ACE Inhibitors
•
70 recomendaciones•29,756 vistas

Ref Book :Dr SK Srivastava,Dr H L Sharma and Dr KK sharma,Dr K D Tripathi, Dr Sparsh Gupta

Recomendados
Más contenido relacionado
La actualidad más candente
La actualidad más candente (20)
Similar a ACE Inhibitors
Similar a ACE Inhibitors (20)
Más de SMS MEDICAL COLLEGE
Más de SMS MEDICAL COLLEGE (20)
Último
Último (20)
ACE Inhibitors
- 3. RAAS –Hormonal System = Sym N System +Aldosterone system
- 4. RAAS
- 5. ACE Inhibitors • ACE = Angiotensin I Converting Enzyme • ACE inhibitors available – benazepril, captopril, enalapril, fosinopril, lisinopril, moexipril, perindopril, quinapril, ramipril and trandolapril. • ACE inhibitors were the 4th most prescribed drug . • Valsartan/sacubitril (codenamed LCZ696) is an investigational combination
- 6. Comparative pharmacokinetic properties of some commonly used ACE inhibitors Ï Drug *Bioavail PPC (h) ** Elim. T ½ (h) Route of Elim. Dose range & Frquency Captopril 75 1-2 2 Renal 25-100 mg, BD Enalapril 60 4-5 10 Renal 2.5-40mg, OD Lisinopril 30 5-8 12 Renal (unchanged) 5-40 mg, OD Prindopril 30 5-6 24 Renal 2-16 mg Ramipril 60 4-6 8-40 Renal 1.25-10 mg, OD Fosinopril 30 3-5 12 Hepatic/Ren al 10-80 mg OD Trandolapril 50 4-6 12-24 Renal 1-8 mg, OD Benazepril 40 4-6 8-12 Renal 5-80 mg, OD
- 7. Compartive features of Captopril, Enalapril and lisinopril Captopril Enalapril Lisinopril Active drug/Prodrug Active Prodrug Active Effect of food on absorption Reduced No Effect No effect Onset of action Faster Delayed Slow (slow absorption) Duration & frequency Short, BD Long, OD Long, OD Route of elimination Renal Renal Renal (unchanged) Dysguesia, skin rashes Common Less likely Less First dose hypotension Common Less likely Less likely
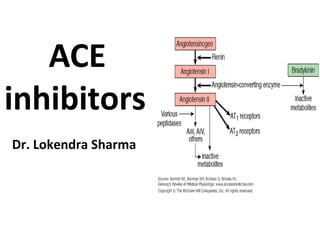
- 8. Other antihypertensive drugs that interfere with the Renin-Angiotensin System ACE KininogenAngiotensinogen Renin Kallikrein Angiotensin I (Inactive) Bradykinin B2 Receptor AT1 Receptor Angiotensin II Vasoconstriction Aldosterone release Na+ Retention Bradykinin(1-7) (Inactive) Blood Pressure Renin Inhibitor Aliskiren Vasodilation Na+ Excretion
- 10. Angiotensinogen Renin Angiotensin I (Inactive) Angiotensin II AT1 Receptor Blood Pressure Endopeptidases Angiotensin 1-7 AT1-7/Mas Receptor Angiotensin 1-5 (Inactive) ACE ACE Inhibitors Mechanism of Action of ACE Inhibitors II Vasodilation Na+ Excretion Anti-inflammatory Oxidative stress Vasoconstriction Aldosterone release Na+ Retention Pro-inflammatory Oxidative stress
- 11. Angiotensinogen Renin Angiotensin I (Inactive) Blood Pressure Kininogen Kallikrein Bradykinin Kinin B2 Receptor Vasodilation Na+ Excretion Bradykinin(1-7) (Inactive) ACE ACE Inhibitors Mechanism of Action of ACE Inhibitors Angiotensin II AT1 Receptor Vasoconstriction Aldosterone release Na+ Retention Pro-inflammatory Oxidative stress
- 12. ACE KininogenAngiotensinogen Renin Kallikrein Angiotensin I (Inactive) Bradykinin B2 Receptor AT1 Receptor Angiotensin II Vasoconstriction Aldosterone release Na+ Retention Bradykinin(1-7) (Inactive) Blood Pressure Angiotensin Receptor Antagonists (the “sartans”, e.g. Losartan) Vasodilation Na+ Excretion Other antihypertensive drugs that interfere with the Renin-Angiotensin System
- 13. CAPTOPRIL(ACE) :Mechanism of action: Inhibit angiotensin I to angiotensin II convertion. Decreased plasma angiotensin II. Increased plasma renin activity (PRA) resulting from loss of negative feedback on renin release. Decreased aldosterone secretion. small increases in serum potassium with sodium and fluid loss.
- 15. Why ACE inhibitors causes Cough ?
