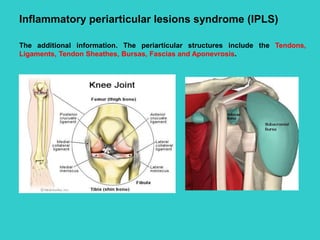
1. Inflammatory periarticular lesions syndrome (IPLS)
The additional information. The periarticular structures include the Tendons,
Ligaments, Tendon Sheathes, Bursas, Fascias and Aponevrosis.
2. Complaints
Regional periarticular pain
1. Usage pain – worse on use, relived by rest. Pain non-progressive
and reproduced by just or a few movements. Apart from the pain, the
patient feels normal.
2. There may be present the rest pain that due to acute inflammation.
Limited movement to one plane;
Localized periarticular swelling.
Present illness
This usually results from an over-usage strain or injury affecting a
periarticular structure. The patient can often state the day or week that it
started and may be able to name an obvious provoking event or injury.
The duration of symptoms is variable.
History
3. Inspection of involved periarticular structure at rest
1. localized redness of the overlying skin
2. localized swelling (bursitis, tenosynovitis)
Attitude of the extremities
(held in “loose-pack” position)
Physical Examination
4. Palpation of involved periarticular structure at rest
1. Localized increasing warmth;
2. Localized periarticular tenderness away from the joint line;
3. Localized swelling [fluid (fluctuant), soft tissue (soft, non-
fluctuant)];
4. Subcutaneous nodules
5. Inspection and auscultation during movement
1. Checking of active movements
• Limited to one plane active movement
• Selective stress pain in direction of use of ligament, tendon or enthesis
[mainly one plane])
2. Checking of passive movements
• Active movement is more restricted than passive
6. 3. Checking of resisted active movement
• Reproduce pain from muscle, tendon, enthesis: e.g. attempted
external rotation reproduces upper arm pain resulting from an teres
minor rotator cuff lesion.
7. 4. Stress tests
• Reproduce pain from ligament or tendon sheath: e.g. passive ulnar
flexion reproduces pain from de Quervain’s tenosynovitis.
5. Checking of crepitus with stethoscope
• The fine, localized crepitus is heard [due to lesion of tendon sheath,
bursa]
8. Lab Tests
1. The full blood count, ESR and C-reactive protein (CRP) may show non-
specific changes that indicate inflammation.
2. Synovianalysis (increased total cell count, crystals, and etc.).
Investigations
9. Imaging Studies
1. Plane X-ray [new
bone formation
(enthesophyte);
calcification os
ligaments, tendons,
burses]
10. 2. US scanning of periarticular structures can confirm their changes;
11. 3. MRI is particulary useful to detect and assess periarticular pathology
(e.g. rotator cuff tears, bursitis, tenosynovitis)
12. Skeletal muscle inflammation syndrome (SMIS)
ComplaintsMuscle pain
There may be the muscle pain in many groups of muscles. However more often the
patient feels the muscle pain in one or few muscles. The character and intensity of
the muscle pain depend on both the expression of the inflammation and the nature
of disorder.
1. Dull or sharp aches in muscles, which are increased by movements, are
typical for SMIS (Usage pain).
2. There may be present the rest pain that due to acute muscle
inflammation.
Swelling of the muscles or Muscle atrophy;
Limitation of the function of joints,
Weakness and Fatigue;
Stiffness. It is sensation of painless resistance to active movements. It is necessary
to specify timing and duration of stiffness. Stiffness is most marked in the early
morning (Morning stiffness) and after inactivity.
There may be other symptoms such as Diplopia, Dysartria, Dysphagia,
Breathlessness.
Non-specific symptoms of systemic illness
History
13. Present illness and Life history
1. Speed of onset. There are acute, subacute or chronic currents of a
SMIS.
2. The previous infections or other provoking factors
3. It is important to know about the setting in which it developed, its
manifestations, treatments, the occurrence of musculoskeletal
disorders in members of their family.
Attitude of the extremities or the trunk
(held in “loose-pack” position)
Physical Examination
14. Inspection of involved
muscles at rest
1. Swelling of the muscles;
2. Muscle atrophy;
3. Dispnoe due to dysfunction
of both intercostals and
diaphragm;
4. Immobile face, ptosis, squint.
15.
16. Palpation of involved muscles at rest
Inflammatory muscle
swelling
Increased in volume;
Tenderness; soft consistence or
hypertone;
Muscle atrophy Muscle-wasting, hypotone
Fibrosis, calcinosis Hard consistence
Inspection during movement
1. Checking of active movements
• Limited to one plane active movement
• Selective stress pain in direction of use of muscle [mainly one plane])
17. 2. Checking of passive movements
• More often reduction of active movements is connected to a muscular spasm
due to the pain. In this situation the range of passive movements is normal. If
structural changes develop in muscles the ranges of both active and passive
movements are reduced.
3. Checking of resisted active movement
• Reproduce pain from muscle.
18. Special Tests
1. Checking of the muscle strength [In SMIS the decreasing muscle strength is
present]
2. Checking of the muscle tone [both hypertone and hypotone are changes of a
normal muscular tone]