – The lower jaw is called the mandible. Mandibular Teeth – The teeth located in the mandible are referred to as mandibular teeth. Distal – Away from the midline of the mouth Buccal – Any area on the cheek side of the teeth Lingual – Any area on the tongue side of the teeth Abukhaleed 12
- 13. TERMINOLOGY CONT.….. Facial – Any area on the cheek or lip side of the teeth. Is often used interchangeably with buccal but mostly in the anterior portion of the mouth. Palatal – Any area on the tongue side of the maxillary teeth Occlusal – Any area on the chewing surfaces of back teeth. Incisal – Any area on the biting surfaces of the front teeth. Abukhaleed 13
- 14. TERMINOLOGY CONT.… Posterior – Towards the back of the mouth. Anterior – Towards the front of the mouth Mesial – Towards the midline of the mouth Abukhaleed 14
- 15. Abukhaleed 15
- 16. QUADRANT Each jaw has two (2) quadrant and in every quadrat of an adult dentition consist of 8 teeth, and 5 teeth in primary dentition. Abukhaleed 16
- 17. QUADRANT CONT… The specific brackets are designed to represent each of the four quadrants of the dentition, as if you were facing the patient as seen below Is upper right quadrant Is upper left quadrant Is lower right quadrant Is lower left quadrant Abukhaleed 17
- 18. CLASSIFICATION OF TEETH PRIMARY DENTITION The first set of teeth we get. These are often referred to as baby teeth. There are 20 teeth in the primary dentition. SECONDARY DENTITION The second set of teeth we get. These are often referred to as adult teeth. There are 32 teeth in the permanent dentition Abukhaleed 18
- 19. DIFF BETWEEN PRI. AND SECONDRY TEETH PRIMARY TEETH Consist of 8 incisors, 4canines, 8molars They are smaller in size They are whiter The crowns are shorter Pulp chambers are larger Roots are longer and slender Have fewer anomalies and variations in tooth form SECONDARY TEETH Consists of 8incisors, 4canines, 8premolars and 12 molars They are large Yellowish Crown is longer Dentine is larger Have many anomalies Abukhaleed 19
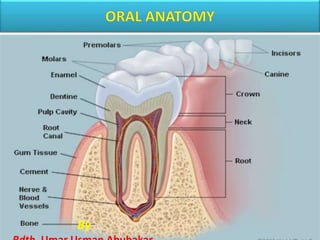
- 21. PARTS OF A TOOTH There are two major part of the tooth crown and root which is further divided into four part, tissues or layer. 1. Enamel 2. Dentine 3. cementum 4. pulp Abukhaleed 21
- 22. ENAMEL Is the white, protective external surface layer of the anatomic crown. It is highly calcified or mineralized, and is the hardest substance in the body. Its content is 95% mineral (calcium hydroxyapatite) The remaining substances include 5% water and enamel matrix. It develops from The enamel organ (ectoderm) and is a product of specialized epithelial cells called ameloblasts Abukhaleed 22
- 23. DENTIN Is the hard yellowish tissue underlying the enamel and cementum, and makes up the major bulk of the inner portion of each tooth (crown and root) Mature dentin is composed of about 70% calcium hydroxyapatite, 18% organic matter (collagen fibers), and 12% water. It harder than cementum but softer and less brittle than enamel. Dentin develops from the mesoderm embryologically. Its forms by odontoblasts cells Abukhaleed 23
- 24. PULP Pulp is the soft (not calcified or mineralized) tissue in the cavity or space in the center of the crown and root called the pulp cavity. The pulp cavity has a coronal portion (pulp chamber) and a root portion (pulp canal or root canal). It develops from the dental papilla (mesoderm) Its soft connective tissue containing a rich supply of blood vessels and nerves, through apical foramen. Abukhaleed 24
- 25. FUNCTION OF PULP Formative: Dentin-producing cells (odontoblasts) produce dentin throughout the life of a tooth. (secondary dentin) Sensory: Nerve endings relay the sense of pain caused from heat, cold, drilling, sweet foods, decay, trauma, or infection to the brain, so we feel it. Nutritive: Blood vessels transport nutrients from the bloodstream to cells of the pulp and the odontoblasts that produce dentin. (Surprisingly, blood in the tooth pulp had passed through the heart only 6 seconds previously.) Defensive or protective: Pulp responds to injury or decay by forming reparative dentin (by the odontoblasts). Abukhaleed 25
