Model Call Girls In Chennai WhatsApp Booking 7427069034 call girl service 24 ...
Cardiac rhythm disturbance
1. MAGDI AWAD SASI CARDIAC RHYTHM DISTURBANCE 2013 1
CARDIAC RHYTHM DISTURBANCE
2013
MAGDI AWAD SASI
2. MAGDI AWAD SASI CARDIAC RHYTHM DISTURBANCE 2013 2
Normal Sinus Rhythm
Implies normal sequence of conduction, originating in the sinus node and
proceeding to the ventricles via the AV node and His-Purkinje system.
EKG Characteristics: Regular narrow-complex rhythm
Rate 60-100 bpm
Each QRS complex is proceeded by a P wave
P wave is upright in lead II & downgoing in lead Avr
P wave should be present, lead 2,v1, positive deflection, single one p followed
by one QRS , fixed shape within normal 2.5 width and 2.5 height (2x2), fixed
P-R within normal max 0.2 sec.
3. MAGDI AWAD SASI CARDIAC RHYTHM DISTURBANCE 2013 3
Rhythm Of The Heart
The Heart is Like an Orchestra.
It has a conducting system
that is directed by a
conductor.
This conductor is the
“Natural Pacemaker” of the
Heart.
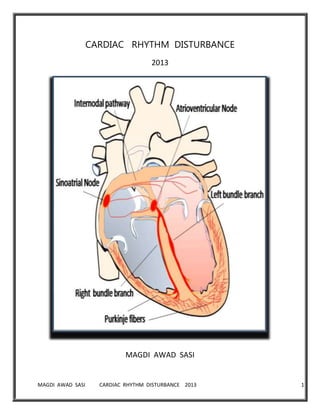
Conducting System:
- SA node (Primary
Pacemaker)
- AV node
- Bundle of His
- Purkinje Fibers
• Sino-Atrial node (SA Node)
-Origination and dissemination of electrical signals to BOTH atria
-Causes BOTH atria to contract
• Atrioventricular Node (AV Node)
-Transmits signal to ventricles by going through interventricular septum
-Causes intentional delay, to allow atria to complete pumping
• His Purkinje System
-Electrical signal flows through the His-Purkinje system and causes the
ventricles to contract SIMULTANEOUSLY
4. MAGDI AWAD SASI CARDIAC RHYTHM DISTURBANCE 2013 4
Normal ECG
Normal EKG:
1. Regular Rate –-----heart rate of 60-100 bpm
2. Regular Rhythm – P – QRS – T – P – QRS – T – P – QRS – T - etc
3. The height of the wave – related to the mass of the muscle
generating the wave
- The ventricles have more mass than the atria:
-
large ventricles (ventricular hypertrophy) more muscle creating a
stronger signal when the ventricles contract:
5. MAGDI AWAD SASI CARDIAC RHYTHM DISTURBANCE 2013 5
ATRIAL FIBRILLATION
AF results from random chaotic depolarization of the atria leading to an
irregularly, irregular tachycardia with irregular ventricular response.
Atrial rate usually 400-700 beat/minutes but ventricular rate is limited by
the refractory period at the AV node, so ventricular rate ranges from 140-
170 beat/minutes
In about one-third of patients with this arrhythmia, the patient is not
aware of so-called ‘asymptomatic AF’.
The prevalence of AF increases with age, from <0.5% at 40–50 years, to 5–
15% at 80 years
Pathophysiology
�No organized atrial electrical activity leads to loss of atrial contraction.
�Leads to loss of atrial kick with resultant decrease in ventricular filling
�This loss of contraction can lead to stagnation of blood in atrium and
can promote thrombus formation
�This thrombus can then be dislodged into the systemic circulation when
AF converts to sinus rhythm leading to thromboembolic complications
7. MAGDI AWAD SASI CARDIAC RHYTHM DISTURBANCE 2013 7
Inducing ectopic firing. A - Enhanced automaticity. B- EADs. C- DADs.
