
Recommended
Recommended
More Related Content
Similar to 1. Journal Entry The attached (BUROS Center for Testing).docx
Similar to 1. Journal Entry The attached (BUROS Center for Testing).docx (16)
More from ambersalomon88660
More from ambersalomon88660 (20)
Recently uploaded
Recently uploaded (20)
1. Journal Entry The attached (BUROS Center for Testing).docx
- 1. 1. Journal Entry: The attached (BUROS Center for Testing) website link presents and explained the seven assessment competencies needed by teachers in detail: http://buros.org/standards-teacher-competence-educational- assessment- students (Links to an external site.)Links to an external site. . Read the information provided on this site and in your Journal self-reflect on the following question: What is my current level of understanding and skill in these competencies? In your self-reflection be sure to address EACH of the seven competencies. NOTE: It is a self-reflection, so you can NOT use any sources other than the attached website. DUE: in 24 hours How nondirective therapy directs: The power of empathy in the context
- 2. of unconditional positive regard Marvin Frankela*, Howard Rachlinb and Marika Yip-Bannicqc aSarah Lawrence College, New York, USA; bStony Brook University, New York, USA; cNew York University, New York, USA (Received 26 November 2011; final version received 16 May 2012) This paper explains how acceptance and empathy are vehicles for psychothe- rapeutic change by showing how these factors function in nondirective client- centered therapy. The paper argues that because the nondirective client-centered therapist’s unconditional positive regard may conflict with the client’s conditional self-regard, the therapy cultivates a novel restructuring of the client’s narrative. By revealing how positive therapeutic change can result from the interplay of unconditional positive regard and empathy, the article explains the effectiveness of classical client-centered therapy in particular and accounts at least in part for the effectiveness of other therapies that stress the healing properties of the psychotherapeutic relationship. Keywords: empathy; unconditional positive regard; Gestalt figure/ground relationships Wie nicht-direktive Therapie dirigiert
- 3. Dieser Artikel erklärt, wie Akzeptanz und Empathie das Agens therapeutischer Veränderung sind, indem er zeigt, wie diese Faktoren in der nicht-direktiven klient-zentrierten Therapie funktionieren. Gerade weil das bedingungslose positive Beachten des nicht-direktiven klientzentrierten Therapeuten im Konflikt liegen kann mit der Sicht des Klienten auf sich selbst, die voller Bedingungen steckt, gerade deshalb kultiviert die Therapie eine neuartige Restrukturierung des Klienten-Narrativs. Positive therapeutische Veränderung resultiert aus dem Zusammenspiel zwischen bedingungsloser positiver Beachtung und Empathie. Die Effektivität der klassischen Klientzentrierten Therapie ist zumindest teilweise die Ursache, wenn es um die Wirksamkeit anderer Therapien geht, die die heilende Dimension der psychotherapeutischen Beziehung betonen. Cómo dirige la terapia no directiva Este escrito explica cómo la aceptación y la empatı́a son vehı́culos de cambio psicoterapéutico, mostrando cómo funcionan estos factores en la terapia no directiva centrada en el cliente. El escrito argumenta que al entrar en conflicto la consideración positiva incondicional de un terapeuta no directivo centrado en el cliente con la auto consideración positiva condicionada del cliente, la terapia
- 4. cultiva una nueva reestructuración de la narrativa del cliente. Al revelar cómo los *Corresponding author. Email: [email protected] Person-Centered & Experiential Psychotherapies Vol. 11, No. 3, September 2012, 205–214 ISSN 1477-9757 print/ISSN 1752-9182 online � 2012 World Association for Person-Centered & Experiential Psychotherapy & Counseling http://dx.doi.org/10.1080/14779757.2012.695292 http://www.tandfonline.com cambios terapéuticos positivos pueden ser resultado de la interacción de la consideración positiva incondicional y la empatı́a, este escrito explica la eficacia de la terapia clásica centrada en el cliente y explica, al menos parcialmente, la eficacia de otras terapias que hacen hincapié en las propiedades curativas de la relación psicoterapéutica. La manière dont la thérapie non-directive est directive Cet article explique la manière dont l’acceptation et l’empathie sont porteuses de changement dans la thérapie non-directive centrée sur le client, en démontrant la façon dont ces facteurs fonctionnent. Il argumente que le regard positif
- 5. inconditionnel du thérapeute non-directif centré sur le client peut entrer en conflit avec le regard conditionnel sur soi du client, et que pour cette raison, la thérapie facilite une restructuration nouvelle du narratif du client. En démontrant la manière dont le changement thérapeutique positif peut résulter des interactions entre le regard positif inconditionnel et l’empathie, l’article explique l’efficacité de la thérapie centrée sur le client classique et explique, du moins en partie, l’efficacité d’autres thérapies qui mettent l’accent sur les propriétés guérissantes de la relation thérapeutique. Como a terapia não-diretiva dirige Este artigo explica de que modo a aceitação e a empatia são veı́culos de mudança psicoterapêutica, demonstrando como estes fatores funcionam no seio da terapia não-diretiva centrada no cliente. O artigo defende que, uma vez que o olhar incondicional positivo do terapeuta não-diretivo pode colidir com o olhar condicionado que o cliente tem sobre si mesmo, a terapia cultiva uma reestruturação original da narrativa do cliente. Ao revelar como a mudança terapêutica positiva pode resultar da interligação entre o olhar incondicional positivo e a empatia, o artigo explica a eficácia da terapia centrada no cliente clássica e justifica, pelo menos parcialmente, a eficácia de outras terapias que dão
- 6. ênfase às propriedades curativas da relação psicoterapêutica. Introduction The following story highlights the major feature of this article: the directive role of empathy in the context of unconditional positive regard. A few months ago the daughter of a friend of mine informed her father of an insight her client-centered therapist had given her that day. My friend was taken aback. He protested, ‘‘But I said that so many, many times to you to no avail.’’ His daughter insisted that he hadn’t. Then my friend reviewed the last time he had an argument with his daughter and 206 M. Frankel et al. reminded her of what he had said. ‘‘Now, wasn’t this what your therapist said?’’ he asked. His daughter replied, ‘‘It’s amazing, I wonder why I forgot!’’ He said, ‘‘You didn’t remember because you hate to give me credit!’’ But the reason why the daughter didn’t remember what the father said was because he did not in fact say the same thing as the therapist. The father offered his insight in the context of anger, criticism, and rejection, or in a word, blame, thus negating the daughter’s openness to critical feedback. In contrast, by offering his insight in the context of acceptance, in other words, without blame, the therapist encouraged the daughter’s
- 7. self-critical attitude. The insights of the father and therapist were no more the same than gray looks the same on black or on white. Unconscious defense mechanisms such as denial and distortion are not required to explain the daughter’s ‘‘forgetfulness’’ (Rogers, 1959). Therapeutic empathy in the context of unconditional positive regard necessarily provides a novel context for self-criticism. Classical client-centered therapy (CCCT) is thus nondirective with respect to the content of the narrative but directive with respect to the attitude that the client brings to the narrative, which in turn transforms the content. We agree with Barbara Brodley that it is mistaken to view the nondirective model as merely one that influences the client. As Brodley (2005) aptly stated, ‘‘. . . all therapies influence . . . clients towards growth and healing. A therapymust influence in order to be effective . . .. The non-directive issue exists at a different level from the discourse on therapy as influencing clients’’ (p. 1). We disagree, however, with her about the nature of this difference. Whereas she argued that ‘‘[e]mpathic understanding, unconditional positive regard and congruence are all non-directive with respect to the client’’ (p. 1), we maintain that the therapist’s communication of unconditional positive regard is directive in cultivating the client’s unconditional positive self- regard and enabling the client to view his/her narrative through this lens. This directive component is too
