Thoothukudi Call Girls 👙 6297143586 👙 Genuine WhatsApp Number for Real Meet
Cbimci
1.
2. IMCI
IMCI strategy was developed by WHO in collaboration with
UNICEF, Government of Nepal decided to introduce it in
June 1995 in Nepal.
It is a curative, preventive and promotive strategy aimed at
reducing the death , severity of illness and disability which
contributes to improve growth and development of under 5
children.
Nepal is almost the first two countries in SEARO region to
start IMCI ( another country being Indonesia). It was initially
implemented in Mahottari and Nawalparasi districts.
By the year 2066, it is implemented in all districts, since
then training started from health facility (HPSHP) to the
community level (VHW MCHW and FCHV)
3. CBIMCI
The community based ARI and CDD (CBAC)
program was merged into IMCI in 1999 and was
named the CBIMCI.
New born care component included in CB-IMCI in
2004 and name given as CB- NCP.
Integrated package of CBIMCI and CBNCP was
implemented as IMNCI from 207172.
4. OBJECTIVES
To reduce under 5 mortality, morbidity and disability
due to pneumonia, diarrhoea, malnutrition, measles
and malaria.
To contribute to improved child growth and
development of under 5 children.
5. COMPONENTS
Improving knowledge and case management skills of
health service providers.
Improvements in the health system required for effective
management of childhood illness.
Improvement in family and community practice.
6. IMCI GUIDELINES ARE BASED ON THE
FOLLOWING PRINCIPLES
All sick children under 5 years of age must be examined for
conditions which indicate immediate referral or
hospitalization.
Children must be routinely assessed for major symptoms,
nutritional and immunization status, feeding problems and
other potential problems.
Based on the presence of selected clinical signs, the child
is placed in a ‘classification’. Classifications are not specific
diagnosis but categories that are used to determine the
treatment.
7. CONTINUATION
Classifications are color coded and suggest referral (pink),
treatment in health facility (yellow) or management at
home (green).
A limited number of essential drugs are used.
Caretakers are actively in the treatment of children.
Counselling of caretakers about home care including
feeding, fluids and when to return to health facility.
8. STRATEGIES OF CB-IMCI
PROGRAMME
1. Recognition of the danger signs of diseases.
2. Timely referral to nearby health facilities and
3. Improve community support for CDD, ARI, Nutrition and
Immunization through group participation and
programme management.
9. APPROACHES OF IMCIIMCI CASE MANAGEMENT
PROCESS
Steps of case management process are as follows
Assess the young infant and child
Classify the illness
Identify treatment
Treat the young infant and child
Counsel the mother
Provide follow up care
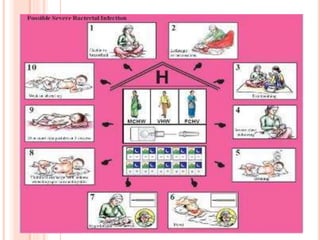
10. SUMMARY OF THE INTEGRATED CASE MANAGEMENT PROCESS
For all sick children age 1 week up to 5 years who are brought to a first-level health facility
ASSESS the child: Check for danger signs (or possible bacterial infection). Ask about main symptoms. If a
main symptom is reported, assess further. Check nutrition and immunization status. Check for other
problems.
CLASSIFY the child’s illnesses: Use a colour-coded triage system to classify the child’s main symptoms
and his or her nutrition or feeding status.
IF URGENT REFERRAL is needed and possible IF NO URGENT REFERRAL is needed or possible
IDENTIFY URGENT
PRE-REFERRAL TREATMENT(S)
needed for the child’s classifications.
.
IDENTIFY TREATMENT needed for the child’s classifications:
Identify specific medical treatments and/or advice.
TREAT THE CHILD: Give urgent pre-
referral treatment (s) needed.
TREAT THE CHILD: Give the first dose of oral drugs in the clinic
and/or advise the child’s caretaker. Teach the caretaker how to
give oral drugs and how to treat local infections at home. If needed,
give immunizations.
REFER THE CHILD: Explain to the
child’s caretaker the need for referral.
Calm the caretaker’s fears and help
resolve any problems. Write a
referral note. Give instructions and
supplies needed to care for the child
on the way to the hospital.
COUNSEL THE MOTHER: Assess the child’s feeding, including
breastfeeding practices, and solve feeding problems, if present.
Advise about feeding and fluids during illness and about when to
return to a health facility. Counsel the mother about her own
health.