EAD indicates early after depolarizations; DAD, delayed after depolarization;
RyR, ryanodine receptor; and AP, action potential
Epidemiology
� most common arrhythmia encountered in clinical practice
Affects more than 2.3 million Americans
�Approximately 15-25% of all strokes in US can be attributed to AF
�Atrial fibrillation (AF) is the most common sustained cardiac arrhythmia,
occurring in 1–2% of the general population. Over 6 million Europeans suffer
from this arrhythmia, and its prevalence is estimated to at least double in the
next 50 years as the population ages
�The lifetime risk of developing AF is ∼25% in those who have reached the age
of 40year.
�AF account for one-third of all admissions for cardiac arrhythmias.
�Left ventricular (LV) function is often impaired by the irregular, fast
ventricular rate and by loss of atrial contractile function and increased end-
diastolic LV filling pressure. Both rate control and maintenance of sinus rhythm
can improve LV function in AF patients.
Classification
��Paroxysmal AF
Episodes that lasts less than 7 days
Terminate spontaneously
��Persistent AF
Episodes lasting more than 7 days
Require either pharmacologic or electrical intervention to terminate
��Permanent AF
Continuous AF that has failed cardioversion
��Lone AF
In individuals without structural or cardiac disease
Low risk for thromboembolism
9. MAGDI AWAD SASI CARDIAC RHYTHM DISTURBANCE 2013 9
CLINICAL FEATURES:
Asymptomatic, discover that they have atrial fibrillation at a doctor’s
appointment. Even without symptoms, atrial fibrillation is a serious medical
condition.
Others present with acute left ventricular failure symptoms if the atrial
contraction is mandatory for cardiac cycle in conditions with high end
intraventricular diastolic pressure i.e. aortic stenosis, HOCM, hypertension or
mitral stenosis.
Others present with dyspnea, palpitation, syncopy, chest pain or according to
underlying cause symptomatic presentation.
Chest discomfort or pain
Fainting or light-headedness
Fatigue, shortness of breath, or weakness
Atrial Fibrillation: Screening Procedures
All patients
– History
– Physical examination
– ECG
– Echocardiogram
– CBC, Thyroid function
Many/most patients
– Exercise stress test
– Holter monitor
Selected patients
– Chest x-ray
– Invasive procedures
10. MAGDI AWAD SASI CARDIAC RHYTHM DISTURBANCE 2013 10
Risk Factors
To help prevent atrial fibrillation, some risk factors may be controlled or modified.
Controllable Risk Factors
High cholesterol
High blood pressure
Heart disease
Smoking
Excess weight
Caffeine
Alcohol abuse
Lack of exercise
Some medications
Sleep apnea
Non-controllable Risk Factors
Family history
Advancing age
Heart disorders from birth
Atrial Fibrillation: Clinical Problems
Embolism and stroke (presumably due to LA clot)
Acute hospitalization with onset of symptoms
Anticoagulation, especially in older patients (> 75 yr.)
Congestive heart failure
o Loss of AV synchrony
o Loss of atrial “kick”
o Rate-related cardiomyopathy due to rapid ventricular response
Rate-related atrial myopathy and dilatation
Chronic symptoms and reduced sense of well-being
ECG
��Results from random chaotic depolarization of the atria
��No organized electrical activity
��No real P waves
��Irregular ventricular rhythm
��Ventricular rate may be fast or slow
11. MAGDI AWAD SASI CARDIAC RHYTHM DISTURBANCE 2013 11
The Major Goals in treating Atrial Fibrillation are:
Relieve AF symptoms and improve patient’s quality of life
Prevent blood clots to decrease the risk of stroke
Control the heart rate to allow the ventricles enough time to fill with
blood
Restore the heart rhythm to allow the atria and ventricles to work
together more efficiently
TREATMENT:
stable
Rate control
Anticoagulation
Conversion to and maintenance of sinus rhythm.
IF A PATIENT PRESENTS WITH A.F.,ANSWER 4 QS:
1. Is he/she haemodynamically stable?
2. Weather to control the rate or rhythm ?
3. What is the underlying cause ?
4. Is there an indication for anticoagulation ?
Urgent cardioversion W/ defibrillator: if hemodynamic instability, hypotension,
angina, heart failure , confusion due to low cardiac output ,no urine.
If cardioverting, ensure R-wave synchronization with electrical cardioversion to
prevent “R-on-T” shock which can induce Ventricular fibrillation.