- 8. systematically employed to be regarded as a mere influential agent. We also consider the model directive rather than influential in the sense that the CCC therapist is going beyond the client’s frame of reference and is thus inconsistent with the alleged essence of nondirective therapy which was to empathically and exclusively respond to the client’s internal frame of reference (Rogers, 1951). As described by Rogers (1951) in Client-Centered Therapy, one major aim of the CCC therapist is to: perceive as sensitively and accurately as possible all of the perceptual field as it is being experienced by the client, with the same figure-ground relationships, to the full degree that the client is willing to communicate that perceptual field; and having thus perceived this internal frame of reference of the other as completely as possible, to indicate to the client the extent to which he is seeing through the client’s eyes. (p. 34) This is, in effect, our operational definition of empathy. We will show, however, that in fact Rogers never empathically reflected ‘‘the same figure- ground relationships’’ as those of the client. Instead he provided a direction by changing the context of the client’s narrative which then transformed the meaning of the client’s experience. The directivity we will be discussing is different from that of other person-
- 9. centered therapies (Cain, 2010), such as those that validate or reassure the client’s experience (Bohart, Elliott, Greenberg, & Watson, 2002; Brink & Farber, 1996), offer evocative reflections (Rice, 1974), or empathic responses that attempt to target the client’s ‘‘edge of awareness’’ (Mearns & Thorne, 1999). Some later forms of person-centered therapy (process directive therapy and relational depth therapy, for example) also tend to introduce various directive elements during the course of Person-Centered & Experiential Psychotherapies 207 therapy (process guiding techniques, therapist self-disclosures, etc.) that might obscure the subtle kind of continuous directivity that takes place in CCCT. While this analysis focuses on CCCT, it is relevant to all psychotherapies that emphasize the importance of acceptance and empathy as a necessary if not a sufficient condition for effective treatment (Farber, 2007); this would include multi- modal therapy (Lazarus, 2005) or any form of cognitive-behavioral therapy. A novel background creates a novel client narrative How do unconditional positive regard and empathy contribute to therapeutic change? After all, empathic reflection does not bring anything new by way of meaning into the client’s frame of reference; instead, it captures, as
- 10. accurately as possible, what is already there in the client’s current frame of reference (Rogers, 1951, 1959). The often-heard client response to an accurate empathic reflection, ‘‘Yes, that’s precisely it,’’ demonstrates this. Rogers’s filmed therapeutic encounter with Gloria (Shostrom, 1965) provides an example of such a response: Rogers: And you feel, this is a conflict and it’s just insoluble and therefore it’s hopeless and here you’ve looked up to me and I don’t seem to give you any help, to . . . This empathic reflection lifts any burden of responsibility and blame from Gloria’s shoulders for her predicament, but just as importantly Rogers openly accepts Gloria’s perception that he was of no help without blaming himself, thus modeling a blameless attitude. Gloria: Right . . . Gloria’s despair when she utters that single word ‘‘Right’’ was not only a confirmation of Rogers’s empathic reflection but a novel expression of her sense of hopelessness. The written word fails to do justice to her troubled expression when she agrees with Rogers. But how did this come about? The noted historian and existential phenomenologist van den Berg (1974) captured the point that an accurate empathic reflection, apart from the communica-
- 11. tion of unconditional positive regard, brings nothing novel to the client’s narrative when he characterized nondirective therapy as one in which the counselor does ‘‘nothing.’’ Of course, van den Berg was not suggesting that Rogers was truly doing nothing, but only that, unlike directive therapies of that time, Rogers did not offer novel interpretations that went beyond or contradicted the phenomenal field of the client. Van den Berg was not suggesting that nondirective therapy was ineffective but only that Rogers was taking an original psychotherapeutic approach by attempting to offer only nondirective reflections of the client’s frame of reference, offering nothing whatsoever from his own frame of reference. Rogers viewed interpretations, self- disclosures, advice and even commendation as reinforcing the undesirable power relations between therapist and client (Rogers, 1942). However, a closer examination will show that Rogers was not offering a purely nondirective response. Consider the following dialogue between Rogers and a client (Kirshenbaum, 1979, p. 248): Client: (. . . begins to talk in hard flat voice, quite unlike her usual tone. Does not look at counselor . . .) You feel I want to come, but I don’t! I’m not coming anymore. It doesn’t do any good. I don’t like you. I hate you! I wish you were never born.
- 12. 208 M. Frankel et al. Rogers: You just hate me very bitterly. Client: I think I’ll throw you in the lake. I’ll cut you up! You think people like you, but they don’t . . . You think you can attract women but you can’t . . . I wish you were dead. Rogers: You detest me and you’d really like to get rid of me. Client: You think my father did bad things with me, but he didn’t! You think he wasn’t a good man, but he was. You think I want intercourse but I don’t. Rogers: You feel that I absolutely misrepresent all your thoughts. Client: . . . You think you can get people to come in and tell you everything, and they’ll think they’re being helped, but they’re not. You just like to make ’em suffer. You think you can hypnotize them, but you can’t! You think you’re good, but you ain’t. I hate you. I hate you. Rogers: You feel I really like to make ’em suffer, but I don’t help them. Client: You think I haven’t been straight, but I have. I hate you. All I’ve had is pain, pain, pain. You think I can’t direct my own life, but I can. You think I can’t get well,
- 13. but I can. You think I had hallucinations, but I didn’t. I hate you. (Long pause, leans on desk in strained, exhausted pose.) You think I’m crazy but I’m not. Rogers: You’re sure I think you’re crazy. Client: (Pause) I’m tired, and I just can’t get loose! (Despairing tone of voice and tears. Pause) I had a hallucination and I’ve got to get it out! . . . (Goes on about her deep conflicts, and tells of her hallucination she has experienced with terrific tension in her voice, but with an attitude very different from that at the beginning of the interview.) (Later in interview) Client: I knew at the office I had to get rid of this somewhere. I felt I could come down and tell you. I knew you’d understand. I couldn’t say I hated myself. That’s true but I couldn’t say it. So I just thought of all the ugly things I could say to you instead. Rogers: The things you felt about yourself you couldn’t say, but you could say them to me. Client: I know we’re coming to rock bottom. In a footnote, Rogers wrote: ‘‘Just as it is impossible to convey on paper the venom and hatred in the client’s voice, so it is utterly impossible to convey the depth of empathy in the counselor’s responses. The counselor states, ‘I tried to enter into and
- 14. to express in my voice the full degree of soul-consuming anger which she was pouring out. The written words look incredibly pale, but in the situation they were full of the same feeling she was so coldly and deeply expressing’’’ (italics added). But if Rogers’s version of what he did is true, if he is merely providing an empathic understanding that remains entirely within the phenomenal field of the client, then why doesn’t the client simply say to each and every one of the empathic reflections: ‘‘But you are simply repeating the meaning of what I just said’’? The answer is that although Rogers is repeating the words, he is not repeating the context of the words and hence the meaning of the words. The client’s assertions are contextualized by her contempt for herself (‘‘I couldn’t say I hated myself’’). Rogers’s statements are contextualized by his compassionate acceptance (uncondi- tional positive regard) of the client. The client was in effect saying: ‘‘I hate you Carl Rogers!’’ In response Rogers asserted, ‘‘I appreciate but do not blame you for the extent of your contempt of me.’’ Indeed, each of Rogers’s empathic reflections could be preceded with the statement, ‘‘I appreciate but do not blame.’’ For this reason, the client did not say to Rogers, ‘‘That is what I just said,’’ since Rogers is never just repeating the meaning (I hate you, Carl Rogers) of the client’s assertions but Person-Centered & Experiential Psychotherapies 209
