
Recomendados
Más contenido relacionado
La actualidad más candente
La actualidad más candente (20)
Destacado
Destacado (20)
Similar a 14 CAP, COMMUNITY ASQUIRED PNEUMONIA
Similar a 14 CAP, COMMUNITY ASQUIRED PNEUMONIA (20)
Más de kdiwavvou
Más de kdiwavvou (20)
Último
Último (20)
14 CAP, COMMUNITY ASQUIRED PNEUMONIA
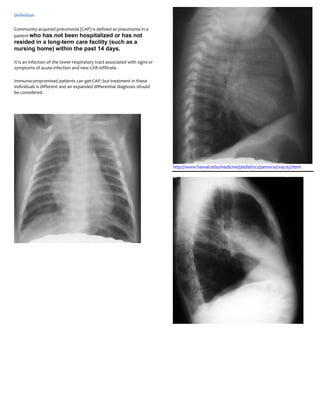
- 1. Definition Community-acquired pneumonia (CAP) is defined as pneumonia in a patient who has not been hospitalized or has not resided in a long-term care facility (such as a nursing home) within the past 14 days. It is an infection of the lower respiratory tract associated with signs or symptoms of acute infection and new CXR infiltrate. Immunocompromised patients can get CAP, but treatment in these individuals is different and an expanded differential diagnosis should be considered. http://www.hawaii.edu/medicine/pediatrics/pemxray/v4c03.html
- 2. These are PA and lateral films of RML pneumonia (arrows). Note the indistinct borders, air bronchograms, and silhouetting of the right heart border.
- 3. Diagnosis for Case of the Week - April 2, 2004 66 year old man s/p renal transplant with Shortness of Breathand Weight Loss PA and Lateral films of RUL pneumonia http://www.radiology.vcu.edu/programs/residents/quiz/Pulm_COTW/2 004%2004%2002%20cotw.htm
- 4. Community-acquired pneumonia treatment Key Highlights Acute Common symptoms include : all patients o cough, o fever and chills, o fatigue, supportive care o dyspnea, o rigors and o pleuritic pain outpatients Important historical factors to narrow the differential diagnosis are : previously healthy and drug-resistance unlikely macrolide or tetracycline therapy o recent respiratory infection, comorbidities or risk factors for drug-resistant S pneumoniae o exposure to respiratory illnesses, o immunocompromise, infection o smoking, fluoroquinolone or combination therapy o alcohol, o travel and o occupational risks inpatients o > 65 years old non-ICU cases OFTEN DIAGNOSIS AND TREATMENT CAN BE BASED SOLELY ON HISTORY AND PHYSICAL EXAM. fluoroquinolone or combination therapy vancomycin or linezolid The most specific and sensitive test is CXR (PA and lateral). ICU cases (nonpseudomonal) combination therapy Initial treatment is empirical with antibiotics. vancomycin or linezolid ICU cases (pseudomonal) Other Factors combination therapy COMPLICATIONS o chills then fever o chest pain o abdominal pain ARDS o lung percussion dullness o bronchial breath sounds Pneumonia can be complicated by ARDS, which is a condition of o tactile vocal fremitus noncardiogenic pulmonary edema and severe lung inflammation. 1st Tests To Order This complication is associated with a 30% to 50% mortality and is treated with low tidal volume plateau pressure limited mechanical o CXR ventilation. o CBC o basic metabolic profile o oximetry or ABG EMPYEMA o blood culture o sputum culture Patients with pneumonia might have metastatic infections such as o sputum Gram stain empyema. [21] Other Tests to Consider Treated with antibiotics and operative drainage. o rapid urinary antigen tests ARTHRITIS o thoracentesis o serology o PCR Patients with pneumonia might have metastatic infections such as o M pneumoniae cold agglutinins septic arthritis. o rapid viral diagnostic tests o CT chest o Bronchoscopy MENINGITIS Patients with pneumonia might have metastatic infections such as meningitis. [21] Treated with antibiotics that are able to cross the blood-brain barrier.