12. MAGDI AWAD SASI CARDIAC RHYTHM DISTURBANCE 2013 12
There is also a role in the management of recent or new onset AF for elective
cardioversion when the patient is hemodynamically stable and one wishes to
try to bring them out of the arrhythmia if AF IS ACUTE AND LESS THAN 72 HRS,
OR TO BE ON WARFARIN FOR 4 WEEKS TO RAISE INR 2 TIMES NORMAL AND TO
DO CARDIOVERSION.
RHYTHM COTROL-
Synchronized DC cardioversion and pharmacologic cardioversion
> 48 hours, or <48 hrs with mitral stenosis or history of emboli – you must
anticoagulate
3-4 weeks of INR at 2-3
Unless – TEE has excluded thrombi
If unstable –DC cardioversion
If stable and correction of underlying problem does not help – either
choice
A. DC cardioversion – 75-93% successful
Depends on atrial size and duration of AF
B. Drugs – 30-60% successful
<7 days – dofetilide, flecainide, ibutilide, propafenone
>7 days – dofetilide
AGENT:
III: Amiodarone, Ibutilide, Dofetilide, Sotalol
IC: Flecainide, Propafenone
IA: Procainamide
RHYTHM CONTROL
ADVANTAGES
Avoids electrical and anatomical remodeling
Improves hemodynamics
Enhanced exercise capacity
Symptom relief
Improves Quality Of Life
Restores atrial transport
Reduces thromboembolic events?
13. MAGDI AWAD SASI CARDIAC RHYTHM DISTURBANCE 2013 13
DISADVANTAGES
Ventricular proarrhythmia
Increased mortality?
Drug-induced bradyarrhythmias
Adverse effects
Recurrences are likely
AF Antiarrhythmic Therapy
• Treatment goals
– ↓ frequency of recurrences
– ↓ duration of recurrences
– ↓ severity of recurrences
– Not to abolish every episode
• Safety is primary concern
• Minimize risk of proarrhythmia
After cardioversion;
Only 20-30 percent of patients stay in sinus for >1 year.
When to Consider Antiarrythmics ?
Don’t in patients with AF less than 1 year, no atrial enlargement,
reversible cause
Consider it in patients with high risk of recurrence
Risks generally outweigh benefits.
Amiodirone – good, but high toxicity profile, used in patients with
bad heart disease (significant systolic dysfunction, hypertension
with LVH)
Toxicity – pulmonary, photosensitivity, thyroid dysfxn,
corneal deposits, ECG changes, Liver dysfunction.
RATE CONTROL
o Essential in all patients.
o Persistent tachycardic rates can induce cardiomyopathy and heart failure.
o Occasional follow-up holter monitor to ascertain rate control.
o Achieved by slowing AV conduction (beta blockers, CCB, dig, amiodarone)
o Digoxin only in hypotension and Heart Failure
o Amiodirone – rarely but effective
14. MAGDI AWAD SASI CARDIAC RHYTHM DISTURBANCE 2013 14
Agents:
Beta Blocker: Metoprolol and Propranolol (ICU=esmolol )
Non-dihydropyridine CA blockers: verapamil & Diltiazem (ICU=diltiazem )
Digoxin Goal: Rest 60-80 bpm and Activity 80-110
IV Amiodarone (in the ICU setting)
Electrical ablation
RATE CONTROL; Which Agent to choose?
Estimated risk of stroke is determined with a CHADS2 score and therapy
determined with this scale of 1-6. (CHF, HTN, Age, DM, Secondary
prevention)
0 get ASA because of 0.5%/year w/o coumadin
1-2 intermediate risk
> or = 3 warfarin
P.S. – ASA usually added to warfarin
Anticoagulation during reversion to NSR
AF >48 hrs or unknown
Anticoagulate for >3 weeks, INR 2-3
15. MAGDI AWAD SASI CARDIAC RHYTHM DISTURBANCE 2013 15
Or, TEE to evaluate for clots in LA Appendage – if no clots – convert.
