2. Pulmonary circulation - FeaturesPulmonary circulation - Features
• 1) Lung is the only organ which
receives the entire cardiac output
(RV) so accommodates a large
amount of blood.
• 2) It is a low pressure and low
resistance system as pulmonary
vessels are highly distensible.
3. Pulmonary artery and itsPulmonary artery and its
characteristicscharacteristics
• 3) The pulmonary artery extends only 5 centimeters
beyond the apex of the right ventricle and then
divides into right and left main branches that supply
blood to the two respective lungs.
• They are thin walled, large diameter and have more
compliance 7 ml/mmHg which is similar to that of
the entire systemic arterial tree.
• This large compliance allows the pulmonary arteries
to accommodate the stroke volume output of the
right ventricle.
4. Pulmonary capillaries and veinsPulmonary capillaries and veins
• 4) Pulmonary capillaries- are larger
than systemic arteries and dense
with multiple anastomosis.
• 5) Pulmonary veins- are highly
distensible and act as blood
reservoirs.
5. Two sources of blood supply to lungsTwo sources of blood supply to lungs
• 6) Two sets of Blood vessels
• A) Pulmonary artery of pulmonary
circulation having deoxygenated blood
and function is gas exchange
• B) Bronchial arteries arising from aorta
of systemic circulation having
oxygenated blood to supply nutrition to
respiratory tree up to terminal
bronchiole.
6. • 7) Pulmonary flow is influenced by intra
thoracic pressure.
• 8) Pulmonary circulation acts as a filter
as it prevents emboli to reach systemic
circulation due to presence of
fibrinolytic system
• they have rapidly tapering ends and act
as sieves to trap the emboli and blood
cells, fat cells, cancer cells, gas bubbles.
7. LymphaticsLymphatics
• 9) Lymph vessels are present in all the
supportive tissues of the lung, beginning in
the connective tissue spaces that surround
the terminal bronchioles, coursing to the
hilum of the lung, and thence mainly into the
right thoracic lymph duct.
• Particulate matter entering the alveoli is
partly removed by way of these channels,
• Plasma protein leaking from the lung
capillaries is also removed from the lung
tissues, thereby helping to prevent
pulmonary edema.
8. • 10) ACE is produced by pulmonary
endothelium cells and it helps to convert
Angiotensin I to Angiotensin II which plays a
major role in maintaining BP.
• 11) Physiologic shunt – Due to broncho -
pulmonary anastomosis it is the bronchial
vessel blood which is not oxygenated in
alveolar capillaries and enters the pulmonary
vein directly and accounts for 1-2 % of
shunted blood in systemic circulation.
• This is also the reason that RV Output is little
less than LV Output.
9.
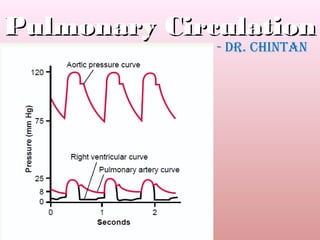
10. Pressures in the pulmonary systemPressures in the pulmonary system
• 1) RV - The systolic pressure in the right ventricle
of the normal human being averages about 25
mm Hg, and the diastolic pressure averages about
0 to 1 mm Hg, values that are only one fifth those
for the left ventricle.
• 2) Pulmonary artery- the systolic pulmonary
arterial pressure averages about 25 mm Hg in the
normal human being, the diastolic pulmonary
arterial pressure is about 8 mm Hg, and the mean
pulmonary arterial pressure is 15 mm Hg.
11. • 3) Pulmonary Capillary Pressure. The mean
pulmonary capillary pressure is about 7 mm
Hg. Rise in this pressure can lead to
pulmonary edema.
• 4) Left Atrial and Pulmonary Venous
Pressures. The mean pressure in the left
atrium and the major pulmonary veins
averages about 2 mm Hg in the recumbent
human being,
• varying from as low as 1 mm Hg to as high as 5
mm Hg.
12. Pulmonary wedge pressurePulmonary wedge pressure
It is usually not possible to measure a human
being’s left atrial pressure using a direct
measuring device because it is difficult to pass
a catheter through the heart chambers into
the left atrium.
However, the left atrial pressure can often be
estimated with moderate accuracy by
measuring the so-called pulmonary wedge
pressure.
13. MethodMethod
• This is achieved by inserting a catheter first
through a peripheral vein to the right atrium,
• then through the right side of the heart and
through the pulmonary artery
• into one of the small branches of the
pulmonary artery,
• finally pushing the catheter until it wedges
tightly in the small branch
14. • The pressure measured through the catheter,
called the “wedge pressure,” is about 5 mm
Hg.
