brief anatomy of larynx and its clinical evaluation
•Download as PPT, PDF•
26 likes•4,685 views

The document provides information on the anatomy and clinical evaluation of the larynx. It describes the larynx's location, cartilages, joints, ligaments, cavities, and complaints that may arise. Examination techniques like indirect and direct laryngoscopy are explained. Indirect laryngoscopy allows visualization of the larynx and vocal cords using a mirror. Direct laryngoscopy provides a more direct view but requires general anesthesia. The document outlines what should be examined during these procedures and common mistakes to avoid.

Recommended
More Related Content
What's hot
What's hot (20)
Similar to brief anatomy of larynx and its clinical evaluation
Similar to brief anatomy of larynx and its clinical evaluation (20)
More from Shraddha Joshi
More from Shraddha Joshi (20)
Recently uploaded
Recently uploaded (20)
brief anatomy of larynx and its clinical evaluation
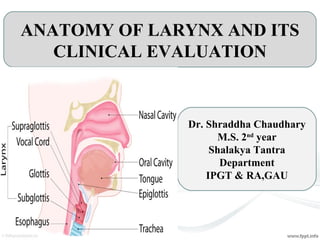
- 1. ANATOMY OF LARYNX AND ITS CLINICAL EVALUATION Dr. Shraddha Chaudhary M.S. 2nd year Shalakya Tantra Department IPGT & RA,GAU
- 2. Anatomy of Larynx • It is a organ of phonation and an air passage. • Extends from root of tongue to trachea. • Lies in front of hypopharynx (opposite to 3rd to 6th cervical vertebrae). • Cartilages: 9 in no. 1. Unpaired: Thyroid Cricoid Epiglottis 2. Paired: Arytenoid Corniculate Cunieform
- 5. • Laryngeal Joints: 2 in no. 1.Cricothyroid joint 2.Cricoarytenoid joint
- 6. • Laryngeal ligaments and membranes: Divided into two: 1. Extrinsic: a. Thyrohyoid membrane b. Cricotracheal Ligament c. Hyoepiglottic Ligament
- 7. • Intrinsic: a. Quadrangular membrane b. Cricovocal membrane c. Cricothyroid Ligament d. Thyroepiglottic ligament
- 8. • Cavities of larynx: Laryngeal cavity starts at laryngeal inlet and ends at lower border of cricoid cartilage, where it continous with lumem of trachea. Two pairs of folds(Vestibular and Vocal) divides the cavity into 3: Vestibule (Supraglottic): Extends from Laryngeal inlet to Vestibular folds. Ventricle (glottis): Deep Elliptical space b/w vestibular folds and Vocal cords. Subglottic space (Infraglottic) : Extends from vocal cords to lower border of cricoid cartilage.
- 9. What complaints we get at Opd level???? • Change in voice • Pain in laryngeal area • Respiratory obstruction • Cough and expectoration • Odynophagia (Painful swallowing) • Dysphagia (Difficulty in swallowing) • FB sensation in throat • Fever • Weight loss • Loss of appetite
- 10. Change in voice/ Disorders of voice • Hoarsness of voice (Roughness of voice) Causes:- Acute inflammations, chronic inflammations, tumors, trauma, paralysis, fixation of cords,etc. • Aphonia (Inability to produce voiced sound) • Functional aphonia/Hysterical Aphonia/Pshycological aphonia More in females(15-30 yrs age) sudden aphonia, unaccompained with laryngeal symptoms • Puberphonia/Mutational Falsetto Voice seen in boys who are emotionally immature. • Diplophonia/Dysphonia Plicae Venticularis(Voice like duet) In this phonation with false vocal cords occurs. Voice is rough, low pitched and unpleasent. Cause: Unilateral complete paralysis of vocal cord. • Phonasthenia (Weakness of voice) Cause : Abuse and misuse of voice. Fatigue of phonatory muscle (Thyroarytenoid & Interarytenoid)
- 11. • Hyponasality/Rhinolalia clausa It is a lack of nasal resonance for the letters/words which are resonated in the nasal cavity. Causes:-Blockage of nose or nasopharynx as in common cold, nasal allergy, nasal polyp, nasal growth, adenoids. • Hypernasality/Rhinolalia aperata It is seen when certain words which have a little nasal resonance are resonated through nose. Causes:- Due to faliure of Nasopharynx to cutoff from oropharynx or abnormal communication b/w oral and nasal cavities. • Stuttering (Abnormal fluency of speech)- Hesitation to start, repetition, prolongation or blocks in the flow of speech. • Phonic spasm In adults who uses their voice professionally. This condition also occurs due to partial paralysis of SLN and RLN. As pt attempt to speak vocal cord firmly pressed together after few words and sound is emitted.