After, anticoagulate for 4 weeks with warfarin – “stunned atrium”
Consider chronic anticoagulation for those with high risk for reversion
16. MAGDI AWAD SASI CARDIAC RHYTHM DISTURBANCE 2013 16
Multifocal Atrial Tachycardia (MAT):
• Multiple ectopic focuses fire in the atria, all of which are conducted
normally to the ventricles
• QRS complexes are almost identical to the sinus beats
• Rate is usually between 100 and 200 beats per minute
• The rhythm is always IRREGULAR
• P-waves of different morphologies (shapes) may be seen if the rhythm is
slow
• If the rate < 100 bpm, the rhythm may be referred to as
“wandering pacemaker”
• Commonly seen in pulmonary disease, acute cardiorespiratory problems,
and CHF.
• Treatments:
1. Ca++
channel blockers
2. B blockers
3. potassium
4.magnesium,
• supportive therapy for underlying causes (antiarrhythmic drugs are
often ineffective)
17. MAGDI AWAD SASI CARDIAC RHYTHM DISTURBANCE 2013 17
Atrial Flutter:
• A single ectopic macroreentrant focuses fire in the atria causing the
“fluttering” baseline Classic inverted ,“sawtooth” ,flutter waves.
• AV node cannot transmit all impulses (atrial rate: 250 –350 per minute)
• ventricular rhythm may be regular or irregular and range from 150
–170 beats / minute
• A-fibrillation and A-flutter rhythm may alternate – these rhythms may
also alternate with SVT’s
• May be seen in CAD (especially following surgery), VHD, history of
hypertension, LVH, CHF
• Treatment:
• DC cardioversion if patient is unstable
• Drugs: (goal: rate control) Ca++
channelblockers to delay AV
conduction
• Amiodarone to delay AV conduction + prolong myocardial AP
(refractoriness of myocardium)
• The danger of thromboembolic events is also high in A-flutter.
18. MAGDI AWAD SASI CARDIAC RHYTHM DISTURBANCE 2013 18
Paroxysmal (of sudden onset) Supraventricular Tachycardia (PSVT):
• A single reentrant ectopic focuses fires in and around the AV node, all of
which are conducted normally to the ventricles (usually initiated by a
PAC)
• QRS complexes are almost identical to the sinus beats
• Rate is usually between 150 and 250 beats per minute
• The rhythm is always REGULAR
• Possible symptoms:
palpitations, angina, anxiety, polyuruia, syncope .
• Prolonged runs of PSVT may result in atrial fibrillation or atrial flutter
• May be terminated by carotid massage
• carotid pressure - baroreceptor firing rate –to increase vagal tone
by valsalva maneuver ,gag reflex, eye ball massage.
Treatment:
Ablation of focus, Adenosine (delay AV conduction), Ca++
Channel blockers
AV nodal reentrant tachycardia (AVNRT)
AV reentrant tachycardia (AVRT)
– Orthodromic
– Antidromic
19. MAGDI AWAD SASI CARDIAC RHYTHM DISTURBANCE 2013 19
PVC
A premature ventricular contraction (PVC), also known as a premature
ventricular complex, ventricular premature contraction (or complex or
complexes) (VPC), ventricular premature beat (VPB), or extrasystole, is a
relatively common event where the heartbeat is initiated by the heart ventricles
rather than by the sinoatrial node, the normal heartbeat initiator. The electrical
events of the heart detected by the electrocardiogram allow a PVC to be easily
distinguished from a normal heart beat.
PVC- bizarre , wide , not preceded by P wave, QRS reverse T wave
Causes
Ischemia
Certain medicines such as digoxin, which
increases heart contraction
Myocarditis
Cardiomyopathy, hypertrophic or dilated
Myocardial contusion
Hypoxia
Hypercapnia (CO2 poisoning)
Sarcoidosis[citation needed
Mitral valve prolapse
Smoking
Alcohol
Drugs such as cocaine
Caffeine
Theobromine[citation needed
Tricyclic antidepressants
Magnesium and potassium deficiency
Calcium excess
Thyroid problems
Chemical (electrolyte) problems in the blood
Heart attack
Adrenaline excess
Lack of sleep/exhaustion
Stress
20. MAGDI AWAD SASI CARDIAC RHYTHM DISTURBANCE 2013 20
PVCs may be unifocal , multifocal or multiformed. Multifocal PVCs have
different sites of origin, which means their coupling intervals (measured from
the previous QRS complexes) are usually different. Multiformed PVCs are
common in digitalis intoxication.