- 5. INFECTIVE ENDOCARDITIS Patient Instructions Patients with pneumonia might have metastatic infections such as endocarditis. [22] The importance of adherence to medication should be emphasized, even if the patient is feeling better. Patients should be instructed to Treated with antibiotics but may require higher doses and longer call the office if their symptoms do not improve within 72 hours. durations than for pneumonia alone. Patient should be instructed to increase water intake to at least eight PERICARDITIS 8 to 12-oz glasses per day, unless otherwise contraindicated. If a patient is a smoker, the importance of smoking cessation during this illness should be stressed. Patient should be explained how smoking Patients with pneumonia might have metastatic infections such as impairs natural mechanisms to eliminate pathogens and debris. pericarditis. [21] To control systemic symptoms of pneumonia, aspirin or Treated with antibiotics but may also require drainage. acetaminophen is recommended (aspirin should not be used in pediatric patients). Patient should be advised to avoid cough suppressants. Patients with pneumonia might have metastatic infections such as Patients should be advised that fatigue is common during the acute peritonitis. [21] phase and that more rest than usual may be necessary. The patient can increase activity as tolerated after the acute phase. Treated with antibiotics. Prognosis Primary Prevention Although prognosis is generally good for patients treated with the appropriate antibiotics, roughly only 80% of patients CDC guidelines recommend pneumococcal polysaccharide vaccine treated with antibiotics have a resolution of clinical signs and should be administered to: [12] symptoms. A meta-analysis of 127 study cohorts revealed a mortality of nearly 14%. The range is from about 5% for Persons aged 65 years or greater hospitalized and ambulatory patients to over 30% for patients Immunocompetent persons aged 2 years or greater who are in intensive care. Factors associated with increased risk of at increased risk for illness and death associated with mortality are: male sex, pleuritic chest pain, hypothermia, pneumococcal disease because of chronic illness systolic hypotension, tachypnea, diabetes mellitus, neoplastic Persons aged 2 years or greater with functional or anatomic disease, neurologic disease, bacteremia, leukopenia and asplenia multilobar radiographic pulmonary infiltrate. Persons aged 2 years or greater living in environments in which the risk for disease is high Monitoring Immunocompromised persons aged 2 years or greater who are at high risk for infection. Monitoring parameters for CAP management should include Protection lasts for over 6 years in most people, although the aspects from both antimicrobial therapy and the disease state. protective value may be lost at a faster rate in elderly people than in Patients need to be educated on potential adverse reactions to younger adults. Anyone at risk of serious pneumonia should be chosen antibiotics and appropriate actions to be taken if these revaccinated 6 years after the first dose. occur. For example, patients should be counseled on the signs and symptoms of severe allergic reactions and should be Secondary Prevention provided with emergency contact information in case of drug side effects. Patients should also be closely monitored either in Pneumococcal vaccine helps to prevent CAP person or by telephone for signs and symptoms of disease resolution or for the worsening of disease. Pneumonia: there is poor-quality evidence that vaccination with pneumococcal vaccine may be no more effective than no vaccination Important parameters include vital signs, symptoms, and CBC at reducing the rates of acquiring definitive pneumococcal pneumonia and oxygen saturation. Although there is a lag time between in immunocompetent adults. improving clinical response and clearing of the CXR, a repeated CXR 4 to 6 weeks after treatment may be used to ensure the condition has not got worse.
- 6. Many viruses associated with CAP follow a seasonal pattern, including Evidence Level C influenza virus, respiratory syncytial virus (RSV) and parainfluenza virus. Other viruses that can cause CAP in adults include adenovirus Poor quality observational (cohort) studies or methodologically and hantavirus. For infants and young children, RSV is the most flawed randomized controlled trials (RCTs) of < 200 participants common cause of lower respiratory tract infections, with an estimated 25% of children hospitalized with pneumonia having RSV as the causative etiology. Pathophysiology Emerging Therapies Most of the infectious agents that cause CAP are aspirated into the Telithromycin lung. CAP that results from aspiration of oropharyngeal contents is the This new ketolide antibiotic is particularly active against resistant S only form of CAP with multiple pathogens. Among older patients, pneumoniae strains. Telithromycin is indicated for mild-to-moderate microaspiration of oropharyngeal secretions is common and is more CAP. However, the most recent ATS/IDSA guidelines comment that prevalent among patients with comorbidities and those taking additional safety data is required before making specific medications that cause sedation. recommendations for its use. An infection usually occurs when one component of the defense mechanism is not functioning properly. This results in microbial colonization of the upper respiratory tract. Microbes can enter and invade the lower respiratory tract by many methods and 6 Diagnostic Criteria mechanisms have been identified in the pathogenesis of pneumonia in immunocompetent adults: Criteria for severe community-acquired pneumonia Inhalation of infectious particles Minor criteria: Aspiration of oropharyngeal or gastric contents Hematogenous deposition of bacteria in the lung Respiratory rate 30 breaths/minute or greater Invasion from infection in contiguous structures PaO2/FiO2 ratio 250 or less Direct inoculation Multilobar infiltrates Reactivation. Confusion/disorientation Uremia (BUN ≥20 mg/dL) Certain pre-existing conditions such as cystic fibrosis, COPD, Leukopenia (WBC <4000 cells/mm^3) corticosteroid use, immunodeficiency, stroke, drug and alcohol use, Thrombocytopenia (platelet count <100,000 cells/mm^3) and pulmonary edema can hinder the ability of the host defense Hypothermia (core temperature <96.8ºF [36ºC]) system to expel the possible pathogens that can predispose an individual to acquiring CAP. Hypotension, requiring aggressive fluid resuscitation Bacterial pathogenesis depends on the virulence and number of Major criteria: organisms aspirated. For encapsulated organisms, such as S pneumoniae, the presence of different capsular polysaccharides, Invasive mechanical ventilation which prevent the host serum bactericidal activity (antibodies and Septic shock with need for vasopressors complement), and opsonic activity of polymorphonuclear leukocytes and macrophages may contribute to the pathogenesis and poor ICU admission is recommended for patients with major criteria or 3 of outcomes. the minor criteria. Once CAP is established, host humoral and cellular responses and early appropriate antimicrobial therapy are critical for containing the infection, preventing complications and improving outcome. Unfortunately, the rapid emergence of antibiotic resistance and Etiology immune deficiency has complicated treatment decisions. Streptococcus pneumoniae (also known as pneumococcus) is the most common cause of CAP. CAP can also be caused by Haemophilus influenzae, Staphylococcus aureus, Moraxella catarrhalis, Klebsiella pneumoniae and other gram- negative bacilli. Atypical microorganisms and respiratory viruses can also cause CAP. A 1996 prospective study identified the prevalence of various pathogens in 346 consecutive patients with CAP. Mycoplasma pneumoniae, Chlamydia pneumoniae and Legionella species accounted for 29%, 18% and 16% of cases, respectively.