- 15. conveying his unconditional positive regard for them. When Rogers wrote that ‘‘it is utterly impossible to convey the depth of empathy in the counselor’s [Rogers’s] responses,’’ he was, in our terms, referring to his unconditional positive regard for the client, which frames his empathic response, rather than just his empathic response. Consequently, the client does not understand Rogers as giving a redundant response. On a more clinical level, the client is expressing her feelings of self-contempt and in return is finding herself not only understood but prized by Rogers. Conceptually, empathy and unconditional positive regard are independent of each other (Rogers, 1957; Shlien, 1997). In fact, a person may be empathic and rejecting at the same time. The journalist Gita Sereny was mainly empathic with the former commandant of a death camp, Franz Stangl, over a period of months but had to excuse herself from one particular interview in utter disgust when confronted with the moral perversity of the commandant (Sereny, 1995). Shlien was so critical of the tendency to blur the distinction between empathy and unconditional positive regard among contemporary person-centered therapists that he highlighted how empathy can ‘‘be a weapon of war, an advantage in every form of competition as well as in
- 16. cooperation’’ (Shlien, 1997, p. 64). But a person can mistakenly feel accepted and safe when being empathically understood. In her book, The Journalist and the Murderer, Janet Malcolm commented on the moral dilemma journalists face when they win the confidence of an alleged criminal simply by understanding them in an empathic way. The alleged criminal feels so accepted that he lets his guard down only to discover, when he reads the journalist’s negative written account, that he was betrayed (Malcolm, 1990). Like Malcolm, existential therapists use empathy to establish rapport and allow clients to be feel accepted when they are lying (to themselves) only at a later time to express their criticism of the clients’ moral position. Prochaska and Norcross (2003), summed up this approach in contrast to the approach of CCC therapy by offering the following description: Existentialists do not agree, however, that a therapist must maintain unconditional positive regard toward the patient. In order to be authentic, the therapist can respond with positive regard only toward honesty and authenticity but never toward lying and pathology. That the therapist at first allows the patient to lie and objectify without overt judgment is accepted in order for the therapist to experience the patient’s phenomenal world. But an authentic therapist can hold no positive regard for a patient’s lying. (p. 124)
- 17. For Rogers, the client’s perception of the CCC therapist’s unconditional positive regard is accurate and not illusory since Rogers has no ulterior motive (writing an article, making an evaluation, inducing a change in a specific direction, etc.) in his relationship with the client. The client is thus justified in feeling unconditionally accepted. By changing the meaning of the client’s narrative through his/her unconditional positive regard, the CCC therapist is introducing a novel feature to the therapeutic discourse and in this significant sense CCCT is directive. The novel context (unconditional positive regard) dramatically alters the text (empathic understand- ing). Thus, in the above dialogue, the client is liberated from her self-protective strategy when she states: ‘‘I couldn’t say I hated myself. That’s true, but I couldn’t say it.’’ In other words, the client offered her narrative with conditional self-regard but received the meanings and feelings of her narrative with unconditional positive regard. In offering his words with a tone of compassion and acceptance, it is as 210 M. Frankel et al. though Rogers is saying in each exchange: ‘‘Here is what you might say if you did
- 18. not blame yourself but had instead unconditional positive self- regard.’’ The power of empathy in the context of unconditional positive regard should come as no surprise since Gestalt psychologists have demonstrated that figure- ground relationships govern all perception. Thus a gray circle on a black background will be seen as white while the same gray circle on a white background will be seen as black. As Rachlin (1994) described this phenomenon: The two spots differ in brightness not because the different backgrounds fool the observer creating an illusion . . . but because of a fundamental fact about phenomenal experience; what you perceive in the first place . . . is the relationship between the spot (gray figure) and its background. . . . [Consequently] on the most fundamental level of perception the two gray spots differ in brightness. Context is thus not a correction to perception or a distorter of perception but a vital component of the fundamental perceptual process. (pp. 7–8) For example, the client offered her narrative, ‘‘You think I had hallucinations, but I didn’t. I hate you’’ (the figure) against the implicit background of her conditional self- worth: ‘‘maybe as much as I hate myself.’’ And so to carry the analogy one step further, the narrative figure is black indeed. The client, if alone at home, may not even be able to experience hostility towards Rogers lest she think
- 19. less of herself (lowered conditions of self-regard) for attacking her therapist. However, in the context of the therapy, Rogers offered an empathic and compassionate reflection, ‘‘You’re sure I think you’re crazy’’ (the figure) against the background of unconditional positive regard, rendering the narrative figure white. In effect, then, the narrative the client initially authored is not the same narrative that is expressed by the therapist. The client’s attack on Rogers resulted in her being accepted by Rogers in no less a way than she was prior to the attack. Indeed, Rogers embraced her rage. Consequently, in listening to Rogers’s response, the client is directed to reflect on a novel meaning of her narrative, and re-view her hatred of Rogers without adding the insult of conditional self-acceptance. In this formulation, Rogers’s unconditional positive regard encouraged the client’s hopes that despite her rage she is beyond blame or praise and thus broadened her perceptual field. In this case, the broadened perception includes the fact that the client hates herself rather than Carl Rogers. Yet, why do clients so often say, ‘‘Yes, you understand me perfectly,’’ when, in fact, their conditional self-regard (implicit or explicit) goes counter to the therapist’s unconditional positive regard? For example, a client who is familiar with Rogers’s vocabulary (Rogers, 1959) might say, ‘‘It is evident that you have unconditional
- 20. positive regard for me, but I have only conditional positive self- regard. Your empathic reflection captures the essence of my feelings perfectly but your total acceptance of me is contrary to the way I feel about myself.’’ Clients do not say this but instead more often than not claim that they feel understood. How then can we make sense of the client’s subjective experience of being so understood? We suggest that it is not entirely accurate to describe clients as simply having conditional positive self-regard (Rogers, 1959). It would be more correct to say that clients are ambivalent about their conditional worth and may hope that their narrative will be utterly acceptable (unconditionally) and even prized by the therapist even as they may fear their narrative will only be conditionally accepted or in fact rejected. Clients often reveal this ambivalence when they express the wish to see themselves in the same benevolent way as their therapists do. One of the authors (MF) recalls from his internship at the Counseling Center of the University of Chicago, one client Person-Centered & Experiential Psychotherapies 211 saying in so many words: ‘‘If I saw myself as you see me I would have little need of you, right?’’ In effect, then, we are suggesting that the unconditional positive
- 21. regard of the therapist fulfills the client’s hopes of acceptance while the empathic reflection illumi- nates the content of the narrative which often expresses shame, guilt, and fears of rejection. The subtext of ‘‘Yes, that’s exactly what I mean,’’ could be understood to mean: ‘‘Yes, you have understood my unspoken hopes to be accepted as well as what I have said.’’ It is true that the CCC therapist will empathically communicate the client’s ambivalence about her self-worth when this is the explicit subject matter of the client’s narrative (the figure), but even then the CCC therapist’s unconditional positive regard conveys a more positive view of the client than the client’s view of herself. Whence the power of unconditional positive regard? Why does the client care at all about being accepted by the therapist? So far as the client is concerned the therapist may be a perfect jerk in his/her own personal and professional life. The therapist does not possess a Ph.D. in maturity or wisdom. Is the unconditional positive regard of the therapist important because of the client’s misperception and overvaluation of the therapist’s character (sensibility, wisdom, expertise)? Freud certainly thought so. The power of the analyst, psychoanalysts argue, resides in the childhood wishes of the client to have a powerful ally. Without the preservation of these wishes, the analyst would be powerless (Freud, 1966). This