- 12. • Mogiphonia- Ordinary conversation voice is unaffected but proffessional speaking or singing is painful and impossible. • Take history:- (Enquire about) 1.Duration 2.Onset(Gradual/Sudden)- Slow- Acute laryngo tracheo bronchitis Incidious- laryngeal diptheria 3.Loud/Soft 4.Diurnal Variation- in chronic laryngitis pt. become aphonic till the end of the day. 5.Characterstic (Clear/Husky/Hoarse/Hot Potato Voice) 6.Fatigable or not
- 13. Pain in Laryngeal area Causes:- •Epiglottitis •Acute Laryngitis (Due to Dryness and Rawness in throat) •Chronic Laryngitis •Acute Vocal Abuse •Ulceromembranous Laryngitis •Diptheric Laryngitis •Cricoarytenoid Arthritis •Layngeal Trauma •FB •Benign or Malignant tumors Enquire for:- •Duration •Number of attacks per month/year •Recurrence (is there or not)
- 14. Respiratory Obstruction Causes: •Foreign body (Depends on site of FB, Size and Nature of FB) •Vocal cord Paralysis •Glottic oedema •Laryngocele •Malignant growth Enquire for: •Duration:- short term/ long term •Onset:- Sudden or Gradual •Progress:- Progressive or Non-Progressive
- 15. Odynophagia and Dysphagia • Fever can be associated with epiglottitis, laryngitis, glottitis, etc.. Especially evening rise of temprature is suggestive of tuberculosis. • Weight loss and Loss of appetite are the associated complaints may be seen in any malignancy. Enquire for:- Duration Onset- Gradual/Sudden Is it for Liquids/Solids/Semisolids Pain while swallowing H/O FB Causes:- Acute epiglottitis Abcess in epiglottis Laryngeal trauma Contact ulcer Vocal nodules Ulceromembranous laryngitis
- 16. PROPER HISTORY IS MUST…… • After asking chief complaints of the patients start with PAST History. • Ask for past medical history H/o similar illness in the past H/o Pulmonary tuberculosis (as it may cause granulomatous growth over vocal cords) H/o DM, Brochial Asthma, HTN,etc. • Treatment History:- H/o biopsy being taken (if any) H/o Irradiation and its side-effects (if any) • Personal History:- Smoking and alcoholic habits.(they are more prone for laryngeal and hypolaryngeal malignancies.) Weight loss Appetite.
- 17. EXAMINATION • External examination: Lymphnodes examination Adam’s apple Laryngeal Crepitus • Internal Examination: Indirect Laryngoscopy Direct Laryngoscopy Fibroptic Laryngoscopy Rigid Laryngoscopy • Imagning Techniques: X-ray of Neck, Larynx, Pharynx CT-scan MRI PET-CT & PET-MRI
- 18. EXTERNAL EXAMINATION • Start with the Lymphnodes Examination: Nodes are to be palpated while standing at the back of the patient. Neck is slightly flexed to achive relaxation of muscles. Sloan Kettering Cervical LN Classification: Level 1A-Submental lymphnodes Level 1B-Submandibular lymphnodes Level 2-Upper Juglar group nodes Level 3- Middle Juglar group nodes Level 4- Lower Juglar group nodes Level 5A-Superior to cricoid Cartilage Level 5B- Inferior to cricoid cartilage Level 6- (Ant. Compartment) Hyoid bone to Suprasternal notch. Level 7- Tracheoesophageal groove nodes and superior mediastinal nodes.