- 16. Therapeutic Uses • Anti-hypertensive • Prevent or reverse LVH • Protect against sudden death and second myocardial infarction after acute MI • Improve survival and hemodynamics in patients with congestive heart failure • Protect against progression of diabetic and non-diabetic nephropathy
- 17. Side Effects/Contraindications • Common – Dry Cough • 5 – 20% of patients • Not dose-related; occurs within 1 wk. – 6 mo. • Women > men • May Require cessation of therapy – Fetopathic Potential • Not teratogenic in 1st trimester • Developmental defects in 2nd or 3rd trimester • Rare – Angioneurotic Edema (or Angioedema) • ~0.1 - 0.5% of patients • Not dose-related; occurs within 1st week • Severe swelling of mouth, tongue, lips, airway • may be life-threatening
- 18. Side Effects/Contraindications • Rare – Hypotension • First dose effect in patients with elevated PRA, salt depletion, CHF – Hyperkalemia • In patients with renal insufficiency, diabetic nephropathy – Acute Renal Failure • Patients with renal stenosis, heart failure, volume depleted – Skin Rash • Extremely Rare (reversible) – Alteration/loss of taste – Neutropenia – Glycosuria – Hepatotoxicity
- 19. Drug Interactions – Antacids • May reduce bioavailability of ACE inhibitors – Capsaicin • May worsen ACE inhibitor-induced cough – NSAIDs • May reduce antihypertensive response to ACE inhibitors – K+ -sparing Diuretics or K+ supplements • May exacerbate ACE inhibitor-induced hyperkalemia
- 20. ENALAPRIL Mechanism of action: Prodrug which, when hydrolyzed by estarases to its active Enalaprilat. blocking the conversion of angiotensin I to angiotensin II. As angiotensin II is a vasoconstrictor and a negative-feedback mediator for renin activity, lower concentrations result in a decrease in blood pressure. act on kininase II,that degrades the vasodilator bradykinin.
- 21. Compartive Pharmacokinetic Properties of Angiotensin Receptor Blockers Drug PI t1/2 (h) PPC (h) Elimination Dose/frequenc y Losartan 2-3 1 Renal/Hepatic 50mg, OD * E3174 7-9 3-4 Renal/Hepatic ---- Candesartan cilexetil 9 3-4 Renal/Biliary 4-32 mg, OD/BD Eprosartan 5-9 1-2 Renal/Hepatic 400-800mg, OD/BD Irbesartan 3 1-3 Biliary 25-100 mg, OD/BD Olmesartan medoxomil 10-15 1.4-2.8 Renal/Biliary 20-40 MG, OD Telmisartan 24 0.5-1 Biliary 40-80mg, OD Valsartan 6-9 2-4 Hepatic 80-320 mg, OD
- 23. Write the name of ACE inhibitor which is eliminated by both kidney & liver ? Fosinopril
- 24. Which type of medications should not be taken with an ACE inhibitors? Potassium-sparing diuretics
- 25. What are the cardiorenal Effects of ACE Inhibitors ? Vasodilation (arterial & venous) Decrease blood volume Depress sympathetic activity Inhibit cardiac and vascular hypertrophy
- 26. Write Therapeutic Use of ACE Inhibitors ? Hypertension Heart failure Post-myocardial infarction
- 27. ACE inhibitor associated with taste distrubances due to its sulfhydryl moiety? Captopril
- 28. Cough and angioedema in a patient receving ACE inhibitors is occur due to ? Bradykinin
- 29. oral bioavailability is not reduce by food for which ACE inhibitors ? Enalapril Lisinopril Trandolapril Perindopril
- 30. Write the name of active ACE inhibitors? Captopril and Lisinopril
- 31. Management of excessive hypotensive reaction probably caused by continued ACE inhibitor treatment perioperatively? crystalloid fluid infusion sympathomimetic administration
- 32. What are the contraindications of Enalapril ? Single kidney or Bilateral renal artery stenosis Hyperkalemia
- 33. Which ACE inhibitor is available as a separate drug meant for use in hypertensive emergencies? Enalaprilat by IV route
- 34. Role of ACE inhibitors in scleroderma crisis? Prevent the manifestations of scleroderma crisis which are mediated by angiotensin II.
- 35. What is the most frequently adverse effect associated with ACE inhibitors and its treatment? Dry cough. It can be reduced by iron supplements and asprin.
- 36. What are the contraindications of ACE inhibitors? Pregnancy (teratogenic in second half of pregnancy) and when serum creatinine is more than 3.5 mg/dl.