PVCs may occur as isolated single events or as couplets, triplets, and salvos (4-6
PVCs in a row), also called brief ventricular tachycardia’s.
21. MAGDI AWAD SASI CARDIAC RHYTHM DISTURBANCE 2013 21
PVCs may occur early in the cycle (R-on-T phenomenon), after the T wave , or
late in the cycle - often fusing with the next QRS (fusion beat). R-on-T PVCs may
be especially dangerous in an acute ischemic situation, because the ventricles
may be more vulnerable to ventricular tachycardia or fibrillation.
"Late" (end-diastolic) PVCs are illustrated with varying degrees of fusion. For
fusion to occur the sinus P wave must have made it to the ventricles to start the
activation sequence, but before ventricular activation is completed the "late"
PVC occurs. The resultant QRS looks a bit like the normal QRS, and a bit like the
PVC; i.e., a fusion QRS.
What is the risk of VPCS?
It depends on:
a. Frequency of VPCS
b. Form of VPCS_ uniform, multiform, salvos
VPCS IN ACUTE SYNDROMES:
1. Myocarditis/percarditis
2. Myocardial reperfusion-PRINZEMATALS ANGINA
THROMBOLYSIS IN MI, BALLON DEFLATION IN PTCA
c. Transient ischemic events
22. MAGDI AWAD SASI CARDIAC RHYTHM DISTURBANCE 2013 22
Ventricular tachycardia
(V-Tach or VT) is a tachycardia, or fast heart rhythm, that originates in one of
the ventricles of the heart. This is a potentially life-threatening arrhythmia
because it may lead to ventricular fibrillation, a systoles, and sudden death.
VT is defined as three or more consecutive ventricular ectopic impulses at a
rate 120/minutes or greater.
By ECG, rapid broad often bizarre QRS complexes with T waves usually opposite
in direction to the main QRS deflection and with rate /min or more.
VT can be defined by duration or ECG pattern.
Ventricular tachycardia can be classified based on its morphology:
A. Monomorphic ventricular tachycardia means that the appearance of all the
beats match each other in each lead of a surface electrocardiogram (ECG).
23. MAGDI AWAD SASI CARDIAC RHYTHM DISTURBANCE 2013 23
B. Polymorphic ventricular tachycardia, on the other hand, has beat-to-beat
variations in morphology. This most commonly appears as a cyclical progressive
change in cardiac axis, previously referred to by its French name torsades de
pointes ("twisting of the points"). However, currently the term torsades de
pointes is reserved for polymorphic VT occurring in the context of a prolonged
resting QT interval.
24. MAGDI AWAD SASI CARDIAC RHYTHM DISTURBANCE 2013 24
Another way to classify ventricular tachycardias is the duration of the episodes:
1. Non-sustained V. T__ the fast rhythm self-terminates within 30 seconds.
2. Sustained V.T. the rhythm lasts more than 30 seconds, (even if it terminates
on its own after 30 seconds).
VT CAN BE:
d. Bigiminy, trigiminy.
e. Couplet , triplet.
f. Salvos-uniform morphology VT-3 to 5 v.ectopics.
Descriptors to consider when considering ventricular tachycardia:
Sustained (lasting >30 sec) vs. nonsustained
Monomorphic (uniform morphology) vs. polymorphic vs. Torsade-d.p.
25. MAGDI AWAD SASI CARDIAC RHYTHM DISTURBANCE 2013 25
Torsade-de-pointes: a polymorphic ventricular tachycardia associated
with the long-QT syndromes characterized by phasic variations in the
polarity of the QRS complexes around the baseline. Ventricular rate is
often >200bpm and ventricular fibrillation is a consequence.
Presence of AV dissociation (independent atrial activity) vs. retrograde
atrial capture
Presence of fusion QRS complexes (Dressler beats) which occur when
supraventricular beats (usually sinus) get into the ventricles during the
ectopic activation sequence.
What is the risk?
Depends on
i. Structural heart disease
ii. Ejection fracture
Symptoms:
palpitation, SOB, chest, syncope
D/D OF WIDE QRS TACCHYCARDIA:
SVT with LBBB
SVT with RBBB
Wolf Parkinson white syndrome
Hyperkalemia
AF with preexcitation
Pacemaker mediated tachycardia
SVT with aberrant conduction
26. MAGDI AWAD SASI CARDIAC RHYTHM DISTURBANCE 2013 26
Ventricular fibrillation is life-threatening.