• Because the blood vessels extending beyond
this artery make a direct connection with the
pulmonary capillaries,
• This wedge pressure is usually only 2 to 3 mm
Hg greater than the left atrial pressure.
15. Clinical importance of wedgeClinical importance of wedge
pressurepressure
• When the left atrial pressure rises to high
values, the pulmonary wedge pressure also
rises.
• Therefore, wedge pressure measurements can
be used to clinically study changes in
pulmonary capillary pressure and left atrial
pressure in patients with congestive heart
failure.
16.
17. Blood Volume of lungsBlood Volume of lungs
• The blood volume of the lungs is about 450
milliliters, about 9 per cent of the total blood
volume of the entire circulatory system.
• Approximately 70 milliliters of this pulmonary
blood volume is in the pulmonary capillaries,
and the remainder is divided about equally
between the pulmonary arteries and the
veins.
18. Lungs act as blood reservoirsLungs act as blood reservoirs
• Exchange between pulmonary and systemic
circulation can occur in certain conditions.
• For instance, when a person blows out air so hard
that high pressure is built up in the lungs— such as
when blowing a trumpet—as much as 250 milliliters
of blood can be expelled from the pulmonary
circulatory system into the systemic circulation.
• Also, loss of blood from the systemic circulation by
hemorrhage can be partly compensated for by the
automatic shift of blood from the lungs into the
systemic vessels
19. • Failure of the left side of the heart or
increased resistance to blood flow through
the mitral valve as a result of mitral stenosis
or mitral regurgitation causes blood to dam
up in the pulmonary circulation,
• sometimes increasing the pulmonary blood
volume as much as 100 per cent and causing
large increases in the pulmonary vascular
pressures – pulmonary edema
20.
21. Factors influencing pulmonary bloodFactors influencing pulmonary blood
flow or regulation of itflow or regulation of it
• 1) Cardiac output- Pulmonary blood flow is directly
proportional to cardiac output. So any factors that
alter CO like VR, Force of contraction, etc will affect
it too.
• 2) Pulmonary vascular resistance – inverse
relationship between the two.
• 3) Nervous factors – Sympathetic stimulation – VC –
more resistance --- decrease flow,
• Parasympathetic stimulation - VD - less resistance –
more flow.
22. • 4) Chemical factors- Hypoxia, Hypercapnia, acidosis,
cause VC and increase pulmonary arterial pressure.
• In all other areas other than lung, hypoxia produces
VD.
• This is the reason for the development of pulmonary
HT in patients with COPD.
• Hypoxia causes histological changes in pulmonary
vasculature leading to increase pulmonary vascular
resistance.
23. Hypoxia - VC substanceHypoxia - VC substance
• The low oxygen concentration causes some yet
undiscovered vasoconstrictor substance to be
released from the lung tissue;
• this substance promotes constriction of the small
arteries and arterioles.
• It has been suggested that this vasoconstrictor might
be secreted by the alveolar epithelial cells when
they become hypoxic.
24. Importance of PulmonaryImportance of Pulmonary
vasoconstriction by hypoxiavasoconstriction by hypoxia
• To distribute blood flow where it is most effective.
• That is, if some alveoli are poorly ventilated so that
their oxygen concentration becomes low, the local
vessels constrict.
• This causes the blood to flow through other areas of
the lungs that are better ventilated,
• thus providing an automatic control system for
distributing blood flow to the pulmonary areas in
proportion to their alveolar oxygen pressures.
25. • 5) Hormonal Factors-
• VC - by Angiotensin II , E/NE, PGF2α, etc
• VD - by Ach, NO etc.
• Constrictors of pulmonary venules –
serotonin, histamine etc.
26. • 6) Phases of respiration-
• In inspiration there is pulmonary VD and increase in
pulmonary perfusion
• Inspiration causes fall of IPP which leads to traction
on bronchial walls which in turn are attached to
pulmonary vessels which also undergo traction thus
widening the vessels.
• In expiration there is VC and increase pulmonary
vascular resistance leading to decrease perfusion.
27. • 7) Effect of gravity-
• In erect posture more marked pressure
gradient in pulmonary arteries from top to
bottom of lungs because of effect of gravity.
• This results in a linear increase in pulmonary
blood flow from apex to base of lung
• In supine lying position all parts of lung get
same blood flow.
28. • Normally in standing position, the hydrostatic
pressure in lower extremity of the body is very
high and in upper parts above the level of
heart the pressure is low.
• This is due to gravitation effect.
• A similar condition is observed to some extent
in lungs also.