FOLLOW-UP care: Give follow-up care when the child returns to the
clinic and,if necessary, reassess the child for new problems.
11. ASSESS THE YOUNG INFANTCHILD
o Ask for the child’s name and age.
o After this, the age of the child is divided into two
categories:- sick infant upto 2 months and a sick child 2
months to 5 years.
o In the first week of life, newborn infants are often sick from
conditions related to labor and delivery or they have
conditions which require special management.
o Newborns may suffer from asphyxia, sepsis from
premature ruptured membranes or other intrauterine
infections or birth trauma, or they may trouble breathing
due to immature lungs. Jaundice also requires special
management in the first week of life.
12. CLASSIFY THE ILLNESS
Classify the severity of sickness by using following colour:-
1. Green colour :- Home management
2. Yellow colour:- management in outpatient basis in the
hospital
3. Pink colour:- For urgent referral cases
13. IDENTIFY THE TREATMENT
In this required treatments are listed.
According to classification, treatment required for all the
classifications must be identified according to IMCI
guideline.
After classifying all conditions, identify specific treatments
for the child. If a child requires urgent referral, give
essential treatment before the patient is transferred.
If a child needs treatment at home, develop an integrated
treatment plan for the child and give the first dose of drugs
in the clinic. If a child should be immunized, give
immunizations.
14. TREAT THE YOUNG INFANTCHILD
Treat the young infant child based on the
classification and treatment identified.
Child is managed with pre-referral treatment for
severe classification and referred urgently for
higher centre.
15. PRE-REFERRAL TREATMENT INCLUDES
Administration of anticonvulsive drugs such as
Diazepam 0.2mgkg IV or rectally and repeat the
dose after 10 minutes if convulsion is continued.
Use Phenobarbital 20mgkg IM to control
convulsion in infants less than 2 weeks of age.
Prevent low blood sugar by giving breast milk or
sugar water.
Warm the young infant by skin to skin contact if
temperature is less than 36.5⁰C while arranging
referral. Advice mother how to keep the infant warm on
the way to the hospital.
16. CONTINUATION
IV infusion to prevent dehydration.
Single dose of IV Ceftriaxone 100mgkg or
Cefotaxime 50mgkg can also be employed as pre-
referral therapy.
17. CONTINUATION
CHILD WITH YELLOW COLOUR IDENTIFICATION TAG IS
TREATED AT OPD IN HEALTH CARE FACILITIES THAT
INCLUDES:-
1. Treat local infection
2. Give oral drugs
3. Advice and teach caretakers and follow up care.
CHILD WITH GREEN COLOUR IDENTIFICATION TAG IS
TREATED AT HOME SETTING BY:-
1. Giving oral drugs
2. Treat local infection
3. Continue exclusive breast feeding
4. Keep child warm and follow up visit.
18. COUNSEL THE MOTHER
COUNSELING INCLUDES:-
Giving information about the:-
1. Continuous treatment of children,
2. Follow up visit,
3. Signs that need immediate visit in hospital,
4. Mother’s general health conditions including
immunization, iron supplementation to mother,
family planning and counselling on STD and AIDS
prevention.
19. FOLLOW UP CARE
THE CARE PROVIDER SHOULD:-
1. Teach mother about signs that mean return immediately for
further care.
2. Advice when to return for follow up.
3. Schedule the next well child immunization visit.
ADVICE MOTHER IMMEDIATELY IF THE FOLLOWING
CONDITION PREVAIL:-
1. The baby not being able to suck or poor sucking.
2. Has fever
3. Become sicker
4. Has fast breathing
5. Diarrhoea and has pale sole and palm.
20. WHEN THE CHILD IS BROUGHT TO THE
CLINIC
Use Good Communication Skills:
Listen carefully to what the mother tells you
Use words the mother understands
Give time for mother to answer questions
Ask additional questions when mother not sure
of answer
Record important information
22. PNEUMONIA
Pneumonia is defined
as the infection and
inflammation of the
lung parenchymal
tissues that impairs gas
exchange.
It may occur as primary
infection or secondary
to upper respiratory
tract infection.
23. NORMAL RESPIRATION RATE
Age Normal Range (Resting)
Premature 40-70
0-3 months 35-55
3-6 months 30-45
6-12 months 25-40
1-3 years 20-30
3-6 years 20-25
6-12 years 14-22
Over age 12 12-18
25. CLINICAL ASSESSMENT
Note the age of child
For how long a child is coughing?