Ventricular fibrillation (v-fib for short) is the most serious cardiac rhythm
disturbance. The lower chambers quiver and the heart can't pump any blood,
causing cardiac arrest.
How it works
The heart's electrical activity becomes disordered. When this happens, the
heart's lower (pumping) chambers contract in a rapid, unsynchronized way. (The
ventricles "flutter" rather than beat.) The heart pumps little or no blood.
Collapse and sudden cardiac arrest follows -- this is a medical emergency!
Signs of cardiac arrest
Sudden loss of responsiveness (no response to tapping on shoulders)
No normal breathing (the victim does not take a normal breath when you
tilt the head up and check for at least five seconds)
Pulse less, Apnea , Centrally cyanosed, convulsion .
This is sudden cardiac arrest (SCA) -- which requires immediate medical
help (CPR and defibrillation)!
Treatment :
Ventricular fibrillation can be stopped with a defibrillator, which gives an
electrical shock to the heart.
27. MAGDI AWAD SASI CARDIAC RHYTHM DISTURBANCE 2013 27
HEART BLOCK------------------------First-degree AV block
• First-degree (AV) block is defined as a fixed prolonged PR interval
exceeding 0.21 seconds with all atrial impulses conducted.
CAUSESE:
1. Athletic training
2. Vascular--Acute MI
3. Drugs:
• Calcium channel blockers,
• Beta-blockers,
• Digoxin,
• Amiodarone
4. Valvular-- Mitral or aortic valve annulus calcification , Rheumatic fever
5. Infectious disease:
• Infective endocarditis,
• Diphtheria,
• Chagas disease,
• Lyme disease,
• Tuberculosis
6.Collagen vascular disease:
• Rheumatoid arthritis
• systemic lupus erythematous
• scleroderma
7.Fetuses of pregnant women who are anti-SSA/Ro positive.
8.Infiltrative diseases such as amyloidosis or sarcoidosis
9.Myotonic dystrophy
28. MAGDI AWAD SASI CARDIAC RHYTHM DISTURBANCE 2013 28
SYMPTOMS:
• Asymptomatic at rest.
• Markedly prolonged PR interval may reduce exercise tolerance in
patients with left ventricular systolic dysfunction.
• Syncope may result from transient high-degree AV block and in
those with infranodal block and wide QRS complex
SIGNS:
• The intensity of the first heart sound (S1) is decreased in patients
with first-degree AV block.
• Patients with first-degree AV block may have a short, soft, blowing,
diastolic murmur heard at the cardiac apex. The diastolic murmur is
thought to be related to antegrade flow through closing mitral
valve leaflets that are stiffer than normal.
TREATMENT:
• Patients with asymptomatic first-degree AV block----no treatment
• In patients with symptomatic first-degree AV block medications with
potential for AV block must be discontinued if possible.
• Permanent electronic pacemakers may be indicated in those with
the following:
1. Severe bradycardia
2. Syncope associated with infranodal block
3. Left ventricular systolic dysfunction, when a shorter AV
delay has been shown to improve hemodynamic condition
• Medications
29. MAGDI AWAD SASI CARDIAC RHYTHM DISTURBANCE 2013 29
COMPLCATIONS:
• Progression to higher degrees of AV block
• Reduction in left ventricular stroke volume and cardiac output
• Pseudo-pacemaker syndrome
PROGNOSIS:
• Isolated first-degree AV block carries no increased risk of mortality.
• Patients with first-degree AV block and infranodal blocks have
increased risk of progression to complete AV block
30. MAGDI AWAD SASI CARDIAC RHYTHM DISTURBANCE 2013 30
Second-degree block:
Mobitz type I (Wenckebach) AV block
Mobitz type II AV block
Mobiz type 1
It is a progressive prolongation of P-Rinterval, with the RR interval shortening,
before the blocked beat; this phenomenon is almost always due to abnormal
conduction within the AV node. (one P in ECG except in one place B/W 2QRSs).
CAUSES:
31. MAGDI AWAD SASI CARDIAC RHYTHM DISTURBANCE 2013 31
It may occur in normal individuals with heightened vagal tone.
