9.gall bladder
•Descargar como PPT, PDF•
6 recomendaciones•423 vistas

9.gall bladder (pathology)

Recomendados
Más contenido relacionado
La actualidad más candente
La actualidad más candente (20)
Similar a 9.gall bladder
Similar a 9.gall bladder (20)
Más de PNK SINGH
Más de PNK SINGH (20)
Último
Último (20)
9.gall bladder
- 1. Pathology of Gall BladderPathology of Gall Bladder
- 2. Gallstones (cholelithiasis)Gallstones (cholelithiasis) Gallstones are the most common biliary pathology.Gallstones are the most common biliary pathology. Gallstones are classified according to their chemical compositionGallstones are classified according to their chemical composition intointo 1.Cholesterol stones,1.Cholesterol stones, SolitarySolitary( cholesterol( cholesterol solitairesolitaire) upto 2-3cm or) upto 2-3cm or Mulberry shapedMulberry shaped stonesstones Pale or yellow, round to ovalPale or yellow, round to oval
- 3. 2. Pigment stones.2. Pigment stones. Black (sterile) or brown (infected)Black (sterile) or brown (infected) Composed of calcium salts of unconjugated bilirubin.Composed of calcium salts of unconjugated bilirubin. They are mostly small (<1cm) and multiple.They are mostly small (<1cm) and multiple. 3.Mixed stones and3.Mixed stones and Mixed stones account for 75-90 per cent of gallstones.Mixed stones account for 75-90 per cent of gallstones. Cholesterol is the major component.Cholesterol is the major component. Other components include calcium bilirubinate, calcium phosphate,Other components include calcium bilirubinate, calcium phosphate, calcium carbonate, calcium palmitate and proteins.calcium carbonate, calcium palmitate and proteins. Usually they are multiple, and they are often faceted.Usually they are multiple, and they are often faceted.
- 4. Pigment gallstones. from a patient with a mechanical mitral valve prosthesis, leading to chronic hemolysis
- 5. Risk Factors for cholesterol stone (4F)Risk Factors for cholesterol stone (4F) FFemale genderemale gender Obesity (Obesity (FFatty)atty) Pregnancy (Pregnancy (FFertile)ertile) Oral contraceptives and hormone replacement therapy (HRT)Oral contraceptives and hormone replacement therapy (HRT) Bile StasisBile Stasis Incidence increases with age (Incidence increases with age (FForty)orty) Risk factors for pigment stoneRisk factors for pigment stone Chronic hemolytic anemiasChronic hemolytic anemias CirrhosisCirrhosis Biliary infectionBiliary infection
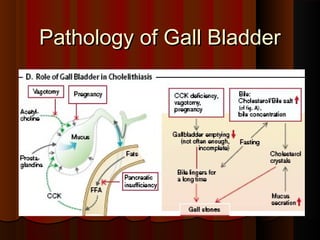
- 6. AetiologyAetiology (Cholesterol)(Cholesterol) The aetiology is probably multifactorial. Factors implicated areThe aetiology is probably multifactorial. Factors implicated are Metabolic (increased cholesterol level)Metabolic (increased cholesterol level) InfectiveInfective Bile stasis.Bile stasis. PathogenesisPathogenesis Factors helping formation of cholesterol Gall stonesFactors helping formation of cholesterol Gall stones Supersaturation of bile with cholesterolSupersaturation of bile with cholesterol Nucleation calcium salts may be the nucleation sites for cholesterolNucleation calcium salts may be the nucleation sites for cholesterol stonesstones GB hypomotility /StasisGB hypomotility /Stasis Accretion - They must remain in the GB long enough choelsterolAccretion - They must remain in the GB long enough choelsterol crystals to agglomerate into stonescrystals to agglomerate into stones
- 7. PathogenesisPathogenesis Factors helping formation of cholesterol Gall stonesFactors helping formation of cholesterol Gall stones Supersaturation of bile with cholesterolSupersaturation of bile with cholesterol Nucleation - calcium salts promotes nucleationNucleation - calcium salts promotes nucleation GB hypomotility – accelerates nucleationGB hypomotility – accelerates nucleation Hyper secretion of GB mucous traps the crystals permitting theirHyper secretion of GB mucous traps the crystals permitting their aggregation into stonesaggregation into stones
- 8. AetiopathogeneisAetiopathogeneis PigmentPigment Increased concentration of pigments – HaemolysisIncreased concentration of pigments – Haemolysis Precipitation of calcium salts of unconjugated bilirubinPrecipitation of calcium salts of unconjugated bilirubin Infection – E. Coli, ascaris lumbricoids, liver flukesInfection – E. Coli, ascaris lumbricoids, liver flukes
- 9. Effects and complications of gallstonesEffects and complications of gallstones In the gall bladder:In the gall bladder: Silent stonesSilent stones Acute cholecystitis –Acute cholecystitis – Empyema, Gangrene, Perforation,Empyema, Gangrene, Perforation, Chronic cholecystitisChronic cholecystitis MucoceleMucocele CarcinomaCarcinoma In the bile ducts:In the bile ducts: Obstructive jaundiceObstructive jaundice CholangitisCholangitis Acute pancreatitisAcute pancreatitis In the intestine:In the intestine: Acute intestinalAcute intestinal obstructionobstruction (gallstone ileus)(gallstone ileus)
- 10. CholecystitisCholecystitis AcuteAcute ChronicChronic Acute cholecystitisAcute cholecystitis 1. Acute calculous cholecystitis1. Acute calculous cholecystitis It is an acute inflammation of the gallbladder, usually caused byIt is an acute inflammation of the gallbladder, usually caused by obstruction of neck or cystic duct by gallstones. (90%)obstruction of neck or cystic duct by gallstones. (90%) 2. Acute acalculous cholecystitis - 10 %2. Acute acalculous cholecystitis - 10 %
- 11. PathogenesisPathogenesis ACC is initially the result of chemical irritation and inflammationACC is initially the result of chemical irritation and inflammation The action of phospholipases derived from the mucosa hydrolyzesThe action of phospholipases derived from the mucosa hydrolyzes biliary lecithin to lysolecithin, which is toxic to the mucosa.biliary lecithin to lysolecithin, which is toxic to the mucosa. Distention and increased intraluminal pressure may alsoDistention and increased intraluminal pressure may also compromise blood flow to the mucosa.compromise blood flow to the mucosa. These events occur in the absence of bacterial infection; only laterThese events occur in the absence of bacterial infection; only later may bacterial contamination develop.may bacterial contamination develop.