- 22. is the essence of positive transference which was itself viewed as a neurosis that eventually had to be extinguished. From this perspective, then, it is only because of ‘‘a positive transference neurosis’’ that the interpretations of the analyst or the explicit empathy and unconditional positive regard of the client- centered therapist are seriously entertained by the client. Rogers eschewed transference and instead stated that people have a need for positive regard that may either be innate or quickly learned and is an expression of the actualizing tendency (Bozarth & Wang, 2008; Rogers, 1959). But to say the client desires the positive regard of the therapist because the client has a need for positive regard and to define the need for positive regard in terms of the client’s desire for it is circular. In any case, we do not seek the positive regard of everyone but only of those we respect. We propose instead, that the CCC therapist’s empathic communications and unconditional positive regard earn the trust and respect of the client. While all therapists may sincerely claim to have a nonjudgmental attitude towards the client, only CCC therapists refrain from offering any comments from the therapist’s frame of reference and in so doing demonstrate a singular openness to the client’s narrative. In this way, the CCC therapist is offering a relationship different from other therapeutic relationships. For example, CCC therapy goes contrary to the current
- 23. practice of personal self-disclosure by therapists to influence their clients to live more optimally (Hill & Knox, 2002, pp. 255–266). In brief, the CCC therapist is providing a unique experience for the client; therein may reside the power of his/her unconditional positive regard. Summary and conclusions This paper offers an alternative to Rogers’s understanding of the effects of uncon- ditional positive regard and empathy by explaining how they work in conjunction with 212 M. Frankel et al. one another. In his introductory comments to the interview with Gloria, Rogers discussed the probable consequences of his empathic and accepting attitude: She’ll explore some of her feelings more and attitudes more deeply. She is likely to discover some hidden aspects of herself that she wasn’t aware of previously. Feeling herself prized by me, it is quite possible she’ll come to prize herself more. Feeling that some of her meanings are understood by me, then she can more readily perhaps listen to herself, listen to what is going on within her own experience. (Shostrum, 1965) In his description, Rogers isolated the effects of his
- 24. unconditional positive regard (his prizing of her will result in her prizing herself) from the effects of his empathic understanding (‘‘. . . feeling that some of her meanings are understood by me then she can more readily listen to herself’’) (Shostrum, 1965). Bohart, Elliott, Greenberg and Watson (2002) offered a similar explanation for the positive therapeutic effects of empathy. Our view differs in two ways. First, we suggest that the unconditional positive regard of the therapist will be effective only if it triggers the client’s hopes that indeed she is acceptable. The client does not see herself solely through Rogers’s eyes but through the lens of her own hopes. Second, we argue that the effects of unconditional positive regard and empathy cannot be isolated from one another in the therapeutic encounter, since the client only values acceptance when understood. If the client felt unconditionally accepted but utterly misunderstood, CCCT would likely have a very different effect than it does. In a review of studies on positive regard, Farber and Lane (2002, p. 177) offered considerable documentation that ‘‘. . . there has been a historical confounding in Rogers’s (and his followers) writings among the concepts of ‘warmth,’ ‘respect,’ ‘acceptance,’ ‘openness,’ ‘genuineness,’ and empathy.’’ Bozarth exemplified this tendency when he stated, ‘‘Rogerian empathy is, in fact, inseparable from unconditional positive regard and, ultimately . . . they are the
- 25. same condition’’ (Bozarth, 1998, p. 52). In this paper we have argued that such confabulation is more apparent than real. Empathy in the context of a respectful, genuine unconditional positive regard is not a confabulation of these conditions but a novel gestalt that is different from its parts. References Bohart, A.C., Elliott, R., Greenberg, L.S., & Watson, J.C. (2002). Empathy. In J. Norcross (Ed.), Psychotherapy relationships that work: Therapists’ relational contributions to effective psychotherapy (pp. 89–108). New York: Oxford University Press. Bozarth, J. (1998). Person-centered therapy: A revolutionary paradigm. Ross-on-Wye, UK: PCCS Books. Bozarth, J., & Wang, C. (2008). The ‘‘unitary actualizing tendency’’ and congruence in client- centered theory. In B. Levitt (Ed.), Reflections on human potential (pp. 102–115). Ross-on- Wye, UK: PCCS Books. Brink, D.C., & Farber, B.A. (1996). A scheme of Rogers’ clinical responses. In B. A. Farber, D. C. Brink, & P. M. Raskin (Eds.), The psychotherapy of Carl Rogers (pp. 15–24). New York: Guilford Press. Brodley, B. (2005). About the non-directive attitude. In B. Levitt (Ed.), Embracing non-
- 26. directivity (pp. 1–4). Ross-on-Wye, UK: PCCS Books. Cain, D.J. (2010). Person-centered psychotherapies. Washington, DC: American Psychological Association. Farber, B.A. (2007). On the enduring and substantial influence of Carl Rogers’ not-quite necessary or sufficient conditions. Psychotherapy, Theory, Research, Practice, Training, 44, 289–294. Person-Centered & Experiential Psychotherapies 213 Farber, B.A., & Lane, J.S. (2002). Effective elements of the therapy relationship: Positive regard. In J. Norcross (Ed.), Psychotherapy relationships that work: Therapist contributions and responsiveness to patients (pp. 175–194). New York: Oxford University Press. Freud, S. (1966). Introductory lectures on psychoanalysis. New York: W.W. Norton and Co. Hill, C.E., & Knox, S. (2002). Self-disclosure. In J.C. Norcross (Ed.), Psychotherapy relationships that work (pp. 255–266). New York: Oxford University Press. Kirschenbaum, H. (1979). On becoming Carl Rogers. New York: Delta. Lazarus, A.A. (2005). Multimodal therapy. In J.C. Norcross & M.R. Goldfried (Eds.), Handbook of psychotherapeutic integration (pp. 105–120). New
- 27. York: Oxford University Press. Malcolm, J. (1990). The journalist and the murderer. New York: Vintage Press. Mearns, D., & Thorne, B. (1999). Person-centred counselling in action. London: Sage. Prochaska, J.O., & Norcross, J.C. (2003). Systems of psychotherapy. New York: Brooks-Cole. Rachlin, H. (1994). Behavior and mind. New York: Oxford University Press. Rice, L. (1974). The evocative function of the therapist. In D. Wexler & L. Rice (Eds.), Innovations in client-centered therapy (pp. 289–311). New York: John Wiley. Rogers, C.R. (1942). Counseling and psychotherapy. Boston: Houghton Mifflin. Rogers, C.R. (1951). Client-centered therapy. Boston: Houghton Mifflin. Rogers, C.R. (1957). The necessary and sufficient conditions of therapeutic personality change. Journal of Consulting Psychology, 21, 95–103. Rogers, C.R. (1959). A theory of therapy, personality, and interpersonal relationships as developed in the client-centered framework. In S. Koch (Ed.), Psychology: A study of science. Vol. 3: Formulations of the person and the social context (pp. 184–256). New York: McGraw-Hill. Sereny, G. (1995). Into that darkness. London: Pimlico. Shlien, J. (1997). Empathy in psychotherapy: A vital mechanism? Yes. Therapist’s conceit? All
- 28. too often. By itself enough? No. In A.C. Bohart & L.S. Greenberg (Eds.), Empathy reconsidered: New directions in psychotherapy (pp. 63–80). Washington, DC: American Psychological Association. Shostrom, E. (Ed.). (1965). Client-centered therapy. In Three approaches to psychotherapy [Film]. Orange, CA: Psychological Films. Van den Berg, J. (1974). A divided existence and complex society: An historical approach. Pittsburgh, PA: Duquesne University Press. 214 M. Frankel et al. Copyright of Person-Centered & Experiential Psychotherapies is the property of PCCS Books Ltd. and its content may not be copied or emailed to multiple sites or posted to a listserv without the copyright holder's express written permission. However, users may print, download, or email articles for individual use. Patient Education and Counseling 81 (2010) 362–367 Structured contraceptive counseling—A randomized controlled trial Aileen M. Langston *, Linette Rosario, Carolyn L. Westhoff
- 29. Division of Family Planning and Preventive Services, Department of Obstetrics and Gynecology, Columbia University Medical Center, New York, USA A R T I C L E I N F O Article history: Received 10 February 2010 Received in revised form 30 July 2010 Accepted 4 August 2010 Keywords: Contraceptive counseling Unintended pregnancy Abortion Contraception Birth control Structured counseling A B S T R A C T Objective: To evaluate the addition of structured contraceptive counseling to usual care on choice, initiation, and continuation of very effective contraception after uterine aspiration.