- 26. CEMENTUM Cementum is the dull yellow external layer of the tooth root. The cementum is very thin especially next to the cervical line. Its (50–100 mm in thick which composed of ; 65% calcium hydroxyapatite (mineralized and calcified), 35% organic matter (collagen fibers), and 12% water. (Another author, Melfi, states that the mineral content of cementum is about 50%.) Cementum is about as hard as bone but considerably softer than enamel. It develops from the dental sac (mesoderm), and is produced by cells called cementoblasts. Abukhaleed 26
- 27. CEMENTOENAMELJUNCTION (CEJ) The CEJ separates the enamel of the crown from the cementum of the root. This junction is also known as the cervical line, that it surrounds the neck or cervix of the tooth Abukhaleed 27
- 28. TEETH IDENTIFICATION In both the maxillary and mandibular arch there are similar teeth. These include the 1) Incisors, 2) Canines, 3) Premolars 4) Molars. Each of these teeth are located in a different area of the mouth and serve different functions Abukhaleed 28
- 29. TYPES OF TEETH Incisors The four front teeth in the mouth are known as incisors. The two center teeth are known as central incisors and the teeth on either side of them are known as lateral incisors. They are located in both the maxillary and mandibular arches. FUNCTION They act like scissors, for cutting or biting food. Abukhaleed 29
- 30. CANINES The teeth located distal to the lateral incisors are known as canines. These teeth form the corners of the mouth. There are 2 canines in each arch (JAW) FUNCTION These teeth are responsible for tearing food particles when chewing. Abukhaleed 30
- 31. PREMOLARS The teeth located distal to the canines are known as premolars. These teeth are smaller than the molars There are 4 premolars in each arch and two are located behind each canine in the arch. They are only present in the permanent dentition. FUNCTION These are responsible for crushing food in the chewing process. Abukhaleed 31
- 32. MOLARS There are normally 6 molars in each arch; three on the left and three on the right side. They are referred to as first, second and third molars. Some people never develop third molars and often these are the molars that are so far back in the mouth that they have difficulty coming in and may have to be taken out. FUNCTION The role of the molars in chewing is to grind the food. Abukhaleed 32
- 33. TOOTH NUMBERING SYSTEM In order to effectively and efficiently refer to teeth we often use numbering or lettering systems. There are several systems that are used throughout the world. These include :- 1. Universal Numbering System 2. Palmer Notation System 3. International Numbering System. The most widely used system in U.S. dental schools is the Universal Numbering System. Abukhaleed 33
- 34. UNIVERSAL TOOTH NUMBERING SYSTEM HISTORY It was first suggested by Parreid in 1882, and officially adopted by the American Dental Association (ADA)in 1975. It is accepted by third-party providers and is endorsed by the American Society of Forensic Odontology. Abukhaleed 34
- 35. PERMANENT DENTITION This consists of assigning numbers to the teeth in the permanent dentition from 1 to 32 starting with the upper right third molar and continuing over to the upper left third molar and then down to the lower left third molar and onto to the lower right third molar. For example: The mandibular right canine tooth would be tooth #27 Abukhaleed 35
- 36. PERMANENT TEETH Universal Numbering System for Permanent Dentition Abukhaleed 36
- 37. PRIMARY/ TEMPORARY DENTITION Using the Universal Numbering System the primary dentition is identified using letters. Beginning at the second molar on the upper right, the teeth in the maxillary arch are assigned letters A – J. Then continuing with the mandibular left second molar and around to the mandibular right second molar, the teeth are assigned letters K – T. Abukhaleed 37
- 38. PRIMARY/ TEMPORARY TEETH Universal Numbering System for temporary Dentition Abukhaleed 38
- 39. ZSIGMONDY-PALMER SYSTEM HISTORY: In 1861 Adolf Zsigmondy introduced a new dental coding system By preparing four sets of eight (8)numbers 1 - 8, (on each quadrant) used for permanent dentition only. Roman numerals, I,II,III, IV,V. for temporary dentition 1870 Palmer modified the system by using alphabet A-E on each quadrant for the primary dentition. Abukhaleed 39
- 40. ZSIGMONDY-PALMER CONT… V IV III II I I II III IV V V IV III II I I II III IV V E D C B A A B C D E E D C B A A B C D E Zsigmondy-Palmers System. Primary Dentition Permanent Dentition 8 7 6 5 4 3 2 1 1 2 3 4 5 6 7 8 8 7 6 5 4 3 2 1 1 2 3 4 5 6 7 8 Zsigmondy Notational system Abukhaleed 40
