Ventouse delivery
•Descargar como PPTX, PDF•
13 recomendaciones•9,181 vistas

ventouse delivery, vacuum delivery techniques , indication and complications

Recomendados
Más contenido relacionado
La actualidad más candente
La actualidad más candente (20)
Similar a Ventouse delivery
Similar a Ventouse delivery (20)
Más de Datta meghe institute of medical sciences
Más de Datta meghe institute of medical sciences (16)
Último
Último (20)
Ventouse delivery
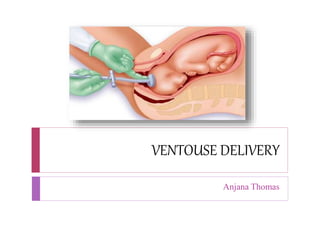
- 2. Description It is an instrumental device designed to assist delivery by creating a vacuum (negative pressure) between itself and the fetal scalp.
- 3. Definition Vaccum extraction also known as ventouse, is a method to assist delivery of a baby using a vacuum device. It is a instrumental delivery to assist delivery by creating a vaccum between it and the fetal scalp.
- 4. Equipment Description Vacuum extractor is composed of: A specially designed cup with a diameter of 3,4,5,6 cm or 30,40,50,60 mm. A rubber tube attaching the cup to a glass bottle with a screw in between to release the negative pressure. A manometer fitted in the mouth of the glass bottle to declare the negative pressure. Another rubber tube connecting the bottle to a suction piece which may be manual or electronic creating a negative pressure that should not exceed- 0.8 kg per cm2
- 5. Part Suction cup of variable sizes. It is either metallic or soft made of silicone . Vacuum generator. Traction tubing.
- 6. Type Malmstrom cup A metal cup to its centre attached a metal chain passed through the rubber tube. The other end of the chain is attached to a handle for traction
- 7. Bird’s cup The suction rubber tube is attached to the periphery of the cup while the handle of traction is attached by a separate short metal chain to the centre of the cup.
- 8. Soft cup It is a bell shaped 6.5 cm diameter soft cup which is made of a firm but supple silastic material.
- 9. Kiwi cup It is fexible stem and low profile cup enable placement over the flexion point of the baby’s head no matter the fetal head position.
- 10. Indications Maternal indication Maternal distress: exhaustion after a long, painful labor due to inefficient uterine contraction. Prolonged second stage of labor. Maternal medical disorders such as heart diseases, HTN and anemia Previous cesarean section or genital prolapse repair. Premature separation of placenta.
- 11. Fetal indication Deep transverse arrest with adequate pelvis. Delay in descend of the high head in case of the second baby of twins. Malposition : occipitolateral and occipito posterior. As an alternative to forceps exept in face presentation and brreech. Fetal distress
- 12. Contraindication Operator inexperience Inability to assess fetal position Suspicion of cephalopelvic disproportion Fetal coagulopathy Preterm babies due to risk of fetal intraventricular hemorrhage. Macrosomia >4kg Soft tissues obstruction in the pelvis Breach presentation and face presentation
- 13. Condition to be fulfilled There should not be any bony resistance below the head The head of a singleton baby should be engaged Cervix should be at least 6 cm dilated.
- 14. Prerequisites Bladder must be emptied Cervix fully dilated No evidence of CPD Vertex presentation and not above the station of +2 Membrane must be ruptured
- 15. Technique Application Station of the head and its position is assessed Instrument is checked to be in working condition before application Selection of cup is important The cup is introduced after retraction of perineum with two fingers of the other hand The centre of the cup should be on the flexion point of the head, which is a point located on the sagittal suture, 3cm in front of posterior fontanelle.
- 16. Traction at this point results in maximum flexion(flexing median application)
- 17. Proper cup placement over flexion point Exclude maternal soft tissue entrapment by palpation
- 18. Vacuum creation by increasing the suction in increments of 0.2 kg/cm2 every 2 mins until 0.8 kg/cm2 A check is made using the fingers round the cup to ensure that no cervical or vaginal tissue is trapped inside the cup . The pressure is gradually raised at the rate of 0.1kg/cm2 per minute until the effective vacuum of 0.8kg/cm2 is achieved in about 10 minutes time The scalp is sucked into the cup and an artificial
- 19. Instrument handle is grasped, and initiation of traction. Traction is initiated by using a two-handed technique, i.e the fingers of one hand are placed against the suction cup, while the other hand grasps the handle of the instrument Traction must be at right angle to the cup Traction directed initially downward then progressively extended upward as head emerge. Traction should be synchronous with the uterine
- 20. Once head is extracted, vacuum pressure is relieved; cup is removed; vaginal delivery followed. The total time from the application until delivery should not exceed 20 minutes. If >20 minutes, the risk of fetal scalp trauma and intracranial damage increases. Many pulls to achieve progress should not be done . The operator should be wiling to abandon the procedure if it does not proceed easily or if the cup dislodges >3 times
- 22. Complications Fetal complications Scalp laceration and bruising Subglial hematoma, Cephalohematoma Intracranial hemorrhage, intraventricular and cerebral hemorrhages Retinal and sub-conjunctival hemorrhages Neonatal jaundice Clavicular fracture, Shoulder dystocia Injury to CVI, CVII nerves, Erb palsy Hypoxia, particularly when extraction has taken a long time and has been difficult Fetal death
- 23. Maternal complications Soft tissues injuries such as cervical tears, annular detachment of the cervix, vaginal tears, perineal lacerations and tears, extension of episiotomy, vaginal wall and perineal hematomas. Traumatic postpartum hemorrhages Infection Genital prolapse
- 24. Management Along with normal delivery management : To assess the effect on the mother and the fetus To start a Ringer’s solution drip and to arrange for blood transfusion, if required To exclude rupture of the uterus To assess if procedure is to be abandoned and consider delivery by cesarean section Laparotomy should be done in a case with rupture of uterus. To administer parenteral antibiotic