- 30. Methods: We conducted a RCT of a version of the WHO Decision-Making Tool for Family Planning Clients and Providers with women having a procedure for a spontaneous or induced abortion. Our intervention provided structured, standardized counseling. We randomized women to usual care or usual care with structured counseling. Our outcomes included choosing a very effective contraceptive method and 3 months continuation. Results: Fifty-four percent of all participants chose a very effective method. Women in the intervention group were no more likely to choose a very effective method (OR 0.74, 95% CI 0.44, 1.26) or to initiate their method compared to the usual care group (OR 0.65, 95% CI 0.31, 1.34). In multivariate models, structured counseling was not associated with using a very effective method at 3 months (AOR 1.06, 95% CI 0.53, 2.14). Conclusion: In this setting, structured counseling had little impact on contraceptive method choice, initiation, or continuation. Practice implications: Adding structured counseling did not increase the proportion choosing or
- 31. initiating very effective contraception in a practice setting where physicians already provide individualized counseling. � 2010 Elsevier Ireland Ltd. All rights reserved. Contents lists available at ScienceDirect Patient Education and Counseling journa l homepage: www.e lsev ier .com/ locate /pateducou 1. Introduction Despite the availability of very effective contraceptive methods, the rate of unintended pregnancy in the United States (US) remained stagnant at 49% from 1995 to 2001 [1]. Most women in the US have not used the most effective methods available [2], and 47% have had a repeat abortion [3]. Women’s health professionals have regarded counseling as an important component of improv- ing contraceptive use [4], and access to counseling services has been considered an integral part of informed choice [5]. The World Health Organization (WHO) has supported the practice of contraceptive counseling so that patients can make informed decisions in conjunction with their provider [6]. Accepted practice within contemporary healthcare has been to offer patients information regarding diagnoses and proposed treatment options. Contraceptive counseling, where options are presented with mechanisms of action, efficacy, risks and benefits,
- 32. has been a challenge due to the limited resources in the clinical * Corresponding author at: Division of Family Planning and Preventive Services, Columbia University Medical Center, 622 West 168th Street, PH 1669, New York, NY 10032, USA. Tel.: +1 212 305 4805; fax: +1 212 305 6438. E-mail address: [email protected] (A.M. Langston). 0738-3991/$ – see front matter � 2010 Elsevier Ireland Ltd. All rights reserved. doi:10.1016/j.pec.2010.08.006 setting and the ability of any person to receive and comprehend a large amount of information. A recent Cochrane Review found that ‘‘little evidence from randomized controlled trials supports the hypothesis that counseling improves contraceptive use,’’ and a systematic review of the literature on counseling to prevent unintended pregnancy also [7] found limited evidence regarding its effectiveness [8]. In 1996 the US Preventive Services Task Force (USPSTF) recom- mended contraceptive counseling, but the 2002 USPSTF withdrew this recommendation due to insufficient evidence [9,10]. Limited data has suggested a possible benefit to using structured counseling—consisting of audio–visual materials with standardized information—for contraceptive counseling. Two randomized controlled trials (RCTs) utilized structured audio– visual educational material with standardized information about
- 33. contraceptive methods. The results from both studies showed increased contraceptive use or continuation of effective contracep- tive methods (pill and injection) 1 year later [11,12]. In a post-abortion population, one RCT of counseling performed by a contraceptive specialist along with advanced provision of contraceptive methods compared to routine counseling found increased uptake of long acting reversible contraceptives and increased continuation at 4 months but no difference in repeat abortion rates at 2 years [13]. The information given by the http://dx.doi.org/10.1016/j.pec.2010.08.006 mailto:[email protected] http://www.sciencedirect.com/science/journal/07383991 http://dx.doi.org/10.1016/j.pec.2010.08.006 A.M. Langston et al. / Patient Education and Counseling 81 (2010) 362–367 363 specialist counselor in this study was not standardized or given in a structured audio-visual format. In an attempt to meet family planning counseling needs, the WHO developed a series of family planning guidelines and tools, including the Decision-Making Tool for Family Planning Clients and Providers (DMT) [14]. A double-sided flipchart with one side for the client to aid in decision-making and the other side for the provider to aid in the counseling process by giving information and guidance, this tool was studied for improving communication
- 34. with clients in limited resource settings [15,16]. The DMT was found to improve communication, particularly with clients choosing a new contraceptive method [15]. Given the need for resource efficiency in health care, the belief by many providers and organizations that contraceptive counsel- ing is necessary and worthwhile, and the limited literature [7– 10,17], we aimed to study this topic using a structured and standardized counseling intervention based on the DMT in a post- abortion setting with most modern methods available for immediate initiation. Our study evaluated structured, standard- ized contraceptive counseling for its influence on participants choosing a very effective contraceptive method at the time of first trimester vacuum aspiration, method initiation, and 3 months and 6 months method continuation. 2. Methods 2.1. Setting and participants From December 2008 to July 2009, we enrolled participants from a family planning referral clinic to a private practice setting serving a predominantly Hispanic (Dominican) population with Medicaid coverage in New York City. Providers at the practice were all physicians: faculty, fellows, and residents at Columbia University Medical Center (CUMC). Vacuum aspiration procedures were offered 1 day per week, and on a given day, 3–4
- 35. physicians each cared for 6–8 patients. The study population consisted of women seeking a first trimester procedure for a spontaneous or induced abortion. Inclusion criteria were (1) age� 18 years, (2) no desire to become pregnant right away, (3) fluency in Spanish or English, and (4) access to a telephone. The CUMC Institutional Review Board approved this study. 2.2. Structured contraceptive counseling intervention In this study we sought to address whether structured, standardized, non-directive counseling (the intervention) in the setting where contraceptive methods are immediately available and the women have confirmed fertility, will result in increased choosing of very effective contraceptive methods, method initiation, and method continuation at 3 months. Structured counseling consisted of the trained research coordinator reading and displaying a contraceptive flipchart in its entirety to the participant in a private office with samples of each method available for patients to see and touch. The counseling was structured in that the format included visual and audio components allowing the participant to both visualize and hear the information. The counseling was standardized in that the same information was presented every time the counseling was performed. Participants were encouraged to ask questions and to write down questions for their physician on
- 36. supplied note cards. The research assistants were trained to answer questions using only the information from the flipchart. If a question was not able to be answered by the information on the flipchart, the research assistant was instructed to request the participant ask her provider this question during usual care. The flipchart was a version of the WHO 2005 Decision-Making Tool for Family Planning Clients and Providers (DMT) [14]. We did not intend the intervention to provide tailored counseling, though that is one of the common uses of the DMT. We chose to use the format of the DMT for its ready-made structure, simple language and images to create our structured and standardized intervention. We utilized the portion of the DMT focused on choosing a method and the method tabs (overview and information for choice, medical eligibility criteria, possible side effects, how to use, when to start, and what to remember). We modified this portion of the DMT to add methods available in the US (patch, ring, levonorges- trel IUD, and etonogestrel implant) and to remove information about methods not available in the US (NET-EN injections, monthly injections, and Norplant) or not appropriate for post procedure patients (lactational amenorrhea and fertility awareness). Thus the flipchart administered by a research coordinator gave our intervention a structured format with visual and audio compo-