- 41. WOLD DENTAL FEDERATION FDI (2 DIGIT ) NOTATION The World Dental Federation notation (also known as the Federation Dentaire Internationale or FDI System) Its Uses two digits for each tooth, permanent or primary. The first digit denotes the quadrant (right or left) and arch (maxillary or mandibular) and dentition (permanent or primary) Abukhaleed 41
- 42. FDI cont…. The second digit denotes the tooth position in each quadrant relative to the midline, from closest to the midline to farthest away. E g; PERMANENT TEMPORARY Quadrant five (5) Upper Right 51- 55 Quadrant six(6) Upper Left 61-65 Quadrant seven(7) Upper Left 71-75 Quadrant four (8) Upper Left 81-85 Quadrant one (1) Upper Right 11-18 Quadrant two (2) Upper Left 21-28 Quadrant tree (3) Upper Left 31-38 Quadrant four (4) Upper Left 41-48 Abukhaleed 42
- 43. FDI 2DIGIT CONT…. PERMANENT 18,16,15,14,13,12,11 21,22,23,24,25,26,27,28 31,32,33,34,35,36,37,38, 48.47,46,45,44,43,42,41 55,54,53,52,51 61,62,63,65,66 85,84,83,82,81 71,72,73,74,75 TEMPORARY Abukhaleed 43
- 44. ALVIOLA BONE Alveolus : small hollow space or socket where the tooth root fits within the jaw bones. Abukhaleed 44
- 45. ALVEOLAR BONE PROPER Is the bony portion of maxilla and mandible where the teeth is embedded and tooth root are supported Alveolar socket is the cavity within the alveolar process in which the root of the tooth is held by the periodontal ligament . When the tooth is multi rooted tooth the bone is called interredicular septum. Its include : I - Cortical plate II - Alveolar crest lll - Trabecular bone Abukhaleed 45
- 46. CORTICAL PLATE Its compose of facial and lingual plate of compact bone. Its dense in nature provide straight and protection Its act for the attachment of the skeletal muscle The mandibular cortical plate is more dense the maxillary due to its less perforation for the passage of nerve and blood vessels Abukhaleed 46
- 47. ALVEOLAR CREST It’s the highest point of the alveolar ridge which joint the facial and lingual cortical plate ALVEOLAR BONE Abukhaleed 47
- 48. TRABECULAR BONE TRABECULAR BONE Abukhaleed 48 Trabecular bone or spongy bone lies within the central portion of the alveolar process and is the less dense, chancellors bone. Its has web-like appearance on a radiographs
- 49. HARD PALATE The hard palate : Is the firm anterior part of the roof of the mouth with mucosa over the underlying bone (namely, the horizontal plates of the palatine bones and palatine processes of the maxillae). The hard palate is covered by keratinized, grayish red to coral pink tissue. Its include the following structure i. Incisive papilla ii. Palatine raphe iii. Palatine ruqae Abukhaleed 49
- 50. STRUCTURE OF THE HARD PALATE Incisive papilla Palatine Rugae Palatine raphe Abukhaleed 50
- 51. INCISIVE PAPILLA This papilla is located over the incisive foramen, where the nasopalatine nerve passes from the nasal cavity onto the palate to innervate the anterior portion of the hard palate. It is the location for injecting anesthetic to numb palatal tissue in this area. Abukhaleed 51
- 52. PALATINE RUQAE [ROO guy] or [ROO jee ] Are a series of palatal tissue elevations, or wrinkles. Its located on the palate just posterior the maxillary anterior teeth. Rugae function in two important ways: tactilely sensing objects or food position in aiding the tongue’s proper placement for the production of certain speech sounds. Abukhaleed 52
- 53. PALATINE RAPHE Is the slightly elevated ridge of firm tissue running anteroposteriorly along the midline of the hard palate. (over the intermaxillary suture attachment between the palatine processes of the right and left maxillae) The mucosa over the raphe is firmly attached to the underlying bone without intervening fat or gland cells. The rest of the tissue on both sides of the raphe has fat or salivary gland Abukhaleed 53
- 54. SOFT PALATE The soft palate : Is the posterior movable part of the roof of the mouth without underlying bony support. The vibrating line is the junction between the hard and soft palate It separates the mouth from the nasal passage If you forcefully say “ah, ah, ah,” you can see the soft palate move (or vibrate) up and down whereas the hard plate does not. Abukhaleed 54
- 55. CLEFT LIP AND PALATE Abukhaleed 55 Cleft palate: •Unilateral •Bilateral •Median