Whether the child is able to drink (if the child is
aged from2 months to 5 year) ?
Has the infant stopped feeding well(child <2
months)?
Does the child have fever, is the child excessively
drowsy or difficult to wake (if yes, for how long?)
Did the child have convulsions, is there irregular
breathing?
26. PHYSICAL EXAMINATION
LOOK & LISTEN FOR THE FOLLOWING :-
1. Count the breath in one minute
2. Look for chest indrawing
3. Listen for stridor
4. Listen for wheeze
5. Look if the child is abnormally sleepy or difficult to wake.
6. Feel for fever.
7. Check for severe malnutrition
8. Check for cyanosis as a sign of hypoxia.
27. •Chest indrawing or
•Stridor in calm child. SEVERE
PNEUMONIA
•Give first dose of an appropriate
antibiotic.
•Refer URGENTLY to hospital.
•Treat fever if present
•Treat wheezing if present.
•Fast
breathing(>=50minute if
the child is 2 to 12 months;
>=40 for the child of 12
months upto 5 years)
PNEUMONIA
•Advice the mother to give home care.
•Give an appropriate oral antibiotic.
•Soothe the throat and relieve the cough
with a safe remedy.
•Advise mother when to return with
child in 2 days for reassessment, or
earlier if child is getting worse.
No signs of pneumonia
or very severe disease.
NO
PNEUMONIA:
COUGH OR
COLD
•If coughing more than 30 days, refer for
assessment.
•Assess and treat ear problem or sore
throat if present.
•Advise mother to give home care.
•.treat fever and wheezing if present.
CLASSIFICATION TABLE FOR PNEUMONIA
SIGNS CLASSIFY AS
IDENTIFY TREATMENT
(Urgent pre-referral treatments are in bold print.)
28. TREATMENT
FOR PNEUMONIA (child with cough and fast breathing)
1. Cotrimoxazole (Trimethoprim/Sulfamethoxazole) is the
drug of choice for the treatment of pneumonia.
AGEWEIGHT DOSE(tab) DOSE(syrup)
<2 months
(Wt. 3-5kg)
1 tab twice a day Half spoon (2.5ml) twice a day
2-12 months
(Wt. 6-9 kg)
2 tablet twice a day One spoon (5ml) twice a day.
1-5 years
(wt. 10-19kg)
3 tablet twice a day One & half spoon (7.5ml) twice
a day.
29. CONTINUATION
FOR SEVERE PNEUMONIA (chest indrawing)
Children with severe pneumonia should be treated as
inpatients with intramuscular injections of benzyl penicillin
(after test dose), Ampicillin or Chloramphenicol.
The condition of the child must be monitored every day
and reviewed after 48 hours for antibiotic therapy.
Antibiotic therapy must be given for a minimum of 5 days
and continued for at least 3 days after the child gets well.
30. CONTINUATION ( FOR 2MONTH TO 5 YEAR)
Antibiotics Dose Interval Mode
A. 1st 48 hours Benzyl penicillin or
Ampicillin or Chloramphenicol
50000 IUkg
50mgkg
25mgkg
6 hourly
6 hourly
6 hourly
IM
IM
IM
B. 1. If condition IMPROVES, then for the next 3 days give:
Procaine Penicillin 50000 IUkg once IM or Ampicillin 50mgkgdose orally or
Chloramphenicol 25mgkgdose 6 hourly orally.
B.2. If NO IMPROVEMENT, then for the next 48 hours;
CHANGE ANTIBIOTIC
If Ampicillin is used changed to Chloramphenicol IM;
If Chloramphenicol is used, change to Cloxacillin 25mgkgdose, every 6 hours
along with Gentamycin 2.5mgkgdose, every 8 hours.
If condition improves continue treatment orally.
31. TREATMENT OF PNEUMONIA UNDER 2 MONTHS
OF AGE
The child must be hospitalized.
Treatment with Cotrimoxazole may be started with
health worker before referring the child.
Antibiotics Dose Frequency
Age <7 days Age 7 days to 2
months
Inj.Benzyl Penicillin 50000IUkg 12 hourly 6 hourly
Inj. Ampicillin 50mgkg 12 hourly 8 hourly
Inj. Gentamycin 2.5mgkg 12 hourly 8 hourly
32. C. Provide symptomatic treatment for fever and wheezing, if required.
D. Monitor fluid and food intake.
E. Advice mother on home management on discharge.
33. CONTINUATION
Besides antibiotics, treatment for the associated
conditions, if any, must be instituted immediately.