- 37. nents. The research coordinators gave standardized information using this structured tool. The simple language and images in the flipchart, as well as reading the pages aloud as they were viewed, mitigated any effects of low literacy. Information on contraceptive methods (female sterilization, male sterilization, copper IUD, levonorgestrel IUD, etonogestrel implant, depo provera injection, ring, patch, pill, and condom) was presented on 5–7 double- sided pages per method with patient and counselor focused content on the front and back, respectively. We used flipcharts printed in English for our participants who preferred English and flipcharts translated and printed in Spanish for our participants who preferred Spanish. The flipchart included information on con- traceptive effectiveness, how to use each method, possible side effects, and when to seek help. Usual care consisted of a single physician performing the medical history, physical exam, ultrasound, obtaining informed consent for the suction aspiration procedure, and carrying out this procedure for each patient. This visit required about one hour to complete. Contraceptive counseling was routinely offered by the physician as well and was embedded in the visit. As part of usual care, the content and duration of contraceptive counseling performed by the provider was left to their discretion. 2.3. Study procedures Two research coordinators fluent in English and Spanish performed enrollment and follow-up. We used training scripts
- 38. and role play to standardize interactions with participants. Questionnaires were piloted and adjusted based on responses prior to enrollment. We assessed all women aged 18 or older registered in the clinic for eligibility. To ease anxiety, the coordinator first gave each patient basic information about routine clinic procedures before discussing the study. Interested and eligible women were consented. A baseline questionnaire was administered to collect demographic characteristics as well as partnership, reproductive, and contraceptive histories. Participants were then randomized to usual care with intervention versus usual care alone. Those randomized to the intervention group received structured counseling by a coordinator immediately prior to usual care during the same visit. Attention was paid to minimize delay for women in the intervention group. Using a random-number table, we determined the sequence for 1:1 allocation constrained by blocks of 10. Randomization assignments were sealed inside numbered, opaque envelopes. The coordinator opened the next sequentially numbered envelope after completing informed consent. No blinding of participants or coordinators was feasible due to the nature of the intervention. Physician-providers did not know the participant’s allocation group, did not discuss the study with patients, and were asked not to change their counseling. A.M. Langston et al. / Patient Education and Counseling 81 (2010) 362–367364
- 39. Contraceptive methods available to participants immediately following their procedure included intrauterine devices (IUDs), implants, injections, rings, and pills. The IUDs and implants were donated and available at no cost to all clinic patients. All participants had either New York State Medicaid coverage for prescription contraceptives or access to additional free supplies at a safety net clinic so all contraceptives offered were available free of charge. The patch was available by prescription only and sterilization by referral only. Those who chose pill or ring received either a prescription or a 1-month supply and prescription. All participants received condoms with handouts on emergency contraception and condom use. After each enrollment day, we reviewed charts to confirm that a procedure was performed and to identify the contraceptive method chosen as well as whether initiation was immediate or delayed. Coordinators called participants 3 months after enroll- ment to assess contraceptive use. A subset of patients received 6 months follow-up phone calls. Initial analysis of the first 101 participants to complete both 3 and 6 months data found no significant differences, so 6 months follow-up was stopped to focus on maximizing 3 months follow-up. 2.4. Outcomes and analysis The primary outcome of this study was proportion of participants choosing a very effective contraceptive method. Secondary outcomes were method initiation on the day of the procedure and method continuation of very effective and/or effective methods at 3 months, and at 6 months for the sub- group
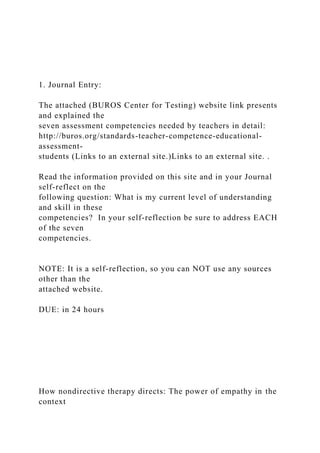
- 40. for whom we collected data. The WHO defined very effective contraceptive methods as those with 1 year typical use pregnancy rates of <1% (sterilization, IUDs, and implants) [6]. Effective methods have typical use pregnancy rates of 1–9% (pills, rings, patches, and injections). The WHO defined additional categories for methods with �10% and >25% typical use pregnancy rates. In this study, we used the WHO [(Fig._1)TD$FIG] Fig. 1. Participant enrollment and follow-up in a randomized con definition for very effective and effective methods and defined less effective methods as those with �10% pregnancy rate (condoms, withdrawal, periodic abstinence, and no method). We defined initiation of effective and very effective methods as leaving the clinic with a method requiring no healthcare provider contact to begin use. If a participant requested pills and left clinic with a pill pack and a prescription, this was coded as immediate initiation. If she left with a prescription only, this was considered delayed initiation because she needed to go to a pharmacy to begin using the method. Less effective contraceptive methods (condoms, withdrawal, and periodic abstinence) were coitally dependent and, therefore, were not able to be initiated in the clinic.
- 41. We defined continuation as using a contraceptive method at 3 or 6 months that was in the same effectiveness group as the method requested at enrollment. For example, two patients requested sterilization and were using an IUD at the 3 months follow-up interview. Both these participants were counted as ‘continuers’ for the very effective group. In this clinic in 2003–2004, 29% of patients chose the most effective available methods (injection, copper IUD, or sterilization) following a first trimester aspiration procedure [18]. We designed our study to identify an increase from 30% to 50% of women requesting a very effective method in the intervention arm. With up to 20% loss due to exclusion after randomization, a two- sided alpha of .05, and power of .80, we needed 125 women in each arm. We used SAS, version 9.2 (SAS Institute, Cary, NC) for statistical analyses to compare the intervention and control groups. We performed Chi-square analyses to assess differences between allocation groups. We calculated two-sided p-values and 95% confidence intervals. We performed logistic regression analyses with two dependent outcomes: very effective method use at 3 months; or very effective or effective method use at 3 months. The 8 participants who reported sexual abstinence since enrollment due to no partner were excluded from these analyses. We performed univariate logistic regression with (1) intervention, (2) immediate initiation, (3) age, (4) education, (5) ethnicity, (6) trolled trial of structured contraceptive counseling, NY 2009.
- 42. Table 2 Structured contraceptive counseling versus usual care: contraceptive method chosen and 3 months continuation. Intervention (N = 114) Usual care (N = 108) Total (N = 222) p-Value* Contraceptive method chosen Very effective methodsa 57 (50%) 62 (58%) 119 (54%) 0.27 Effective methodsa 48 (42%) 37 (34%) 85 (38%) 0.27 Less effective methodsa 9 (8%) 9 (8%) 18 (8%) 1.0 (N = 89) (N = 83) (N = 172b) 3 months continuation Very effective methodsc 41/48 (85%) 40/52 (77%) 81/100 (81%) 0.28
- 43. Effective methodsc 28/41 (68%) 21/31 (68%) 49/72 (68%) 0.96 * Chi-square p-value. a Very effective methods—copper IUD, levonorgestrel IUD, etonogestrel implant, sterilization. Effective methods—DMPA, ring, patch, pill. Less effective methods— intervention group: 1 undecided, 2 abstinence, 2 declined contraception, 4 condoms. Control group: 3 undecided, 1 natural family planning, 1 coitus interruptus, 1 declined contraception, 3 condoms. b Less effective methods are not represented in this total. c Numerators are continuers and denominators are those who chose this method group and completed 3 months follow-up. A.M. Langston et al. / Patient Education and Counseling 81 (2010) 362–367 365 parity, (7) prior abortion, (8) stable relationship status, (9) provider and (10) current smoking. Variables were chosen for multivariate logistic regression based upon univariate results and overall importance to the clinical outcome. We constructed the final model using the likelihood ratio test as variables were added sequentially to determine the most parsimonious model. The Hosmer–Lemeshow statistic was calculated to test the goodness- of-fit of the final model.