1. Drug effect (especially digitalis, calcium channel blockers, β-
blockers, or other sympatholytic agents), often superimposed on
organic disease.
2. These disturbances also occur transiently or chronically due to
A. Ischemia
B. Infarction
C. Inflammatory processes
D. fibrosis
E. Calcification
F. Infiltration.
The prognosis is usually good, since reliable alternative pacemakers arise from
the AV junction below the level of block if higher degrees of block occur.
THE MOST IMPORTANT AETIOLOGY TO BE R/O IS STEMI (INFERIOR WALL).
32. MAGDI AWAD SASI CARDIAC RHYTHM DISTURBANCE 2013 32
Mobitz type II AV block
There are intermittently nonconducted atrial beats not preceded by
lengthening AV conduction. It is usually due to block within the His bundle
system.
The distance of P waves from QRS complexes is fixed but only one P wave pass
through AV node and result in QRS .It is called 2:1 block- 2 P waves, or 3:1
block 3 P waves.
33. MAGDI AWAD SASI CARDIAC RHYTHM DISTURBANCE 2013 33
Mobitz type II block is almost always due to organic disease involving the
infranodal conduction system.
In the event of progression to complete heart block, alternative pacemakers are
not reliable.
Thus, prophylactic ventricular pacing is required.
SUMMARY:
FIRST DEGREE- ONE P /FIXED PROLONGED PR INTERVAL MORE THAN 5 SQ
SECOND DEGREE
MOBIZ 1 - PROGRESSIVE PROLONGATION OF PR INTERVAL
ONE P / EXCEPT IN ONE PLACE 2 P WITH ONE QRS
REVERSIBLE/ BENIGN CONDITION
ACUTE INFERIOR MI
MOBIZ 2 - MANY FIXED P WAVES /FIXED NUMBER AND DISTANCES
3:1 BLOCK, 4:1 BLOCK ONE P ONLY PRODUCE ONE QRS
PACEMAKER IS THE TREATMENT.
ACUTE STEMI CAN CAUSE ALL TYPES OF BLOCK.
ANY PATIENT PRESENTED WITH HEART BLOCK SHOULD ALARM US TO LOOK
FOR DRUGS AND POSSIBILITY OF ACUTE CORONARY SYNDROMES.
34. MAGDI AWAD SASI CARDIAC RHYTHM DISTURBANCE 2013 34
Complete heart block:
Complete (third-degree) heart block is a more advanced form of block often due
to a lesion distal to the His bundle and associated with bilateral bundle branch
block. The QRS is wide and the ventricular rate is slower, usually less than
50 beats/min. Transmission of atrial impulses through the AV node is
completely blocked, and a ventricular pacemaker maintains a slow, regular
ventricular rate, usually less than 45 beats/min. Exercise does not increase the
rate.(( LBBB + RBBB+ 1ST
DEGREE HAERT BLOCK=CHB ))
SYMPTOMS:
Patients may be asymptomatic or may complain of low cardiac output
symptoms- fatigue, sweating, dizziness, lose of effort, weakness or dyspnea if
the rate is less than 35 beats/min; symptoms may occur at higher rates if the
left ventricle cannot increase its stroke output.
The patient may be in shock if it is caused by acute myocardial infarction.
During periods of transition from partial to complete heart block, some patients
have ventricular asystole that lasts several seconds to minutes. Syncope occurs
abruptly.
SIGNS:
The first heart sound varies in intensity
Wide pulse pressure
Changing systolic BP level
Cannon venous pulsations in the neck are also present.
35. MAGDI AWAD SASI CARDIAC RHYTHM DISTURBANCE 2013 35
Treatment
The indications for permanent pacing have been discussed:
Symptomatic bradyarrhythmias,
asymptomatic Mobitz II AV block, or complete heart block
CAUSES OF AV BLOCKS
REVERSIBLE PERMANENT
PHYSIOLOGIC; CAD;
CAD; MATERNAL SLE;
INF. ENDOCARDITIS; CMP;
MYOCARDITIS; INFILTRATIVE;
METABOLIC; TRAUMATIC;
TRAUMATIC; TUMOURS;
DRUG INDUCED; NM DISORDERS;
IDIOPATHIC;