• The pulmonary vascular pressure varies in
different portions of the lungs
29. • The pulmonary arterial pressure in the uppermost
portion of the lung of a standing person is about 15 mm
Hg less than the pulmonary arterial pressure at the level
of the heart,
• and the pressure in the lowest portion of the lungs is
about 8 mm Hg greater.
• Such pressure differences have profound effects on
blood flow through the different areas of the lungs.
• In the standing position at rest, there is little flow in the
top of the lung but about five times as much flow in the
bottom.
• lung as being divided into three zones.
30.
31. ApexApex
• At the apical portion- Pulmonary capillary pressure is
same as atmospheric pressure in alveoli.
• So in normal conditions pulmonary arterial pressure
is just sufficient for blood flow in the capillaries.
• But if pulmonary arterial pressure is decreased or if
alveolar pressure is increased the capillaries collapse
• and thus no blood flow and hence apex is area of
zero blood flow
32. Mid portion of lungMid portion of lung
• Alveolar pressure is less than pulmonary
artery systolic pressure but more than its
diastolic pressure.
• Hence blood flows in the alveolar pulmonary
cap in systole and it is prevented during
diastole.
• So this part gets intermittent blood flow.
33. Lower portion of lungLower portion of lung
• Here the pulmonary arterial pressure
is high and more than alveolar
pressure in both during systole and
diastole.
• Thus there is a continuous blood
flow in this part of the lung.
34. Exercise effectExercise effect
• 8) Effect of exercise –
• Exercise causes rise of CO and blood flow through
the lungs increases fourfold to sevenfold. This extra
flow is accommodated in the lungs in three ways:
• (1) by increasing the number of open capillaries,
sometimes as much as threefold;
• (2) by distending all the capillaries and increasing
the rate of flow through each capillary more than
twofold;
35. • In the normal person, these changes decrease
pulmonary vascular resistance so much that the
pulmonary arterial pressure rises very little, even
during maximum exercise
• The ability of the lungs to accommodate greatly
increased blood flow during exercise without
increasing the pulmonary arterial pressure
conserves the energy of the right side of the
heart.
• This ability also prevents a significant rise in
pulmonary capillary pressure, thus also
preventing the development of pulmonary
edema.
36.
37. Ventilation – Perfusion RatioVentilation – Perfusion Ratio
• It is the ratio of alveolar ventilation and the
amount of blood that perfuse the alveoli.
• It is expressed as VA/Q.
• VA is alveolar ventilation, Q is blood flow.
• Normal value for whole blood is 0.8
• 4.2 L/min / 5 L /min = 0.84
38. Significance of the ratioSignificance of the ratio
• At ratio of 0.84 there is maximum
oxygenation of blood.
• This ratio determines the pulmonary
gas exchange and composition of
alveolar air
39. Variations in the ratioVariations in the ratio
• Physiological variation-
• Ratio increases, if ventilation increases without
change in blood flow.
• Ratio decreases , if blood flow increases without any
change in ventilation.
• Effect of posture – in upright position high ratio at
apex (3.3) due to less perfusion due to effect of
gravity and
• at the base ratio is decreased (0.6) as very high
perfusion due to gravity and
• in the middle ratio is almost (1)
40. • Pathological variation
• Uneven ventilation as seen in Bronchial
asthma, emphysema, pneumothorax,
pulmonary fibrosis
• Uneven pulmonary blood flow as in
Fallot’s Tetralogy, pulmonary embolism
etc.
41. Effects of change in ratioEffects of change in ratio
• At the apex- due to less perfusion there
develops Physiological dead space which
favors growth of TB bacilli
• also as perfusion is less - blood borne
immunity like Abs and lymphocytes is less
• At the base – Very high perfusion as
compared to ventilation so development of
physiological shunt blood which means
• blood leaving this part continues to be
deoxygenated.
42.
43. Pulmonary capillary dynamicsPulmonary capillary dynamics
• The capillary blood flows in the alveolar
walls as a “sheet of flow,” rather than in
individual capillaries.
• The alveolar walls are lined with so many
capillaries that, in most places, the
capillaries almost touch one another
side by side.
44. Pulmonary capillary pressurePulmonary capillary pressure
• No direct measurements of pulmonary capillary
pressure have ever been made.
• “isogravimetric” measurement of pulmonary
capillary pressure, using a technique has given a
value of 7 mm Hg.
• This is probably nearly correct, because the mean
left atrial pressure is about 2 mm Hg and the mean
pulmonary arterial pressure is only 15 mm Hg,
• so the mean pulmonary capillary pressure must lie
somewhere between these two values.
45. Length of time blood stays in theLength of time blood stays in the
pulmonary capillariespulmonary capillaries
• From histological study of the total cross-
sectional area of all the pulmonary
capillaries, it can be calculated that
• when the cardiac output is normal,
blood passes through the pulmonary
capillaries in about 0.8 second.