- 57. MAXILLARY BONE CONT… Consists of one large, hollow, central mass called the body, and four projecting processes or extensions of bone. Maxilla Structures The body of the maxilla is shaped like a four-sided, hollow pyramid with the base oriented vertically next to the nasal cavity and the apex or peak extending laterally into part of the cheekbone (or zygomatic bone). The superior portion of the maxilla forms the floor of the orbit of the eye where an infraorbital fissure is located. Abukhaleed 57
- 58. MAXILLARY SINUS OR ANTRUM Sinuses are hollow spaces within bones and are found within the sphenoid, frontal, and ethmoid bones, as well as within each maxilla. Sinuses functions (a) lighten the skull, (b) give resonance to the voice, (c) warm the air we breathe, and (d) moisten the nasal cavity. Abukhaleed 58
- 59. BONY PROCESS There are four processes extending out from the body of the maxillae. 1) Frontal (or Nasofrontal) Process 2) Zygomatic Process 3) Alveolar Process 4) Palatine Process of the Maxilla Abukhaleed 59
- 60. MANDIBLE BONE The single horseshoe- shaped mandible [MAN de b’l]. Is the largest and strongest bone of the face. It is attached by ligaments and muscles to the relatively Abukhaleed 60
- 61. MANDIBLE STRUCTURE It’s the largest and strongest bone of the skull that forms the lawer jaw The mandible is the only bone of the skull that can move The TMJs between the mandible and the temporal bones are movable articulations, the only visible movable articulations in the head. The mandible has 3 mean part i. 2 vertical rami ii . body of the mandible Abukhaleed 61
- 62. BODY OF MANDIBLE An alveolar process surrounds the tooth roots and alveolar eminences are visible as vertical elevations over tooth roots on the facial surface. The prominent elevations overlying the roots of the canines are called the canine eminences. The bulky, curved, horizontal body and the flattened vertical ramus join at the angle of the mandible on either side. The symphysis is the line of fusion of the right and left sides at the midline where the two halves of the mandible (body) fused (joined together) during the first year after birth. It is therefore usually not visible. Abukhaleed 62
- 63. RAMUS OF MANDIBLE There are two processes on the superior end of each ramus. The coronoid process is the more pointed, anterior process on the upper border. The second more rounded and posterior process of the ramus is the condyloid process (also called the mandibular condyle). This process is composed of a bulky condyle head and a narrow neck that attaches the head to the ramus. sigmoid notch or semilunar notch its between two process Abukhaleed 63
- 64. ANOMALIES Diseases of the hard structure affect the enamel and dentine part of the tooth. Some of that diseases are:- 1. Dental caries 2. Amelogenesis inferfectar 3. Dentinogenesis inferfecter 4. Non caries lesion - Attrition - abrasion - eruption and fluorosis Abukhaleed 64
- 65. DENTAL CARIES Dental caries tooth decay is a major oral health problem in most industrialized countries. Its affecting about 60- 90% of school children and majority of an adult. its manifesting from small patch and then demineralised the enamel surface of the tooth Abukhaleed 65
- 66. DENTAL CARIES DEF: - Is define as an irreversible destruction of hard structure of the tooth. (WHO) Abukhaleed 66
- 67. G.V. BLACK’S CLASSIFICATION OF DENTAL CARIES G.V. Black’s Classification of Dental Caries, which was first introduced in 1908 and is still used today. Black’s original classification consisted of five categories, with a sixth added later Abukhaleed 67
- 68. CLASSIFICATION OF DENTAL CARIES Class I: Caries affecting pits and fissures on occlusal third of molars and premolars, occlusal two-thirds of molars and premolars, and lingual part of anterior teeth. Class II: Caries affecting proximal surfaces of molars and premolars. Class III: Caries affecting proximal surfaces of central incisors, lateral incisors, and cuspids without involving the incisal angles. Class IV: Caries affecting proximal including incisal angles of anterior teeth. Class V: Caries affecting gingival one-third of facial or lingual surfaces of anterior or posterior teeth. Class VI: Caries affecting cusp tips of molars, premolars, and cuspids Abukhaleed 68
- 69. MANAGEMENT OF DENTAL CARIES Restoration by the use of restorative dental material Extraction as a last option Abukhaleed 69
- 70. AMELOGENESIS IMPERFECT is a hereditary disorder that affects the enamel formation of both dentitions. Abukhaleed 70