- 44. 3. Results 3.1. Enrollment We screened 380 women and enrolled 250 women (Fig. 1). We excluded 28 women after randomization because they did not have a procedure that day primarily due to pregnancies in the second trimester, completed spontaneous abortions, and ectopic pregnancies. The remaining 222 women were eligible for analysis and follow-up. The groups were well balanced with regard to baseline characteristics (Table 1). They were mainly Hispanic and in stable relationships, defined as a relationship the participant reported will continue for >1 year. Participants’ ages ranged from 18 to 45 years with a mean age of 26.2 years. Participants were seeking induced abortion (94%) or spontaneous abortion management (6%). The time used to conduct the structured counseling intervention was, on average, 20 min (standard deviation �8 min). 3.2. Methods requested The intervention and control groups were similar in the methods requested (Table 2). Participants in the intervention group were similar to the usual care group in often choosing a very effective method (OR 0.74, 95% CI 0.44, 1.26). Most women requested very effective methods (levonorgestrel IUD (27%), copper IUD (15%), implant (9%) and sterilization (2%)). Many women requested effective methods (oral contraceptive pills (18%), vaginal ring (9%), injection (7%), and patch (5%)). Fewer
- 45. women requested less effective methods (undecided/declined (n = 7), condoms (n = 7), abstinence (n = 2), withdrawal (n = 1) and periodic abstinence (n = 1)). Comparing the demographics of participants who chose very effective methods to those who did not, parous women and women in a stable relationship were more likely to choose a very effective method (OR 2.51, 95% CI 1.35, 4.67 and OR 1.98, 95% CI 1.11, 3.54, Table 1 Demographics and reproductive history—structured contraceptive counseling versus usual care (N = 222). Intervention (N = 114) N (%) Usual care (N = 108) N (%) Age (SD) 25.6 (5.7) 26.8 (6.7) Age<25 years 59 (52%) 49 (45%) Hispanica 98 (87%) 97 (90%) Education�12th grade 74 (65%) 77 (71%) Birthplace United States 47 (41%) 43 (40%)
- 46. Dominican Republic 50 (44%) 53 (49%) Other 17 (15%) 12 (11%) Current smokersb 20 (18%) 20 (19%) Gravida>1 98 (86%) 96 (89%) Parous 84 (74%) 81 (75%) Ever had a prior abortion 57 (50%) 58 (54%) Ever used contraception 109 (96%) 104 (96%) Current stable relationship 78 (68%) 77 (71%) a One missing value from intervention group. b One missing value from intervention group. respectively). Six providers saw the majority (91%) of the participants. No differences were seen in the methods requested (p = 0.44) or the proportion of methods initiated immediately (p = 0.83) among these providers. There was no difference between the intervention and control groups in the physician-providers from whom they received usual care (p = .59). 3.3. Immediate versus delayed initiation Participants in the intervention group were not more likely to initiate the requested method immediately compared to those in the usual care group (OR 0.65, 95% CI 0.31, 1.34) (Table 2). Only 15 percent of participants chose a method that could not be initiated the same day (18 less effective methods, 10 patches, and 5
- 47. sterilizations). The other 189 participants selected a method that could be initiated the same day; 80% of these women initiated their method the same day (80 IUDs, 28 pills, 19 implants, 15 injections, and 10 rings). The remaining 20% of participants had delayed initiation of their method (14 IUDs, 11 pills, 10 rings, 1 injection, and 1 implant). Of these, 3 women preferred to delay IUD insertion, and 1 woman wanted to obtain her pill prescription from her personal physician. The physician-providers delayed 9 initiations due to infection, 2 due to bleeding, and 1 due to lack of confirmatory products of conception at the time of the procedure. Twenty-one women were given prescriptions only (10 rings, and 11 pills). 3.4. Follow-up and continuation Of 222 participants, 186 (84%) completed 3 months follow-up (Fig. 1). Loss to follow-up was equal between the intervention and control group. The baseline characteristics and requested methods of the women who completed 3 months follow-up and those who did not were similar (data not shown). Those in the intervention group who completed 3 months follow-up had chosen similar methods compared to those in the control group (p = 0.51). No participants reported a repeat pregnancy at 3 months. For those who chose a very effective or effective method, 3 months continuation of the requested method and 3 months continuation of immediately initiated methods were not signifi- cantly different comparing the intervention group to the usual
- 48. care group (OR 1.24, 95% CI 0.62, 2.50 and OR 1.43, 95% CI 0.58, 3.52, respectively) (Table 2). Fourteen (78%) participants who chose a less effective method completed 3 months follow-up; 13 reported being sexually active; and only 2 reported adopting an effective Table 3B Predictors of contraceptive method use at 3 months, multivariate model (N = 186). Very effective method use Very effective or ef- fective method use AOR 95% CI AOR 95% CI Structured counseling 1.06 (0.53, 2.14) 1.59 (0.77, 3.28) Immediate initiation 15.5 (6.02, 39.7) 4.26 (2.05, 8.87) Age 0.91 (0.43, 1.89) 1.67 (0.81, 3.47) Education – – – – Prior abortion – – – – Parous 3.17 (1.37, 7.32) – –
- 49. Hispanic – – – – Relationship – – – – Smoking – – – – *Excluded participants abstinent since enrollment from the analysis (N = 8). **The reference group is ‘no’ and the comparison group is ‘yes’ except for age where reference group is <25 years and comparison group is �25 years. A.M. Langston et al. / Patient Education and Counseling 81 (2010) 362–367366 method (pills). In a sub-group analysis of those who initiated a very effective method on the day of enrollment (n = 83), the interven- tion group trended towards increased 3 months continuation compared to the usual care group (98% versus 83%; p = .06). With the initial participants at the start of the study, we took the opportunity to conduct 6 months follow-up interviews. We completed 6 months follow-up with 131 (59%) participants. For these participants, 6 months continuation between the inter- vention group (67%) and the usual care group (68%) was similar (OR 0.95, 95% CI 0.45, 2.02). Two participants reported a repeat pregnancy at 6 months, one from each randomization group. 3.5. Predictors of using a very effective and/or effective method at 3
- 50. months When limiting our outcome to using a very effective method at 3 months, the counseling intervention did not have a strong effect in univariate or multivariate models (Tables 3A and 3B). In univariate analyses, completing at least the 12th grade in school and immediate initiation of a requested contraceptive method had the strongest associations with using a very effective or effective method at 3 months (Table 3A). In a multivariate model, the counseling intervention did not have a strong association with using a very effective or effective method at 3 months (AOR 1.59, 95% CI 0.77, 3.28). 4. Discussion and conclusion 4.1. Discussion We sought to address whether structured, standardized, non- directive counseling (the intervention) in the setting where contraceptive methods are immediately available and the women have confirmed fertility, will result in increased choosing of very effective contraceptive methods. We specifically chose a counsel- ing format that would not be performed by a physician to reflect the reality of limited health resources and the common practice of family planning clinics in the US to utilize non-physicians to perform counseling. We chose standardized counseling in contrast to tailored counseling to ensure that participants in the interven-
- 51. tion group received the same information to minimize bias from the counselor. Minority women have been shown to be more likely to receive contraceptive and sterilization counseling compared to white women [19], and our clinic serves a predominantly minority population. We performed a RCT of an intervention utilizing a modified version of a readily reproducible counseling intervention (DMT) Table 3A Predictors of method use at 3 months, univariate analyses (N = 186). Very effective method use Very effective or effective method use OR 95% CI OR 95% CI Structured counseling 0.97 (0.53, 1.74) 1.35 (0.68, 2.68) Immediate initiation 14.02 (5.58, 35.22) 3.87 (1.90, 7.89) Age 1.05 (0.58, 1.89) 1.44 (0.73, 2.86) Education 1.65 (0.87, 3.14) 2.11 (1.04, 4.25) Prior abortion 0.91 (0.50, 1.64) 1.62 (0.82, 3.22)
- 52. Parous 2.43 (1.19, 4.95) 1.37 (0.65, 2.89) Hispanic 0.86 (0.33, 2.24) 1.46 (0.52, 4.10) Relationship 1.38 (0.72, 2.65) 1.10 (0.53, 2.29) Smoking 0.77 (0.35, 1.69) 1.12 (0.46, 2.74) *Excluded participants abstinent since enrollment from the analysis (N = 8). **The reference group is ‘no’ and the comparison group is ‘yes’ except for age where reference group is <25 years and comparison group is �25 years. that is available online and developed by experts. Our structured and standardized counseling intervention did not result in more women choosing a very effective contraceptive method, immedi- ately initiating more methods, or significantly increasing 3 months continuation of their chosen method in our setting. In our clinic, physicians who specialize in family planning are providing contraceptive counseling with the patients as an integrated part of their visit for a first trimester uterine aspiration. Additional counseling may have been unnecessary in this setting. Our study had several limitations. Our clinic setting had specialized providers as well as a specific ethnic demographic that limited the generalizability of our study’s findings. We utilized the DMT for structured, standardized counseling, and it was
