Organisational Outcomes of Person-Centred Hearing Care
•
1 recomendación•121 vistas

Research Aims: 1.According to senior management, how is ‘success’ defined and evaluated in hearing care organisations in Australia? a)What are the organisational values used to drive clinical practice and clinical change? b)What are the measures used to drive clinical practice and clinical change? c)To what extent it PCC reflected in these values and measures? 2.What short and long term effects does a PCC approach have on the measures?
Recomendados

Recomendados
Más contenido relacionado
La actualidad más candente
La actualidad más candente (20)
Destacado
Destacado (8)
Similar a Organisational Outcomes of Person-Centred Hearing Care
Similar a Organisational Outcomes of Person-Centred Hearing Care (20)
Más de HEARnet _
Más de HEARnet _ (20)
Último
Último (20)
Organisational Outcomes of Person-Centred Hearing Care
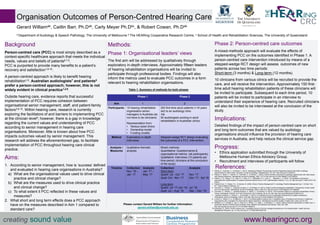
- 1. Organisation Outcomes of Person-Centred Hearing Care Gerard Williamab, Caitlin Barr, Ph.Dab, Carly Meyer Ph.Dbc, & Robert Cowan, Ph.Dab a Department of Audiology & Speech Pathology, The University of Melbourne b The HEARing Cooperative Research Centre, c School of Health and Rehabilitation Sciences, The University of Queensland Background Person-centred care (PCC) is most simply described as a context-specific healthcare approach that meets the individual needs, values and beliefs of patients6,7,9. PCC is purported to provide many benefits to a patient’s recovery and satisfaction1,6-10. A person-centred approach is likely to benefit hearing rehabilitation1,6. Australian audiologists7 and patients5 prefer a person-centred approach; however, this is not widely evident in clinical practice1,2,6. Outside hearing care, evidence reports that successful implementation of PCC requires cohesion between organisational senior management, staff, and patient-family factors3,8,10. Within hearing care, research is currently exploring the facilitators of and barriers to implementing PCC at the clinician level5; however, there is a gap in knowledge regarding the current values and understanding of PCC according to senior management in hearing care organisations. Moreover, little is known about how PCC impacts outcomes valued by senior management. This research will address the aforementioned gap, to facilitate implementation of PCC throughout hearing care clinical practice. Aims: 1. According to senior management, how is ‘success’ defined and evaluated in hearing care organisations in Australia? a) What are the organisational values used to drive clinical practice and clinical change? b) What are the measures used to drive clinical practice and clinical change? c) To what extent it PCC reflected in these values and measures? 2. What short and long term effects does a PCC approach have on the measures described in Aim 1 compared to standard care? Phase 2: Person-centred care outcomes A mixed-methods approach will evaluate the effects of implementing PCC on the outcomes identified in Phase 1. A person-centred care intervention introduced by means of a stepped-wedge RCT design will assess outcomes of new patients across two time periods: Short-term (3 months) & Long-term (12 months). 10 clinicians from various clinics will be recruited to provide the care, and will receive the intervention. Approximately 150 first- time adult hearing rehabilitation patients of these clinicians will be invited to participate. Subsequent to each time period, 10 patients will be invited to participate in an interview to understand their experience of hearing care. Recruited clinicians will also be invited to be interviewed at the conclusion of the study. Implications: Detailed findings of the impact of person-centred care on short and long term outcomes that are valued by audiology organisations should influence the provision of hearing care services in Australia, and help reduce the clinical service gap. Progress: • Ethics application submitted through the University of Melbourne Human Ethics Advisory Group. • Recruitment and interviews of