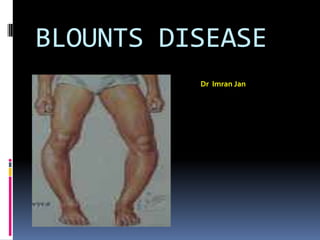
2. Definition
It is an disorder of the proximal
medial tibial growth plate
causes progressive varus
alignment of the knees (bowed
legs) in children or adolescents .
3. synonyms
Infantile tibia vara
Erlacher`s disease
Blount-barber disease
Subepipyseal osteochondropathy
Non rachitic bow legs
Ostetis deformans tibia
4.
5. BLOUNTS DISEASE
Erlacher first description of
tibia vara and internal tibial torsion
(1922)
Blount (1937) described tibia vara as
“an osteochondrosis similar to coxa
plana and Madelung's deformity but
located at the medial side of the
proximal tibial epiphysis.”
.
6. Prevalence
<1% of all bow legs
The infantile form is more common in girls.
The juvenile or adolescent form is more
common in boys.
The disorder is more common in African
American children than those of other races.
7. ETIOLOGY
Current concept is tibia vara is
An acquired disease of the
proximal tibial metaphysis of
unknown cause
Enchondral ossification seems
to be altered.
8. Suggested causative factors include
infection
trauma
osteonecrosis
latent form of rickets
although none of these has been proved
A combination of hereditary and
developmental factors is the most
likely cause
9. The relationship of early walking
and obesity to Blount disease
has been clearly documented.
Rarely seen in non ambulant
children
10. BLOUNTS DISEASE
COMPONENTS OF DEFORMITY
Varus
Internal torsion of tibia
Recurvatum
LLD
Femoaral varus late
MSC hypertrophy
11. PATHOLOGY
islands of densely packed chondrocytes with
hypertr0phy
areas of almost acellular cartilage
Intraphyseal ossification centers
abnormal groups of capillaries.
Extension of noncalcified cartilaginous bars
into the proximal epiphysis and distal
metaphyses
12. CLASSIFICATON
Infantile:
before 8 years of age
bilateral in 60%
Adolescent more than 8Yrs till
skeletal fusion
1 with a cause
2 obese , black
14. Radiology
medial half of the epiphysis as seen on
radiographs is short, thin, and wedged
the physis is irregular in contour and slopes
medially.
The proximal metaphysis forms a projection
medially
. According to Smith, however, medial
metaphyseal fragmentation is pathognomonic
for the development of a progressive tibia
vara.
19. Langenskiold classification
(1952)
I - irregular metaphyseal ossification combined with medial and distal
protrusion of the metaphysis
II, III, IV - evolves from a mild depression of the medial metaphysis to a
step-off of the medial metaphysis
V - increased slope of medial articular surface and a cleft separating the
medial and lateral epicondyle
VI - bony bridge across the physis
Depending on degree of metaphysial and epiphysial changes
on radiograph – 6 progressive stages with increasing age
20. Work up findings
No specific blood marker
Tests to R/o Infection and
Rickects
CT scan in 5yrs + to detect
physeal bar
22. Treatment
Treatment choices and
prognosis depend greatly on
the age of the patient and
radiographic stage at the time
of diagnosis
23. Rx - Orthotics
Recommended for patients < 3 years of age and <
stage II disease
Rainey et al recommended LOCKED KAFO that
produced a valgus force by three point pressure
23 HRS /DAY
Full weight bearing
Risk for failure included ligamentous
instability, patient weight above 90th percentile and
late initiation of bracing
25. Rx – Corrective Osteotomy…
Rab
proximal tibial oblique
metaphyseal osteotomy in which
single plane oblique cut allows simultaneous
correction of varus and internal rotation and
permits postoperative cast wedging if necessary
to obtain appropriate position.
28. Rx – Corrective Osteotomy…
Greene
Chevron open- closing wedge osteotomy in
which opening and closing wedges can be
made so that the limb length deformity
present in moderate to severe tibia vara will
not be increased. He prefers a crescent
shaped osteotomy using one half lateral
closing wedge and using the graft medially in
an opening wedge to maintain length.
30. Rx – Corrective Osteotomy…
In children older than 9 years with more severe
involvement, osteotomy alone, with bony bar
resection, or with epiphysiodesis of the lateral
tibial and fibular physes may be indicated
For older children in whom bracing and tibial
osteotomy have failed to prevent progressive
deformity, Ingram, Siffert and others have
suggested an intraepiphyseal osteotomy to
correct severe joint instability and a valgus
metaphysial osteotomy to correct the varus
angulation
31. Rx – Corrective Osteotomy…
Schoenecker et al – elevation of medial tibial
plateau with metaphysial wedge osteotomy
Gregosiewics – double elevating osteotomies;
intraepiphyseal and metaphyseal
Zayer – hemicondylar tibial osteotomy through
the epiphysis into the tibial intercondylar notch
Bell, Coogan – recommended Ilizarov’s
technique
Uniplanar external fixator for isolated frontal one
plane deformity
37. CONGENITAL METATARSUS
ADDUCTUS
Definition
Metatarsus adductus is a congenital
foot deformity consists of adduction
of the forefoot in relation to the
midfoot and hindfoot presenting as
in-toeing in children.
41. CONGENITAL METATARSUS ADDUCTUS
It can occur as an isolated
anomaly or in association with
clubfoot.
Among individuals with
metatarsus adductus, 1% to 5%
also have developmental
dysplasia of the hip or
acetabular dysplasia
42. Metatarsus adductus may be
seen as a residual deformity in
patients previously treated
surgically or nonsurgically for
congenital clubfoot.
This residual metatarsus adductus can be rigid, indicating fixed
positioning of the forefoot on the midfoot and hindfoot, or it can
be dynamic, caused by imbalance of the anterior tibial tendon
during gait.
43. CONGENITAL METATARSUS ADDUCTUS
BLECK classified as
mild
moderate
severe
In the mild form, the forefoot can be clinically
abducted to the midline of the foot and beyond
The moderate form has enough flexibility to allow
abduction of the forefoot to the midline only
In rigid metatarsus adductus, the forefoot cannot
be abducted at all.
55. CCV foot
Ccv presents
Marked dorsiflexion at ankle
Hind foot valgus
Dorsum of foot against anterior
surface of distal leg
Ankle ROM till neutral or lessat
birth with a dramatic