- 71. DENTINOGENESIS IMFERFECTA Dentinogenesis imperfecta Is a hereditary disorder that affects the dentin formation of both dentitions. Clinically, all teeth have an unesthetic light blue- gray to yellow, somewhat opalescent appearance hence the term hereditary opalescent dentin. Abukhaleed 71
- 72. ATTRITION Is define as were away of a tooth structure due to contact with one another during mastication in older age. The incisor tooth is appeared flattened and Its mostly occur in man then woman Abukhaleed 72
- 73. ABRASION/ EROSION Abrasion: Is the wearing away of tooth structure due to friction of the hard object e. g tooth brush The harder material is tend to be more abrasive then the soft one. Erosion: is the chemical wearing away of tooth structure, which lead to damaging of enamel surface erosion Abukhaleed 73
- 74. DENTAL FLUOROSIS Fluorosis is a condition caused during enamel formation by the ingestion of a high concentration of fluoride compounds in drinking water that greatly exceeds the concentration recommended for controlling decay. Abukhaleed 74
- 75. SOFT TISSUES Gums/ mucosa Periodontal ligament Tongues Tonsils Lips Cheeks Uvula Abukhaleed 75
- 76. INTRODUCTION Oral cavity it’s the entrance of the upper digestive tract which is continue into oropharynx. Its divided into two region 1st NS 2ND . 1ST region Is oral vestibule its located external to the dental arch. 2nd region is oral cavity proper which is located internal to dental arch The soft tissues component of the oral cavity are:- Lips mucosa, gingival gums, alveolar mucosa, tongues palate and mucosa covering its, uvula , and floor of the mouth. Abukhaleed 76
- 77. MUCOSA The oral mucosa is lined by a mucous membrane that consists of a lining epithelial tissue and an underlying connective tissue. The oral mucosa can be classified as follows: lining, masticatory, and specialized. FUNCTIONS, protection, taste sensation, and chewing. Abukhaleed 77
- 78. LINING MUCOSA The lining of oral mucosa must be as flexible as possible in order to be protective. Related to chewing, the oral masticatory mucosa permits a free movement of the lips, tongue, and cheek muscles. It exhibits a covering of keratinized epithelium and its connective tissues is strongly attached to the bone to withstand the constant mastication of food. The specialized mucosa that is found in the dorsal surface of the tongue exhibits papillae and taste buds responsible for taste sensation. In the case of the oropharynx mucosa, it is lined by non keratinized squamous stratified epithelium Abukhaleed 78
- 79. ORAL VESTIBULE/ORAL CAVITY PROPER ORAL VESTIBLE; It’s the region surrounded by the lip (buccal) mucosa mucobuccal fold, alviolar mucosa, gingiva and upper and lower dental arch. ORAL CAVITY PROPER; saparated by oral vestible when teeth are in contact between upper and lower jaw. FRENULUM; Is the mucosal fold that run from the central incisors region of the alveolar mucosa to the lip mucosa of the upper and lower. BUCCAL FRENULA; Is the mucosal fold that run from the molar region of the alveolar mucosa. The VESTIBULAR FORNICES (fornix vestibuli superioris and inferioris) form the superior and inferior margins of the oral vestibule, where the mucosa of the cheeks and lips reflect back onto the alveolar mucosa. Abukhaleed 79
- 80. UPPER LIP The lip are fleshy folds tissue around the opening of the mouth. Its covered with the skin on the outer side and mucous membrane on the inner side. The upper lip is also known as superior lip and its close to the nose and chin from the side Abukhaleed 80
- 81. LOWER LIP The lower lip is also known as inferior lip and is the lip close to the chin from the side Its conversed the mouth from the mandibular side (lower jaw) Its covered by the skin from the outer side and mucous membrane from the inner side Abukhaleed 81
- 82. SOFT PALATE Its locate posterior to the hard palate and consist of mainly muscle tissue Its continues posteriorly to the uvula and laterally its related to the tonsils Its movable part of the palate which is connected hard palate via vibratory line Abukhaleed 82
- 83. UVULA Uvula is a projection of the soft tissue which is hang posterior to the soft palate as the continuation its moving upward during same text say ”dangles’’ It prevent the food /liquid that is being swallowed from passing into the nasal cavity FUNCTION i. Prevent food entering to the nasal cavity ii. Producing large amount of saliva to lubricate throat iii. Play role in speech Abukhaleed 83