46. Upon increase of cardiac outputUpon increase of cardiac output
• When the cardiac output increases, this can
shorten to as little as 0.3 second. The
shortening would be much greater if it is not
for the fact that additional capillaries, which
normally are collapsed, open up to
accommodate the increased blood flow.
• Thus, in only a fraction of a second, blood
passing through the alveolar capillaries
becomes oxygenated and loses its excess
carbon dioxide
47. Dynamics of fluid exchangeDynamics of fluid exchange
• 1)Low Pulmonary capillary pressure-
• The pulmonary capillary pressure is low,
about 7 mm Hg, in comparison with a
considerably higher functional capillary
pressure in the peripheral tissues of
about 17 mm Hg.
48. More negative interstitial fluidMore negative interstitial fluid
pressurepressure
• 2. The interstitial fluid pressure in the lung is
slightly more negative than that in the
peripheral subcutaneous tissue.
• (This has been measured in two ways: by a
micropipette inserted into the pulmonary
interstitium, giving a value of about –5 mm
Hg, and by measuring the absorption pressure
of fluid from the alveoli, giving a value of
about –8 mm Hg.)
49. Leaky pulmonary capillaries – moreLeaky pulmonary capillaries – more
COP of interstitial fluid- 14 mm HgCOP of interstitial fluid- 14 mm Hg
• 3. The pulmonary capillaries are
relatively leaky to protein molecules, so
that the colloid osmotic pressure of the
pulmonary interstitial fluid is about 14
mm Hg,
• in comparison with less than half this
value in the peripheral tissues.
50. Thin alveolar wallsThin alveolar walls
• 4. The alveolar walls are extremely thin,
and the alveolar epithelium covering the
alveolar surfaces is so weak that it can
be ruptured by any positive pressure in
the interstitial spaces greater than
alveolar air pressure (greater than 0 mm
Hg),
• which allows dumping of fluid from the
interstitial spaces into the alveoli.
52. • Thus, the normal outward forces are
slightly greater than the inward forces,
providing a mean filtration pressure which
can be calculated as follows
53. Filtration from pulmonary cap intoFiltration from pulmonary cap into
interstitial space into lymphaticsinterstitial space into lymphatics
• This filtration pressure causes a slight
continual flow of fluid from the pulmonary
capillaries into the interstitial spaces,
• and except for a small amount that
evaporates in the alveoli, this fluid is pumped
back to the circulation through the
pulmonary lymphatic system.
54. Negative Interstitial pressure and itsNegative Interstitial pressure and its
role in keeping alveoli dryrole in keeping alveoli dry
• Whenever extra fluid appears in the alveoli, it will
simply be sucked mechanically into the lung
interstitium through the small openings between the
alveolar epithelial cells.
• Then the excess fluid is either carried away through
the pulmonary lymphatics or absorbed into the
pulmonary capillaries.
• Thus, under normal conditions, the alveoli are kept
“dry,” except for a small amount of fluid that seeps
from the epithelium onto the lining surfaces of the
alveoli to keep them moist.
55. Pulmonary oedemaPulmonary oedema
• Pulmonary edema occurs in the same way
that edema occurs elsewhere in the body.
• Any factor that causes the pulmonary
interstitial fluid pressure to rise from the
negative range into the positive range
• will cause rapid filling of the pulmonary
interstitial spaces and alveoli with large
amounts of free fluid.
56. Causes of pulmonary oedemaCauses of pulmonary oedema
• 1. Left-sided heart failure or mitral valve disease,
with consequent great increases in pulmonary
venous pressure and pulmonary capillary pressure
and flooding of the interstitial spaces and alveoli.
• 2. Damage to the pulmonary blood capillary
membranes caused by infections such as pneumonia
or by breathing noxious substances such as chlorine
gas or sulfur dioxide gas.
• Each of these causes rapid leakage of both plasma
proteins and fluid out of the capillaries and into
both the lung interstitial spaces and the alveoli.
57. Pleural EffusionPleural Effusion
- Pleural effusion means the collection of large amounts
of free fluid in the pleural space.
- “edema of the pleural cavity.”
- (1) blockage of lymphatic drainage from the pleural
cavity;
- (2) cardiac failure, which causes excessively high
peripheral and pulmonary capillary pressures, leading to
excessive transudation of fluid into the pleural cavity;
- (3) greatly reduced plasma colloid osmotic pressure,
thus allowing excessive transudation of fluid; and
- (4) infection or any other cause of inflammation of
the surfaces of the pleural cavity, which breaks down the
capillary membranes and allows rapid dumping of both