- 19. Observe the Adam’s apple. An advanced Laryngeal Carcinoma may distort the shape of Adman’s Apple. Laryngeal Crepitus:- It is normal sound produced by the movement of laryngeal cartilage against cervical spine. • Absence of this (Boca’s Sign) may be because of any growth. Widening of larynx (Growth of Pyriform Fossa)
- 20. INTERNAL EXAMINATION Simplest method of Larynx and Vocal cords examination. Most adult and older children. Significant skill and patient co-operation. Larynx examination:- At rest Gental Breathing During phonation Coughing INDIRECT LARYNGOSCOPY:
- 21. Cont…… Diagnostic:- •Change in voice •FB sensation •Odynophagia •Dysphagia •Throat Pain •Stridor, etc. Therapautic:- •FB removal •Intubation •Biopsy of growth in hypopharynx or vocal cords •Placing gastric tube INDICATIONS
- 22. • Contraindication:-No absolute contraindications. But special caution should be taken in Acute Epiglottitis. • EQUIPMENTS REQUIRED: Laryngeal mirror Adequate lighting( ideally a strong headlight) Gauze sponges Local anesthetic (spray or viscous solution) Spirit lamp or hot water A B
- 23. • Technique: This procedure works best in a brightly lit room. Use a headlight or mirror light to direct light parallel to your field of vision. Warm the mirror over an alcohol lamp or with warm water to prevent fogging. The patient should be sitting upright with a straight back, leaning slightly toward you with chin pointing upward (“sniffing position”). Sit to the patient’s side, and be higher than the patient. Apply anesthetic to the patient’s pharynx and ask patient to gargle and spit. Test the temperature of the mirror before commencing the procedure to ensure it is not dangerously hot. Ask the patient to relax and to protude out his or her tongue. Cover the tongue in gauze and pull it with the thumb and middle finger of your nondominant hand. With the patient breathing in and out, direct the mirror into the mouth and toward the back of the throat, making sure the glass side is downward.
- 24. At the back of the throat, press the mirror upward, against the uvula and soft palate. Avoid the gag reflex by not touching the posterior pharyngeal wall or tongue base. Slightly alter the mirror and try various angles to visualize the desired structures. Structures to be examined:- Base of tongue Pyriform fossa Vallecula False cords Epiglottis True cords Areyepiglottic folds Upper 2-3 tracheal rings
- 25. Structures seen on I/L are:- Ant. Part of larynx (Epiglottis, ant. Commissure)- towards top of mirror. Post. Part of larynx ( Arytenoids and Post. Commissure)- seen at lower portion of mirror. Patients right vocal cord is seen on left side of mirror and vice versa.
- 26. • THINGS TO BE EXAMINED:- Epiglottis:- Pinkish-Normal Bright red,swollen- Acute epiglottitis, Laryngitis. Pale, swollen- allergic laryngitis Turban shaped epiglottis- Tuberculosis of larynx. V-shape epiglottis- Lupus Ulcers over epiglottis- Corrosive poisioning, Burns,Malignancy Ventricular Bands: (False Vocal Cords) Should be examined for hypertrophy. In Dysphonia Plicae Ventricularis O/E margins of bands may be seen to approximate to hide true vocal cords.
- 27. PYRIFORM FOSSA:- Fullness of this area- suspicious of malignancy. Pooling of saliva (Jackson’s sign)- suspicious of postcricoid malignancy. VOCAL CORDS:- Pearly white- Normal Congested- Acute Laryngitis Edges should be examined for any growth: Vocal nodules (at junc. of ant, 1/3rd and post 2/3rd of vocal cords). Malignant growth may be seen. Surface should be observed for cyst, ulcer, leukoplakic patch or granulations. Vocal cord movement should be examined at: NORMAL Vocal nodules a. Gentle Breathing- Abduction b. During phonation c. Forced Inspiration- Fully abducted d. On coughing-adduction followed by abduction e. At rest- gently abducted
- 28. Movement of vocal cord is restricted in: Abductor or adductor paresis Any growth in glottis region Cricoarytenoid arthritis
- 29. POSITION OF VOCAL CORDS: Position of Vocal cords Distance from centre Healthy Diseased Median Midline Phonation RLN Paralysis Paramedian 1.5mm Strong Whisper RLN Paralysis Intermediate (Cadaveric) 3.5mm Neutral position Paralysis of RLN & SLN Gentle Abduction 7mm Quite Respiration Paralysis of Adductors Full Abduction 9.5mm Deep Inspiration -
- 30. vocal cord paralysis should be checked according to position and movement:- Types -4 • Unilateral incomplete paralysis • Unilateral complete paralysis • Bilateral incomplete paralysis • Bilateral complete paralysis
- 31. • Some other disease which involves Vocal cords and sorrounding area: Viral Laryngitis:- Laryngeal mucosa is diffusely erythematous, esspecially over the true vocal cords. Simple Diffuse chronic laryngitis:- Examination shows a reddned hyperemic laryngeal mucosa. The true vocal cord looses their white color and becomes pink or red. Keratosis:- The surface of the vocal cord is white in color as a consequence of thickning of the squamous epithelium covered by excess keratin. Laryngitis sicca:- the laryngeal mucosa has dry, glazed, roughned appearance Crusts(yellowish or black in color)- Interarytenoid area. Vocal Nodules Vocal Polyp:- Polyps can be on one or both of the vocal folds. They may look like a swollen spot or bump, a blister, or a thin, long growth.