- 84. TONSIL Palatine tonsil are the pair of soft tissue masses located at the rear of the throat (pharynx) Each tonsils is compose of similar lymph nodes , covered by mucosa (like on the adjacent mouth lining) Abukhaleed 84
- 85. TONSILLITIS TONSILLITIS It’s the inflammation of the 2 oval- sharped pad tissues at the back of the throat. Its can be course by viral or from bacterial infection Abukhaleed 85
- 86. SIGN AND SYMPTOM Sore throat Difficulty swallowing Tender lymph nodes TREATMENT SELF-CARE Tea with honey, salt water gargle and throat lozenge MEDICATION Nonsteriodal anti-imflamatory drug , analgesic and antibiotics SURGERY Tonsillectomy; removal of tonsils Abukhaleed 86
- 87. FLOOR OF THE MOUTH The floor of the mouth lies between the parabolic mandibular body and extends as far as the root of the tongue. It is the muscular base of the oral cavity, being formed by some of the suprahyoid muscles of the hyoid bone, mainly by the mylohyoid muscles (musculus mylohyoidea; running from the mandibular body transversely to the midline of the skull), on which the tongue rests. Above and below these muscles are the sublingual and submandibular salivary glands. This limited sublingual space is often referred to as the floor of the mouth. Sublingual and submandibular salivary glands are found in the floor of the mouth. Abukhaleed 87
- 88. SALIVARY GLAND Salivary glands lie in the oral cavity and produce saliva. They can be classified according to their size. Small salivary glands in the mouth are mucous and serous glands and include the following: Labial glands (glandulae labialis) Buccal glands (glandulae buccalis) Molar glands (glandulae molares), which open into the vestibular area of the mouth Palatine glands (glandulae palatinae) Lingual glands (glandulae linguales), which open into the oral cavity Large salivary glands include the following: Parotid gland (glandula parotis), a serous gland that lies in front of the outer ear and exits in the cheek, level with the second molar (Fig 6-40) Sublingual gland (glandula sublingualis), a mixed gland that lies in the sublingual fossa of the mandible and exits in the sublingual caruncle, a papilla of mucous membrane next to the frenulum of the tongue (Fig 6-41) Submandibular gland (glandula submandibularis), mixed gland that lies in the mandibular Abukhaleed 88
- 90. NERVE SUPPLY SENSORY Roof: by greater palatine and nasopalatine nerves (branches of maxillary nerve) Floor: by lingual nerve (branch of mandibular nerve) Cheek: by buccal nerve (branch of mandibular nerve) MOTOR Muscle in the cheek (buccinator) and the lip (orbicularis oris) are supplied by the branches of the facial nerve Abukhaleed 90
- 91. CHEEKS The cheeks (buccae) originate from the sides of the face at the nasolabial sulcus (sulcus nasolabialis) and, together with the lips, form the external border of the oral vestibule. The cheeks can contain thick pads of fat; the layer of fatty tissue in the faces of women may be twice as thick as in men. The thickness of facial skin varies across the different sections of the face, but it is highly elastic in all areas and has a plentiful supply of blood vessels and nerves. Abukhaleed 91
- 92. CHEEKS COND.. The muscular basis of the cheeks is formed by the buccinator muscle (musculus buccinator), which attaches the cheeks to the molars and premolars. The mucosa of the cheeks, like that of the lips, contains small mixed salivary glands (glandulae buccales). The exit point of the parotid gland in the form of a small mucosal protuberance (papilla parotidea) is located close to the second molar, and this is the reason for the tartar deposits that are commonly found on the vestibular surface of the maxillary molars. Abukhaleed 92
- 93. PERIODONTIUM GUMS Cementum periodontal fibers Periodontal blood vessels Alveolar bone Abukhaleed 93
- 94. PERIODONTIUM cond.. The comprises all the tissues that anchor the tooth in the bone; I e, it is tooth supporting tissue (peri = around, odous = tooth; paradontal = near or close to the tooth). functional unit of various supporting tissues. Firstly because they form a single unit once they have developed. Secondly, they belong together in terms of clinical pathology. Thirdly, they form a compact system for the particular task (function)of anchoring the tooth in the jawbone. Abukhaleed 94