The child should be kept warm and dry.
Breast feeding must be promoted strongly.
34. TREATMENT OF CHILD WITH NO PNEUMONIA
Many children with presenting symptoms of cough,
cold and fever do not have pneumonia and do not
require treatment with antibiotics.
Symptomatic treatment and care at home is
generally enough for such cases.
The mother must be advised how to take care of
the child at home.
35. PREVENTION OF PNEUMONIA
1. Good hygiene practices
2. Appropriate handling and disposal of respiratory
secretions of the infected persons.
3. Maintenance of warm well ventilated environment.
4. Special protection during weather variation to
prevent cold.
5. Maintenance of nutritional status of the children.
6. Immunization to be completed as per schedule.
7. Use of home remedies for cough and cold e.g.
tulasi, honey, zinger hot drinks etc.
36.
37. DIARRHOEA
DEFINITION OF DIARRHOEA
Diarrhoea is defined as the passage of loose, liquid or watery
stool more than three times in 24 hours.
DYSENTRY
Diarrhoea with blood in the stool, with or without mucus, is
called dysentery. The most common cause of dysentery is
Shigella bacteria.
INCIDENCE
It is more common in children, especially those between 6
months to 2 years of age.
38. TYPES OF DIARRHOEA
1. Acute Diarrhoea
2. Chronic (persistent) Diarrhoea
ACUTE DIARRHOEA
Acute diarrhoea as an attack of sudden onset,
which usually last 3-7 days, may last upto 10-14
days.
About 10% of acute diarrhoeal episodes become
chronic persistent diarrhoea.
39. CONTINUATION,,
CHRONIC (PERSISTENT) DIARRHOEA
If diarrhoea last for more than 2 weeks and may vary
from day to day, is termed as chronic (persistent)
diarrhoea.
It is usually associated with malabsorption syndrome,
chronic inflammatory bowel disease and food allergies.
40. CAUSES
1. Viral causes:- common viruses are Rota virus, Astro virus,
Adeno virus, Norwalk virus group, Corona viruses &
Entero virus.
2. Bacterial causes:- Common bacteria are Escherichia coli,
Shigella, Salmonella, Vibrio Cholera, Bacillus cereus,
Compylovbacteria jejuni.
3. Protozoal causes :- Entamoeba Histolytica, Giardia
lamblia.
4. Other causes:- worm infestations, allergic diarrhoea due to
milk protein, metabolic diarrhoea due to
Galactosaemia,etc. Emotional stress induces diarrhoea.
41. SIGN AND SYMPTOMS OF DIARRHOEA
Loose watery stool
Vomiting
Thirsty
Lose of skin elasticity
Sunken eyes
Blood and mucus in
Stool
Fever
Lethargy
Dehydration
Abdominal pain and
cramps
42. SIGN AND SYMPTOMS OF DEHYDRATION
Restless, Irritable,
Lethargic or
Unconsciousness
Sunken eyes
Tears absent
Dry mouth with coated
tongue
Thirsty, drinks poorly or
not able to drink
Loss of skin elasticity
Urine not passed or low
in volume
43. ASSESSMENT OF DEHYDRATION
A B C
1. Ask about
• Diarrhoea
• Vomiting
• Thirst
• Urine
<4 liquid stoolsday
None or small amount
Normal
Normal
4-10 liquid stoolsday
Some
> Normal
Small amount & dark
>10 liquid stoolsday
Very frequent
Unable to drink
No urine for 6 hours
2. Look at
Condition
Eyes
Tears
Mouth& tongue
Breathing
Well, alert
Normal
Present
Moist
Normal
Restless, irritable or sleepy,
unwell
Sunken
Absent
Dry
Faster than normal
Lethergic or unconscious,
floppy
Very sunken and dry
Absent
Very dry
Very fast and deep
3. Feel
Skin pinch
Pulse
Goes back quickly
Normal
Goes back slowly
Faster than normal
Goes back very slowly
Very fast weak or cannot feel
44. CLASSIFICATION OF DEHYDRATION
Signs Classify as Identify treatment (plan C)
Two of the following
signs:-
Lethargic or
unconscious
Sunken eyes
Not able to drink or
drink slowly
Skin pinch goes back
very slowly
SEVERE
DEHYDRATIO
N
If child has no other severe
classification
•Give fluid for severe dehydration
OR
If a child have other severe
classification
Refer urgently to the hospital with
mother giving frequent sips of ORS
on the way
Advice continue breastfeeding
If child is 2 year or older and there
is cholera in your area then give
antibiotic for cholera.