- 37. Which ACE inhibitor causes postural hypotension? Captopril
- 38. Role of Angiotensin converting enzyme inhibitors in CHF? First choice drugs unless contra-indicated
- 39. Drugs that can be used for the treatment of hypertension in a diabetic patient? ACE inhibitors (e.g. captopril) and AT1 antagonists (e.g. losartan)
- 40. Antihypertensive drugs having neutral role in lipid metabolism? ARB and ACE inhibitors
- 41. Ramesh is CEO in a company and has a traveling job. He is a known diabetic controlled on oral hypoglycemic drugs. On his recent visit to the doctor, his blood pressure was found to be 164/102 mm Hg. Most suitable drug for this patient should be ? Enalapril
- 42. Indication of ACE inhibitor in diabetes mellitus are? Diabetic nephropathy and Nephropathy unrelated to diabetes
- 43. Write the names of ACE inhibitors whose absorption is reduced by food? Fosinopril Quinapril Ramipril
- 44. What is the effect of Enalapril on renin on prolonged use? Increase
- 45. ACE Inhibitors should not be given with? Spironolactone
- 46. Difference between ACE inhibitors and ARBs? ARBs do not increase bradykinin and thus have less chances of causing cough and angioedema as compared to ACE inhibitors
- 47. Indications of ACE inhibitors? ACEI are used for the treatment of: Hypertension, CHF, evolving MI, diabetic nephropathy, diabetic retinopathy, non-diabetic renal disease and in scleroderma crisis
- 48. Mechanism of action of ACE inhibitors? Decreases the activity of RAAS and also potentiate the vasodilatory action of bradykinin
- 49. Compounds included in ACE inhibitors? Captopril Enalapril Lisinopril Ramipril Perindopril Trandolapril Fosinopril & Moexipril
- 50. What are the differencs between captopril and other ACEIs? Important differences between is that captopril is lesspotent, has fast onset and short duration of action and less absorption in presence of food in GIT.
- 51. Mention the teratogenic effects of ACE inhibitors? Fetal growth retardation Hypoplasia of organs Fetal death
- 52. Angioedema
- 53. Agranulosytosis
- 54. Agranulocytosis
Notas del editor
- Renin act on angiotensinogen (plasma globulin) Main function of Angiotensin ll vasoconstruction sodium and water retention
- Valsartan/sacubitril (codenamed LCZ696) is an investigational combination drug consisting of two antihypertensives (blood pressure lowering drugs),
- Notes: Ï All are prodrug except captopril, lisinopril and enalaprilat, active metabolite of enalapril (not shown) * Biovailability of active form/drug ** Elimination t1/2 also included the active metabolite; OD = once a day, BD = twice a day. PPC = Peak Plasma concentration
- An additional mechanism by which ACE inhibitors can work involves the angiotensin metabolite, Angiotensin 1-7 (1 residue shorter than angiotensin II). This metabolite can be generated directly from angiotensin I by endopeptidases such as neutral endopeptidase, prolylendopeptidase and thimet oligopeptidase. Angiotensin 1-7, acting through its receptor (also called the Mas receptor), has effects opposite to those of angiotensin II and thereby is a negative regulator of the renin-angiotensin system. ACE inhibitors promote angiotensin 1-7 generation via 2 mechanisms: 1) increasing angiotensin 1 levels by inhibiting conversion to angiotensin II increases substrate concentration and thus conversion by endopeptidases. 2) by blocking ACE metabolism of angiotensin 1-7 into the inactive metabolite angiotensin 1-5.
- prevents the conversion of angiotensin I to angiotensin II by inhibition of ACE. Decreased plasma angiotensin II. Increased plasma renin activity (PRA) resulting from loss of negative feedback on renin release. Decreased aldosterone secretion. small increases in serum potassium with sodium and fluid loss.
- Enalapril, an angiotensin-converting enzyme (ACE) inhibitor, is a prodrug which, when hydrolyzed by estarases to its active Enalaprilat. Mechanism of action: Enalaprilat competes with angiotensin I for binding at the angiotensin-converting enzyme, blocking the conversion of angiotensin I to angiotensin II. As angiotensin II is a vasoconstrictor and a negative-feedback mediator for renin activity, lower concentrations result in a decrease in blood pressure. Enalaprilat may also act on kininase II,that degrades the vasodilator bradykinin. Pharmacokinetic data : Bioavailability - 60% (oral), Metabolism - hepatic (to enalaprilat), Half-life - 11 hours (enalaprilat), Excretion - renal. Clinical uses : Management of hypertension. In hypertensive patients with heart failure, postmyocardial infarction, high coronary disease risk etc.
- Active carboxylic acid metabolite of losartan Notes: 1 Candesartan and olemesartan are the prodrugs (inaxtive esters) and converted to active form during absorption from GIT. Food reduces absorption of valsartan. Irbesartan also generates active metabolite (t1/2 6-9h) and also has antiplatelet action by blocking TXA2 receptor. Irbesartan, Telmisartan and valsartan are safe in renal insufficiency as they are not eliminated through kidneys.