- 53. designed for tailored counseling. This approach may have affected the effectiveness of the intervention. Our 3 months contraceptive data was self-reported and vulnerable to social desirability bias. We made an effort to reduce patients’ anxiety but could not eliminate it before the intervention. This anxiety could have lessened the effects of the structured counseling intervention. A further limitation was that the providers in our setting were aware of the study and could have altered their counseling during the study, minimizing the effect of the intervention, though they were asked not to do so. We also did not collect data on participant satisfaction specifically with the contraceptive counseling or detailed data on participants’ desires for future pregnancy beyond whether they desired contraception. One further limitation of our study was that it was powered for the outcome of choosing a very effective contraceptive method; however, it was not powered for the other outcomes collected— initiation and continuation. The initiation outcome for very effective methods was so similar between the intervention and control groups (84% versus 82%, respectively) that, though underpowered, the trend showed no difference. The continuation outcome for very effective methods was less similar between the two groups (85% versus 77%, respectively). A larger sample size could have benefited this outcome in our study. We had a very high proportion of patients in both the intervention and control group who chose IUDs (42%) compared
- 54. to the 2% of contracepting women using IUDs in the US in 2002 [20]. Hispanic women in the US have been found to have higher ever-use of IUDs (10.0%) and implants (4.0%) compared to non- Hispanic White (4.7% and 1.4%) and non-Hispanic Black (5.5% and 3.2%) women [20]. The community served by our practice is predominantly Hispanic, and greater baseline usage of these long- acting methods among Hispanic women could partially explain the high proportion of women choosing an IUD. In one study of post- abortion contraception, 53% chose the pill, 11% chose the IUD, 8% chose DMPA and 17% declined or were undecided on the day of A.M. Langston et al. / Patient Education and Counseling 81 (2010) 362–367 367 their procedure so our findings were not typical though the literature is limited on post-abortion contraceptive use [21]. The proportion of our participants selecting very effective methods was also higher than found in the same population and setting in 2003– 2004—54% compared to 29% [18]. The larger than expected proportion of women in the control group who chose a very effective method was an unexpected outcome and decreased the power for our sample size. The physicians and patients participating in this study may have been further motivated by the fact that these very effective contraceptive methods were available for insertion on the same day as the procedure. Previously in this same clinic, patients
- 55. who chose a very effective method had to make an additional visit on a different day to have the method initiated. Immediate access to very effective contraceptives following an abortion has been shown to decrease repeat abortion [22,23]. The intervention to increase uptake of very effective post-abortion contraception may be to provide increased access to contraceptives while the specific counseling methods may be less significant as long as contracep- tive counseling is provided. Interventions to improve contracep- tive uptake and use to better meet family planning needs deserve continued study. 4.2. Conclusion Contraceptive counseling is valuable. The exact amount and extent of counseling appropriate for each patient likely varies though a common minimum should be standard to give patients the opportunity to make an informed choice. All our patients received contraceptive counseling by the physician doing their procedure with the structured counseling done in addition if they were part of the intervention group. Due to a higher than expected proportion choosing a very effective method in the control group, our power was less than planned and needs to be considered in the interpretation of our outcomes. Structured contraceptive counseling in our setting did not have a significant impact on method choice, method initiation, or 3 months continuation. Interventions to improve contraceptive use deserve continued study. 4.3. Practice implications
- 56. Adding structured contraceptive counseling did not increase the proportion choosing or initiating a very effective contraceptive method in a practice setting where specially trained physicians already provide informal individualized counseling. Conflict of interest None. Acknowledgements The authors acknowledge Heidi Jones and Sara Fuentes, Division of Family Planning and Preventive Services, Columbia University and Sarah Johnson, Department of Reproductive Health and Research, WHO. Financial support provided by a grant from an anonymous foundation. This foundation approved the study design. It did not have a direct role in the collection, analysis and interpretation of data; the writing of the manuscript; or the decision to submit the manuscript for publication. References [1] Finer LB, Henshaw SK. Disparities in rates of unintended pregnancy in the United States, 1994 and 2001. Perspect Sex Reprod Health 2006;38:90–6. [2] Frost JJ, Darroch JE. Factors associated with contraceptive choice and incon-
- 57. sistent method use United States, 2004. Perspect Sex Reprod Health 2008;40:94–104. [3] Henshaw SK, Kost K. Trends in the characteristics of women obtaining abor- tions, 1974 to 2004. New York: Guttmacher Institute; 2008. [4] Landry DJ, Wei J, Frost JJ. Public and private providers’ involvement in improving their patients’ contraceptive use. Contraception 2008;78:42–51. [5] EngenderHealth. Choices in family planning: informed and voluntary decision making: realizing rights in sexual and reproductive health services. New York: Automated Graphic Systems Inc.; 2003. [6] World Health Organization Department of Reproductive Health and Research (WHO/RHR) and Johns Hopkins Bloomberg School of Public Health/Center for Communications Programs (CCP) IP. Family planning: a global handbook for providers. Baltimore and Geneva: CCP and WHO; 2007. [7] Halpern V, Grimes DA, Lopez L, Gallo MF. Strategies to improve adherence and acceptability of hormonal methods for contraception. Cochrane Database Syst Rev 2006. CD004317. [8] Moos MK, Bartholomew NE, Lohr KN. Counseling in the clinical setting to prevent unintended pregnancy: an evidence-based research
- 58. agenda. Contra- ception 2003;67:115–32. [9] Westhoff CL, Personal communication from third author; 2009 [10] USPSTF. Guide to clinical preventive services, 2nd ed., Baltimore: Williams and Wilkins; 1996. [11] Canto De Cetina TE, Canto P, Ordonez Luna M. Effect of counseling to improve compliance in Mexican women receiving depot- medroxyprogesterone ace- tate. Contraception 2001;63:143–6. [12] Danielson R, Marcy S, Plunkett A, Wiest W, Greenlick MR. Reproductive health counseling for young men: what does it do? Fam Plann Perspect 1990;22:115– 21. [13] Schunmann C, Glasier A. Specialist contraceptive counselling and provision after termination of pregnancy improves uptake of long-acting methods but does not prevent repeat abortion: a randomized trial. Hum Reprod 2006;21:2296–303. [14] World Health Organization and the INFO Project JHBSoPHCfCP. Decision- making tool for family planning clients and providers. Baltimore and Geneva: Bloomberg School of Public Health and WHO; 2005.
- 59. [15] Kim YM, Davila C, Tellez C, Kols A. Evaluation of the World Health Organiza- tion’s family planning decision-making tool: improving health communica- tion in Nicaragua. Patient Educ Couns 2007;66:235–42. [16] Kim YM, Kols A, Martin A, Silva D, Rinehart W, Prammawat S, et al. Promoting informed choice: evaluating a decision-making tool for family planning clients and providers in Mexico. Int Fam Plan Perspect 2005;31:162– 71. [17] Ferreira AL, Lemos A, Figueiroa JN, de Souza AI. Effectiveness of contraceptive counselling of women following an abortion: a systematic review and meta- analysis. Eur J Contracept Reprod Health Care 2009;14:1–9. [18] Madden T, Westhoff C. Rates of follow-up and repeat pregnancy in the 12 months after first-trimester induced abortion. Obstet Gynecol 2009;113:663– 8. [19] Borrero S, Schwarz EB, Creinin M, Ibrahim S. The impact of race and ethnicity on receipt of family planning services in the United States. J Womens Health (Larchmt) 2009;18:91–6. [20] Mosher WD, Martinez GM, Chandra A, Abma JC, Willson SJ. Use of contracep- tion and use of family planning services in the United States: 1982–2002. Adv Data 2004;1–36.
- 60. [21] Bianchi-Demicheli F, Perrin E, Bianchi PG, Dumont P, Ludicke F, Campana A. Contraceptive practice before and after termination of pregnancy: a prospec- tive study. Contraception 2003;67:107–13. [22] Goodman S, Hendlish SK, Reeves MF, Foster-Rosales A. Impact of immediate postabortal insertion of intrauterine contraception on repeat abortion. Con- traception 2008;78:143–8. [23] Heikinheimo O, Gissler M, Suhonen S. Age, parity, history of abortion and contraceptive choices affect the risk of repeat abortion. Contraception 2008;78:149–54. Structured contraceptive counseling-A randomized controlled trialIntroductionMethodsSetting and participantsStructured contraceptive counseling interventionStudy proceduresOutcomes and analysisResultsEnrollmentMethods requestedImmediate versus delayed initiationFollow-up and continuationPredictors of using a very effective and/or effective method at 3 monthsDiscussion and conclusionDiscussionConclusionPractice implicationsConflict of interestAcknowledgementsReferences