- 12. MorphologyMorphology GB is enlarged ,tensed, redGB is enlarged ,tensed, red Shows evidence of acute inflammation- congestion, edema, and Fibrinous orShows evidence of acute inflammation- congestion, edema, and Fibrinous or suppurative exudate on serosasuppurative exudate on serosa On being openedOn being opened Obstructive stone in neck or cystic ductObstructive stone in neck or cystic duct The lumen is filled with cloudy fluid, may contain several stoneThe lumen is filled with cloudy fluid, may contain several stone Empyema of GB – when it contains frank pusEmpyema of GB – when it contains frank pus Wall of GBWall of GB ThickenedThickened Gangrenous cholecystitis – may be necrosis of mucosa with small to largeGangrenous cholecystitis – may be necrosis of mucosa with small to large ulcersulcers It may perforate or ruptureIt may perforate or rupture
- 13. HistologyicallyHistologyically The microscopic features are classical for acute inflammation andThe microscopic features are classical for acute inflammation and include hyperemia, polymorphonuclear leukocyte infiltration, edemainclude hyperemia, polymorphonuclear leukocyte infiltration, edema and in severe cases, necrosis of the wall of the gall bladder.and in severe cases, necrosis of the wall of the gall bladder.
- 14. SequelaeSequelae SubsideSubside Chronic CholecystitisChronic Cholecystitis Sub acute cholecystitisSub acute cholecystitis Porcelain (calcified) GBPorcelain (calcified) GB Carcinoma of GBCarcinoma of GB
- 15. ComplicationsComplications Gangrene of the gallbladderGangrene of the gallbladder Perforation and peritonitisPerforation and peritonitis Fistula formation and gallstone ileusFistula formation and gallstone ileus Ascending cholangitisAscending cholangitis Liver abscess, sub hepatic or subdiaphragmatic abscessLiver abscess, sub hepatic or subdiaphragmatic abscess SepticaemiaSepticaemia
- 16. Mucocele of GBMucocele of GB Distention of GB filled by clear, watery, mucinous secretionDistention of GB filled by clear, watery, mucinous secretion PathogenesisPathogenesis Total obstruction of cystic ductTotal obstruction of cystic duct Trapped bile is absorbedTrapped bile is absorbed GB becomes filled with clear, mucinous secretions from mucosal cellsGB becomes filled with clear, mucinous secretions from mucosal cells AppearanceAppearance Enlarged, tense & translucentEnlarged, tense & translucent Wall becomes thinWall becomes thin
- 17. Chronic cholecystitisChronic cholecystitis It is the continuous chronic inflammation of the gallbladder usuallyIt is the continuous chronic inflammation of the gallbladder usually caused by gallstonescaused by gallstones Aetiology – Probable actorsAetiology – Probable actors Sequelae to acute cholecystitisSequelae to acute cholecystitis Always associated with gall stonesAlways associated with gall stones Supersaturation of bile – (Chemical injury)Supersaturation of bile – (Chemical injury) Infection – enteric bacteriaInfection – enteric bacteria
- 18. MacroscopicMacroscopic GB – contracted, normal or enlargedGB – contracted, normal or enlarged Wall is hypertrophic or atrophicWall is hypertrophic or atrophic Flattening of mucosal folds, thinning & atrophy of mucosaFlattening of mucosal folds, thinning & atrophy of mucosa
- 19. Micro:Micro: Chronic inflammation and Rokitansky-Aschoff sinuses (OutpouchingsChronic inflammation and Rokitansky-Aschoff sinuses (Outpouchings of the mucosa through the wall)of the mucosa through the wall) Late complication:Late complication: Calcification of the gallbladder ("porcelain gallbladder")Calcification of the gallbladder ("porcelain gallbladder") Carcinoma of gall bladder.Carcinoma of gall bladder.
- 20. Carcinoma of GallbladderCarcinoma of Gallbladder Malignant epithelial tumor of the gallbladder, commonly of theMalignant epithelial tumor of the gallbladder, commonly of the adenocarcinoma type.adenocarcinoma type. Squamous cell carcinoma or adenosquamous carcinoma may ariseSquamous cell carcinoma or adenosquamous carcinoma may arise from squamous metaplasisafrom squamous metaplasisa EtiologyEtiology Cancer of the gallbladder is strongly associated with stone disease.Cancer of the gallbladder is strongly associated with stone disease. Even in patients with gallstones, the risk of carcinoma is low.Even in patients with gallstones, the risk of carcinoma is low. PathogenesisPathogenesis Unknown,Unknown,
- 21. Gross PathologyGross Pathology Mass that may be:Mass that may be: diffuse (70%)diffuse (70%) polypoid (30%)polypoid (30%) growing in diffuse fashion in the wall of the gallbladder, associated with extensive involvement of the liver. Adenocarcinoma of the gallbladder having a predominantly papillary configuration.