45. CONTINUATION
Signs Classify as Treatment (Plan B)
Two of the following
sins:-
Restlessness,
irritable
Sunken eyes
Drinks eagerly,
thirsty
Skin pinch goes
back slowly
SOME
DEHYDRATION
Give fluid and food for some
dehydration
If child also have severe
classification
oRefer URGENTLY to hospital
with mother giving frequent sips
of ORS on the way.
oAdvice the mother to continue
breastfeed.
oAdvice mother when to return
immediately
oFollow-up in 5 days if not
improving.
46. CONTINUATION
Signs Classify as Treatment (Plan A)
Not enough signs to
classify as some or
severe dehydration
NO DEHYDRATION Give fluid and food to
treat diarrhoea
Advice mother when to
return immediately
Follow-up in 5 days if
not improving
47. PRINCIPLES OF DIARRHOEA MANAGEMENT
Assessment of the children’s condition
Identify level of dehydration
Correction of dehydration
Proper nutritional care
Treatment of underlying causes and associated
problems
Treatment of complications
Prevention of dehydration
48. TREATMENT PLAN FOR DEHYDRATION ACCORDING TO
IMCI GUIDELINE
No dehydration: Plan A treatment
Some dehydration : Plan B treatment
Severe dehydration: Plan C treatment
49. NO DEHYDRATION: PLAN ‘A’
TREATMENT
1. Give extra fluid with
continue feeding :
If the child is exclusively
breastfeed, give ORS or
clean water in addition to
breast milk.
If the child is not exclusively
breastfeed, give one or
more of the following: ORS,
food based fluids (such as
Rice-water, soup or salted
sugar solution and yogurts
drinks) or plain water.
Teach the mother how to
mix and give ORS.
50. CONTINUATION
Upto 2 years of age: 50 to 100ml after each loose
stool upto 500mlday.
Two years of age or more: 100 to 200ml after each
loose stool upto 1000mlday.
More than 10 years as much as child want upto
2000mlday.
51. SOME DEHYDRATION:- PLAN ‘B’ TREATMENT
For obvious signs of dehydration oral fluid therapy
for correction of dehydration,
- Give recommended amount of ORS over first 4
hours.
- Determine amount of ORS to give during first 4
hours.
Age <4months 4-11months 12-23
months
2-4years 5-14years 15 years
or more
Weight
in kg
<5kg 5-7.9kg 8-10.9kg 11-15.9kg 16-29.9kg 30kg or
more
Fluid in
ml
200-400ml 400-600ml 600-800ml 800-
1200ml
1200-
2200ml
2200-4000
52. FOR SEVERE DEHYDRATION: PLAN ‘C’
TREATMENT
Start IV fluid immediately. If the child can drink give
the ORS by mouth while the drip is setup.
Give 100mlkg RL or if available, normal saline
divided as follows:
Age First give
30mlkg in:
Then give
70mlkg in:
Infant under 12 months 1 hour 5 hours
Children 12 to 60 months 30 minutes
(30mlkg)
2⅟2 hrs (70mlkg)
53. CONTINUATION
Repeat once if radial pulse is very weak or not
detectable.
Reassess the child every 1-2 hourly. If hydration status
is not improving, give IV drip more rapidly.
Give ORS (about 5mlkghrs as soon as the child can
drink: usually after 3-4 hours infants or 1-2hrs older
child.
Reassess an infant 6 hourly and a child after 3 hourly.
After this classify dehydration and choose the
appropriate plan to continue treatment.
54. CONTINUE
If IV line is not available, start Rehydration by tube or
mouth with ORS solution. Give 20mlkghrs for 6 hours
(total of 120 mlkg).
Reassess the child every 1-2 hourly: If there is repeated
vomiting or increasing abdominal distension, give the fluid
more slowly.
Besides rehydration therapy, antimicrobial therapy may
also be needed for treatment of associated consequences
such as dysentery, persistent diarrhoea cholera etc.
In case of dysentery, treat with oral antibiotics for 5 days
and ask for follow up in 2 days.
55. PREVENTION OF DIARRHOEA
Exclusive breast feeding for 6 months of life and
continue breast feeding upto 2 years of age.
Timely weaning.
Giving freshly prepared foods and clean safe
drinking water to child.
Discourage bottle feeding.
Follow proper hand washing technique and teach
child accordingly.