participants will follow. creating sound value www.hearingcrc.org References:1. Ekberg, K., Grenness, C., & Hickson, L. (2014). Addressing Patients’ Psychosocial Concerns Regarding Hearing Aids Within Audiology Appointments for Older Adults. American Journal of Audiology, 23(September), 337–351. http://doi.org/10.1044/2014 2. Ekberg, K., Meyer, C., Scarinci, N., Grenness, C., & Hickson, L. (2015). Family member involvement in audiology appointments with older people with hearing impairment. International Journal of Audiology, 54(2), 70–76. http://doi.org/10.3109/14992027.2014.948218 3. Helfrich, C. D., Sylling, P. W., Gale, R. C., Mohr, D. C., Stockdale, S. E., Joos, S., … Meredith, L. S. (2015). The facilitators and barriers associated with implementation of a patient-centered medical home in VHA. Implementation Science, 11(1), 24. http://doi.org/10.1186/s13012-016- 0386-6 4. Hosford-Dunn, H., Roeser, R.J., & Valente, M. (2008). What is Practice Management? In Audiology Practice Management (pp.1-12).New York, NY: Thieme Medical Publishers, Inc. 5. Grenness, C., Hickson, L., Laplante-Lévesque, A., & Davidson, B. (2014). Patient-centred audiological rehabilitation: Perspectives of older adults who own hearing aids. International Journal of Audiology, 53(S1), S68–S75. http://doi.org/10.3109/14992027.2013.866280 6. Grenness, C., Hickson, L., Laplante-lévesque, A., Meyer, C., & Davidson, B. (2015). Communication Patterns in Audiologic Rehabilitation History- Taking: Audiologists, Patients, and Their Companions. Ear & Hearing, 36, pp.191-204. http://doi.org/0196/0202/2015/362-0191/0 7. Laplante-Lévesque, A., Hickson, L., & Grenness, C. (2014). An Australian survey of audiologists’ preferences for patient-centredness. International Journal of Audiology, 53(S1), S76–S82. http://doi.org/10.3109/14992027.2013.832418 8. Luxford, K., Safran, D. G., & Delbanco, T. (2011). Promoting patient-centered care: A qualitative study of facilitators and barriers in healthcare organizations with a reputation for improving the patient experience. International Journal for Quality in Health Care, 23(5), pp.510–515. 9. McMillan, S. S., Kendall, E., Sav, A., King, M. A., Whitty, J. A., Kelly, F., & Wheeler, A. J. (2013). Patient-Centered Approaches to Health Care: A Systematic Review of Randomized Controlled Trials. Medical Care Research and Review, 70(6), 567–596. http://doi.org/http://dx.doi.org/10.1177/1077558713496318 10. Rosengren, K. (2016). Person-centred care : A qualitative study on first line managers experiences on its implementation. Health Services Management Research, pp.1-8. http://doi.org/10.1177/0951484816637748 Please contact Gerard William for further information: gerard.william@unimelb.edu.au Methods: Phase 1: Organisational leaders’ views The first aim will be addressed by qualitatively through exploratory in-depth interviews. Approximately fifteen leaders of hearing rehabilitation organisations will be invited to participate through professional bodies. Findings will also inform the metrics used to evaluate PCC outcomes in a form relevant to hearing rehabilitation organisations. Phase 1 Phase 2 Aim 1 2 Participants: 15 hearing rehabilitation organisation senior managers in Australia (do not have to be clinicians) Representation from: • Various sized clinics • Ownership model • Funding models 200 first-time adult patients (>18 years old) to an audiology clinic Via 50 audiologists working in adult rehabilitation in Australian clinics Method Exploratory in-depth interviews Stepped-wedge RCT design evaluating the outcomes of a PCC intervention. Analysis / Measures Qualitative thematic analysis Mixed methods: Quantitative: Questionnaires & organisational metrics (all participants). Qualitative: Interviews (10 patients per time period; clinicians at the conclusion of the study) Timeline Collection: Nov ‘16 – Jan ’17 Analysis: Jan ‘17 – May ‘17 Collection: Short-term Quant: Jul - Oct ’17 Qual: Oct - Nov ‘17 Long-term Quant: Jul ‘17-Jun ’18 Qual: Jul – Aug ‘18 Analysis: Nov ‘17 Dec ’17- Apr’18 Jul ’18 Sep – Dec ‘18 Table 1: Summary of methods for both phases