- 95. GINGIVAL The gingiva is the part of the soft tissue in the mouth that covers the alveolar bone of the jaws, and is the only part of the periodontium that is visible in a healthy mouth. Its divided into; Free gingiva (unattached gingival) Attached gingiva. (or marginal gingiva) Abukhaleed 95
- 97. FREE GINGIVA Is a collar of thin gingiva that surrounds each tooth and, in health, adapts to the tooth but provides access into the potential space between the free gingiva and the tooth which is called a gingival sulcus (crevice). The gingival sulcus is not seen visually but can be evaluated with a periodontal probe, since it is actually a space (or potential space) between the tooth surface and the narrow unattached cervical collar of free gingiva. If you insert a thin probe into this sulcus, it should extend only 1 to 3 mm deep in a healthy person. Abukhaleed 97
- 98. INTERDENTAL PAPILLA Is the part of the collar of free gingiva that extends between the teeth. A healthy papilla conforms to the space between two teeth (interproximal space), so it comes to a point near where the adjacent teeth contact. The papilla also has a hidden sulcus where dental floss can fit once it passes between the teeth. Abukhaleed 98
- 99. ATTACHED GINGIVAL Is a gingival that firmly bound to the underlying alveolar bone. It begin from the civical line to the alviolar mucosa Abukhaleed 99
- 100. GINGIVITIS GUMS disease is one of the most common diseases of humans. According to statistics, as many as 75 per cent of adults over the age of 30 may suffer from some form of gum disease at some point in their life. Not only can gum disease cause oral pain, discomfort and tooth loss, it can also seriously affect a person’s overall health. The connection between oral infections and other diseases in the body is be comin understood and accepted within the health-care community Abukhaleed 100
- 101. SIGN AND SYMPTOM Red, swollen or tender gums Gums that bleed when brushing or flossing Receding gums Deep pockets (the space between the gums and the teeth) Metallic taste Tooth sensitivity for no apparent reason Loose or shifting teeth Abscesses Abukhaleed 101
- 102. PERIODONTAL SPACE The periodontal space is a gap about 0.1 to 0.2 mm wide (when healthy) between the cementum and the alveolar bone, which is seen as a thin line on radiographs. This is where the periodontal ligament is located. It is mainly made up of connective tissue fibers that join together to form separate bundles of fibers These are known as Sharpey fibers. The periodontal ligament also contains blood vessels and nerves. Abukhaleed 102
- 103. PERIODONTAL LIGAMENT The periodontal ligament is a very thin ligament composed of many tissue fibers that attach the outer layer of the tooth root (covered with cementum) to the thin layer of dense alveolar bone surrounding a tooth. Abukhaleed 103
- 104. PERIODONTITIS Its an inflammation of the periodontal fiber around the tooth Its course by bacteria Untreated periodontitis can eventually resulting to loss of tooth It may increase the risk of: stroke, heart attach and others health problem Abukhaleed 104
- 105. SIGN AND SYMPTOM Inflamed or swollen gum Bright red gum Pain on gums Receding gums Space between teeth Pus between teeth Bleeding when brushing teeth Loose of teeth Halitosis etc Abukhaleed 105
- 106. TREATMENT OF PERIODONTITIS Good oral hygiene Scaling and cleaning Medication - Antibiotic - Antiseptic Advances periodontitis may need flap surgery (Root planning )or bone and tissue grafts HOME REMEDY Brushing Using dental plus Use mouth wash Extra care of denture, crown or filing's teeth. Abukhaleed 106
- 107. TONGUE The tongue is muscular organ lined by an oral epithelium. It contains numerous specialized structures related to taste sensation Internally, however, the tongue predominantly composed of striated muscle. Abukhaleed 107
- 108. PART OF THE TONGUE Superior surface of the tongue has a v-sharped line known as terminal sulcus which is divided the tongue in to anterior and posterior ROOT is located between hyoid bone and mandible and dorsal portion sits in the oropharynx which attached to the roofing of the mouth BODY Anterior 2/3, rough surface, lingual papilla and lateral portion in relation to the teeth APEX Also known as tip located in the anterior 1/3 of the anterior tongue which rest in incisors teeth and is highly mobile Abukhaleed 108