- 32. Common mistakes we make during procedure….. • Fails to explain procedure. • Fails to position the patient perfectly. • Fails to focus light properly on mirror. • Fails to elevate uvula with back of mirror. • Visualizing larynx directly without looking at adjacent structures.
- 33. DIRECT LARYNGOSCOPY • Direct visualization of larynx and hypopharynx. Indications Diagnostic: Infants and young children Strong gag reflex & overhanging epiglottis Examine hidden areas of Hypopharynx & Larynx Find extent of growth and take biopsy Symptoms- Hoarseness, Dyspnoea, stridor, dysphagia. Therapautic: Removal of benign lesions of larynx FB removal Dilatation of laryngeal strictures.
- 34. • CONTRAINDICATIONS:- Diseases/ Injuries of cervical spine. Stridor (Unless airway provided by tracheostomy) Recent coronary occlusion. Cardiac Decompensation • ANESTHESIA:- Usually done under general Anaesthesia. • EQUIPMENTS:- Consist of:- a. Handle b. Blade Blades:- A. Miller blade:- Straight blade The size of flange is reduced to minimize trauma. Curve at the tip is extended to improve lifting of epiglottis.
- 35. B.Macintosh Blade:- •POSITION:- Curved Blade Tip of blade rests in vallecula, indirectly lifting epiglottis.
- 37. POSTOPERATIVE CARE:- Patient is kept in coma position to prevent aspiration of blood or secretions. Patients respiration should be watched for any laryngeal spasm and cyanosis. Trauma to larynx, especially if repeated attempt at laryngoscopy have been made. May lead to Laryngeal oedema and respiratory distress. Bleeding may occur from operative site. Pt. may spit blood. Care should be taken to prevent aspiration. COMPLICATIONS:- Injury to lips and tongue if they are nipped b/w the teeth and the laryngoscope. Injury to teeth. They may get dislodged and fall into pharynx. Bleeding. Laryngeal oedema.
- 38. Flexible Fibreoptic Laryngoscopy • It is modified technique of direct laryngoscopy. • In difficult cases, where laryngeal examination cannot be performed with mirror due to anatomical abnormlities or intolerance of mirror by the patient, this can be used. • It is passed through the nose under local anasthesia and gives a good view of larynx, laryngopharynx, subglottis, and even upper trachea.
- 39. Rigid Endoscopy • A rigid fiberooptic telescope is used. • It gives a clear, wide-angle view of the larynx and laryngopharynx. • Local anaesthesia may be required for patients with an active gag reflex.
- 40. STROBOSCOPY • The vocal folds vibrate so fast during voice production (over one hundred times a second in men and double that in women) that this vibration is impossible to see clearly with the naked eye. The free edges of the vocal folds appear as a blur. • Stroboscopy is a special method of examination of a vibrating or fast moving object, such as the vocal folds. • A bright flashing light lasting a fraction of a second (10µs) is used to illuminate the vocal folds. This flash ‘freezes’ the movement of the vibrating vocal folds. By taking multiple snapshots at different phases of the vibratory cycle it is possible to see details of the change in shape of pliable surface of the vocal folds.
- 41. IMAGNING TECHNIQUES • X-ray:- Lateral view of neck:- In normal person it shows- outline of base of tongue, vallecula, Hyoid bone, Epiglottis and Aryepiglottic fold, Arytenoids, False and true cords, Cartilages, subglottic space , trachea, Cervical spine. This view helps in diagnosis of: FB of Larynx, Pharynx. Laryngeal stenosis Acute Epiglottitis (Thumb sign) Fracture of larynx and hyoid bone and their displacement. Caries of cervical spine,etc. AP view of neck:- This view is useful to diffrentiate a FB of larynx from that of oesophagus. Also to see any compression or displacement of trachea, bilateral neck masses.