Proper disposal of human excreta and use of toilet.
56. CONTINUATION
Having your child immunized against preventable
communicable diseases.
Public awareness regarding Government policies.
Use of zinc supplementation, at a dosage of 20
milligrams per day for children older than six
months or 10 mg per day in those younger than six
months, for 10–14 days.
Health education on environmental and personal
hygiene.
57. MEASLES (RUBEOLA)
Measles is a highly
contagious viral disease
manifesting with fever,
cough, coryza,
lacrimation and koplik
spot in the pre-eruptive
phase.
It is caused by Morbilli
virus of Paramyxo virus
family.
60. POST MEASLES STAGE
Rashes starts disappearing after 4-5 days in the
same order in which it appeared.
The temperature comes down.
Fever and rashes last for one week.
The patient may have anorexia, malaise.
61.
62. CLASSIFICATION OF MEASLES
Signs Classify as Treatment plan
•Any general danger sign or
•Clouding of cornea or
•Deep or extensive mouth
ulcers
SEVERE COMPLICATED
MEASLES
Give vitamin A
Give first dose of an appropriate
antibiotic
If clouding of the cornea or pus
draining from the eye, apply
tetracycline eye ointment
Refer urgently to hospital
•Pus draining from the eye or
•Mouth ulcers
MEASLES WITH EYE
OR MOUTH
COMPLICATIONS
•Give vitamin A.
•If pus draining from the eye, treat
eye infection with tetracycline eye
ointment.
•If mouth ulcers, treat with gentian
violet
•Follow up on 2 days.
Measles now or within the
last 3 months
MEASLES Give vitamin A.
63. MANAGEMENT ACCORDING TO IMCI
GUIDELINE
SEVERE COMPLICATED MEASLES
DIAGNOSIS
a. Clinical presentations above and any one of the following
symptomssigns: vomiting everything, inability to drink or
breastfeed and convulsion.
b. On examination: presence of signs of complication after
the rash has disappear i.e. lethargy or unconsciousness,
corneal clouding, deep and extensive mouth ulcer,
pneumonia, diarrhoea, stridor and severe malnourished.
64. CONTINUATION
TREATMENT
Admit the child in the hospital
Give Vitamin A therapy unless the child already had
adequate vitamin to prevent from blindness.
Dose is 2 lakh units orally for children more than 1
years of age. 1st dose immediately, 2nd dose on the
next day & 3rd dose in 2-4 weeks after the 2nd dose
in follow up visit if the child shows signs of Vitamin
A deficiency or severely malnourished.
65. CONTINUATION
Supportive care: Isolation, care & maintain
respiratory hygiene, bed rest during prodermal
stage, antipyretic for fever, nutritional support,
continue breastfeeding, frequent small meal, check
and care of mouth ulcer, eye care and skin care.
Monitor fever twicc a day and also monitor signs of
complication.
Follow up: Ask mother to return immediately if any
complication arises.
66. MEASLES WITH EYE OR MOUTH
COMPLICATIONS
DIAGNOSIS
Measles rash or if the child has; fever generalized
rash and one of the following (cough, running nose
or red eyes) but no features of severe measles.
TREATMENT
Treatment in outpatient, give Vitamin A.
67. CONTINUATION
SUPPORTIVE CARE
Give paracetamol for fever
Treatment of secondary infection if present
Nutritional support
Eye care with clean cotton in boiled cooled warm
water and apply tetracycline eye ointment three
times a day for 7 days.
If infection is present, give mouth care with clean
salted water if mouth sore present and ask to come
for follow up in 2 days.
68. PREVENTION OF MEASLES
Isolation. Measles is highly contagious from about
four days before to four days after the rash breaks
out, people with measles shouldn't return to
activities in which they interact with other people
during this period.
It may also be necessary to keep non immunized
people away from the infected person.
Vaccinate:- MR vaccine ( 9 and 15 month)
71. COMMON FORMS OF MALNUTRITION
Protein energy malnutrition (PEM) refers to
inadequate availability or absorption of energy and
proteins in the body.
Micronutrients deficiency disorder:- deficiency of
micro elements such as Iron, Iodine, Calcium, Zinc
in the body.
72. INDICATOR OF MALNUTRITION
Stunting :- Low height for age-indicate chronic
malnutrition, due to prolonged food deprivation, or
disease.
Wasting: Low weight for Height indicate acute
malnutrition.
Underweight: low weight for age.