- 109. SURFACE FEATURES OF THE TONGUE The body and tip (apex) contain test bud which is located in anterior part of the tongue viz VALLATE PAPILLA: Its large and flat papilla arranged in a V-sharped in anterior terminal sulcus FOLIATE PAPILLA: are poorly develop fold on the side of the tongue FILIFORM PAPILLA: are long, conical, pinkish gray projection that are sensitive to tough. FUNGIFORM PAPILLA: are pink to red spots distributed between the filiform papilla and are most dense at the apex and margins of the tongue Abukhaleed 109
- 110. SURFACE FEATURES OF THE TONGUE Abukhaleed 110
- 111. TONGUE CONTD Embryologically the tongue might be classified by anterior and posterior regions. Anterior region: Its about 2/3 of the length tongue, is a visible, highly mobile, and directed forward against the lingual surfaces of the lower incisor teeth. Posterior region : About 1/3 of the length of the tongue has its base on the floor of the mouth, connected with the hyoid bone, epiglottis, and soft palate, styloid process, and approximates the oropharynx. The posterior surface has no lingual papilla but has rough due to present of lymphoid nodule. Inferior surface is connected with the floor of the mouth by a fold known as lingual frenulum Abukhaleed 111
- 112. MUSCLE OF THE TONGUE The tongue muscle can be divided into two intrinsic and extrinsic muscle Intrinsic muscles : The intrinsic muscles are four Superior longitudinal muscles Inferior longitudinal muscles Transvers muscles Vertical muscles These muscles originate and terminate at the within the tongue they do not attach to any bone, they are altering the shape of the tongue Superior and inferior longitudinal muscle retract the tongue by making it short and thick Transvers and vertical muscles protrude the tongue by making it long (narrow) out of the mouth. Abukhaleed 112
- 113. MUSCLE OF THE TONGUE CONTD .. Extrinsic muscles: These muscles are four viz. Genioglossus Hyoglossus Styloglossus Palatoglossus These muscle originate out side the tongues and they are attached to the bone. Abukhaleed 113
- 114. FUNCTION OF TONGUE TASTE: the test buds, the sensory receptors for taste, are located in the tongue. SPEECH: The movement of the tongue are very crucial for articulation during speech. CLEANING: The movement of the tongue dislodge food particle stuck between the teeth gum and cheek so that it can be spat out or swallowed. Abukhaleed 114
- 115. SENSORY NERVE OF THE TONGUE Anterior ⅔: General sensations: Lingual nerve Special sensations : chorda tympani Posterior ⅓: and soft palate General & special sensations: glossopharyngeal nerve Base: General & special sensations: internal laryngeal nerve Abukhaleed 115
- 116. MOTOR NERVE OF THE TONGUE Intrinsic muscles: Hypoglossal nerve Extrinsic muscles: All supplied by the hypoglossal nerve, except the palatoglossus The palatoglossus supplied by the pharyngeal plexus Abukhaleed 116
- 117. BLOOD SUPPLY Arteries: Lingual artery Tonsillar branch of facial artery Ascending pharyngeal artery Veins: Lingual vein, ultimately drains into the internal jugular vein Abukhaleed 117
- 118. OCCLUSION Abukhaleed 118 Normal occlusion: The normal occlusion involves a small vertical overlap of the maxillary teeth over the mandibular anterior teeth, usually without contact. Malocclusion: Its an abnormal relationship of the upper and lower dental arch. Prognathism: If the maxillary anterior teeth protrude considerably, with an adverse esthetic effect and receding chin. Retrognathism: Prognathism takes the form of a reverse vertical overlap of the mandibular anterior teeth, identified by a prominent chin. Open bite: Is a localized malocclusion in which individual teeth in terminal occlusion have no contact in the anterior or posterior segment. If severe, it leads to open mouth breathing together with a susceptibility to caries.
- 120. REFERENCES Woelfel, JB, RC Scheid. Dental Anatomy, Its Relevance to Dentistry. Fifth ed. Williams and Wilkins, Baltimore. 1997, pp. 1-118. https://www.cdha.ca/pdfs/Profession/Policy/research_age nda_102603.pdf Teaford, M. F. Scanning electron microscope diagnosis of wear patterns versus artifacts on fossil teeth. Scanning Microsc. 2, 1167–1175 (1988). Foundation of dental technology anatomy and physiology by Arnold Hohmann Werner Hielscher Abukhaleed 120