73. ASSESSMENT OF
MALNUTRITION
LOOK FOR VISIBLE SEVERE WASTING
If a child is very thin, has no fat, and looks like skin and
bones he may be having marasmus.
To look for visible severe wasting, remove the child’s
clothes. Look for severe wasting of the muscles of the
shoulders, arms, buttocks and legs.
Look to see if the outline of the child’s ribs is easily seen.
Look at the child’s hips. They may look small.
Look at the child from the side to see if the fat of the
buttocks is missing.
When wasting is extreme, there are many folds of skins on
the buttocks and thigh.
74. CONTINUATION
LOOK FOR PALMAR PALLOR
Pallor is unusual paleness of the skin. It is a sign of anaemia.
To see if the child has Palmar pallor, look at the skin of the
child’s palm.
Hold the child’s palm open by grasping it gently from the
side.
Do not stretch the fingers backwards. This may cause pallor
by blocking the blood supply.
Compare the colour of the child’s palm with your own palm
and with the palms of other children.
If the skin of the child’s palm is pale, the child has some
palmar pallor.
If the skin of the palm is very pale it looks white, the child
has severe palmar pallor.
75. CONTINUATION
LOOK AND FEEL FOR OEDEMA OF BOTH FEET
A child with oedema of both feet may have kwashiorkor.
Oedema is when an unusually large amount of fluid
gathers in the child’s tissues. The tissues become filled
with the fluid and look swollen or puffed up.
Look and feel to determine if the child has oedema of
both feet.
Use your finger to press gently for a few seconds on the
top side of each foot.
The child has oedema if a dent remains in the child’s
foot when you lift your finger.
76. DETERMINE WEIGHT FOR AGE
Weight for age compares
the child’s weight with the
weight of other children
who are the same age.
Identify children whose
weight for age is below the
bottom curve of a weight for
age chart.
Children who are below the
bottom curve are very low
weight and need special
attention to how they are
fed.
To determine weight for
age:
1. Calculate the child’s age
in months.
2. 2. Weigh the child
accurately.
77. CONTINUATION
3. Use the weight for age chart to determine weight for
age. — Look at the left-hand axis to locate the line that
shows the child’s weight. — Look at the bottom axis of the
chart to locate the line that shows the child’s age in
months.
4. Decide if the point is above, on, or below the bottom
curve. — If the point is below the bottom curve, the child
is very low weight for age. — If the point is above or on
the bottom curve, the child is not very low weight for age.
78. CLASSIFICATION OF MALNUTRITION & ANAEMIA
Signs Classify as Identify treatment
Visible severe wasting or
Severe palmer pallor or
Oedema of both feet
SEVERE
MALNUTRITION
OR SEVERE
ANAEMIA
Give Vitamin A
Refer urgently to hospital
Keep child warm while referring
Some pallor or
Very low weight for age
ANAEMIA OR
VERY LOW
WEIGHT
Assess the child’s feeding and counsel the
mother on feeding .If feeding problem ,
follow up in 5 days.
If pallor
-Give iron
-Give Antimalarial if high malarial risk
-Give Mebendazole if child is 2 year or older
and has not had a dose in previous 6
months.
Advice mother when to return immediately
If pallor, follow-up in 14 days.
If very low birth for age, follow-up in 30
days.
Not very low weight for age
and no other signs of
malnutrition
NO ANAEMIA
NOT VERY LOW
WEIGHT
If child is less than 2 years old, assess the
child’s feeding and counsel the mother on
feeding.
If feeding problem, follow-up in 5 days.
Advice mother when to return immediately.
79. TREATMENT OF SEVERE MALNUTRITION OR
SEVERE ANAEMIA
If the child has visible severe wasting, severe palmar
pallor or oedema of both feet, classify the child as
having SEVERE MALNUTRITION OR SEVERE
ANAEMIA. These Children need urgent referral to
hospital where their treatment can be carefully
monitored.
They may need special feeding, antibiotics or blood
transfusions. Before the child leaves for hospital, give
the child a dose of vitamin A.
80. TREATMENT OF ANAEMIA OR VERY LOW
WEIGHT
If the child is very low weight for age or has some palmar pallor,
classify the child as having anaemia or very low weight.
While recording this classification, just write ANAEMIA if the child
has only palmar pallor or VERY LOW WEIGHT if the child is only
very low weight for age.
Assess the child’s feeding and counsel the mother about feeding
her child.
A child with some palmar pallor may have anaemia. Treat the
child with iron.
The anaemia may be due to Malaria or Hookworm. Give an
Antimalarial for malarial risk. Give the child Mebendazole only if
there is hookworm in the area.
Only give Mebendazole if the child with anaemia is 2 years of
age or older and has not had a dose of Mebendazole in the last 6
months.
81. TREATMENT OF NO ANAEMIA AND NOT
VERY LOW WEIGHT
If the child is not very low weight for age and there are no
other signs of malnutrition, classify the child as having
NO ANAEMIA AND NOT VERY LOW WEIGHT.
Children less than 2 years of age have a higher risk of
feeding problems and malnutrition than older children do.
If the child is less than 2 years of age, assess the child’s
feeding.
Counsel the mother about feeding her child.
82. PREVENTION OF MALNUTRITION
1. Growth monitoring
2. Oral rehydration therapy
3. Breast feeding
4. Immunization
5. Parents education on; birth spacing, child care,
maternal health status, periodic health check-up.
83. MALARIA
Malaria is a Protozoal
disease caused by
arthropod borne infection
with malarial parasite
(plasmodium), which is
transmitted by infected
female Anopheline
mosquito.
Malaria is found about 100
countries in the world.
84. CAUSES
Malaria is caused by four distinct species of the
malaria parasite:-
1. P. vivax
2. P. falciparum
3. P. malariae
4. P. ovale
85. MODE OF TRANSMISSION
Mainly vector transmission by female anopheline
mosquito.
Anyone having malaria should not be accepted as
blood donor until three years.
Congenital malaria rarely may occur to the newborn
from an infected mother.
86. INCUBATION PERIOD
Incubation period varies depending upon the types of
parasite.
1. 9-14 days for P. falciparum
2. 8-17 days for P. Vivax
3. 16-18 days for P. malariae
88. COLD STAGE
The onset is with lassitude, headache, nausea and
chilly sensation followed by rigors.
Rise in temperature rapidly to 39-41˚C.
In starting skin feels cold later it becomes hot.
Pulse is rapid.
Parasite is usually demonstratable in blood.
This stage lasts for 1 hour.
89. HOT STAGE
Patient feels burning hot and casts off his clothes.
The skin is hot and dry to touch.
Headache is intense but nausea commonly
diminishes.
The respiration is rapid.
This stage is lasts for 2 to 6 hours.
90. SWEATING STAGE
Fever comes down with profuse sweating.
The temperature drops rapidly to normal and skin is
cool and moist.
Pulse rate becomes slower.
Patient feels relieved and often falls asleep.
This stage lasts for 2-4 hours.
91. CLASSIFICATION OF MALARIA
Signs Classify as Treatment
•Any general
danger sign
•Stiff neck
VERY
SEVERE
FEBRILE
DISEASE
Give quinine for severe malaria (1st dose)
Give 1st dose of an appropriate antibiotic
Treat the child to prevent low blood sugar
Give one dose of paracetamol in clinic for high fever
(38.5˚C or above).
Refer URGENTLY to hospital
No runny nose &
no measles & no
other cause of
fever.
MALARIA •If no cough with fast breathing, treat with oral Antimalarial
OR
•If cough with fast breathing, treat with cotrimoxazole for 5
days.
•Give 1 dose of paracetamol in clinic for high fever.
•Advice mother when to return immediately.
•Follow-up in 2 days if fever persists.
•If fever is present every day for more than 7 days, REFER
for assessment.
•Runny nose
PRESENT OR
•Measles
PRESENT OR
•Other cause of
fever PRESENT
FEVER-
MALARIA
UNLIKELY
•Give one dose of paracetamol in clinic for high fever.
•Advise mother when to return immediately.
•Follow-up in 2 days if fever persists.
•If fever is present every day for more than 7 days, REFER
for assessment.
92. DIAGNOSIS
History collection
Physical examination
Blood smear test
Blood test ( will show severe anemia&
hypoglycemia)
Lumbar puncture to exclude meningitis
93.
94. PREVENTION OF MALARIA
Malaria can often be avoided using the ABCD approach to
prevention, which stands for:
Awareness of risk – find out whether you're at risk of
getting malaria
Bite prevention – avoid mosquito bites by using insect
repellent, covering your arms and legs, and using a
mosquito net
Check whether you need to take malaria prevention
tablets – if you do, make sure you take the right
Antimalarial tablets at the right dose, and finish the
course.
Diagnosis – seek immediate medical advice if you
have malaria symptoms, including up to a year after you
return from travelling