2. • Streptomycin was the first member discovered in 1944 by
Waksman and his colleagues.
• These are a group of natural and semisynthetic antibiotics
containing amino sugars(streptidine, 2-deoxy streptamine,
garosamine) linked to an aminocyclitol ring by glycosidic bond.
• Obtained from variety of soil actinomycetes
• Streptomycin derived from Streptomyces griseus Natural
• Gentamicin from Micromonospora
• Amikacin is a derivative of Kanamycin Semi-synthetic
• Netilmicin a derivative of sisomicin
3. Mechanism of action
• Aminoglycosides are rapidly acting bactericidal agent, and have
concentration dependent killing
• A post antibiotic effect i.e residual bactericidal effect persist even
after serum concentration has fallen below minimum inhibitory
concentration.
• Aminoglycoside diffuse across the outer coat of gram-negative
bacteria through porin channels. Entry from the periplasmic space
across the cytoplasmic membranes is carrier mediated which is
linked to the electron transport chain. Thus, penetration is
dependent upon maintenance of a polarized membrane and on
oxygen dependent active processes (energy dependent phase I or
EDP1 entry).
4. • Aminoglycoside
aqueous channel Porin Protein in outer membrane of
gram negative bacteria
Periplasmic space
Inhibited by divalent cations Energy dependent phase 1(EDP-1)
Ca2+ , Mg2+, hyperosmolarity,
Decrease Ph, Anaerobic condition
Cytoplasmic space
• Anaerobes are not sensitive and facultative anaerobes are more
resistant when O2 supply is deficient, e.g. inside big abscesses.
• Penetration is also favoured by high pH; aminoglycosides are ~20
times more active in alkaline than in acidic medium.
• Inhibitors of bacterial cell wall (β-lactams, vancomycin) enhance
entry of aminoglycosides and exhibit synergism
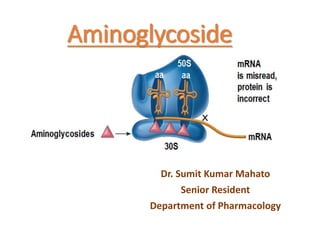
5. • Inside the bacterial cell, streptomycin binds to 30S
ribosomes, but other aminoglycosides bind to additional
sites on 50S subunit, as well as to 30S-50S interface.
• They freeze initiation of protein synthesis,
• Prevent polysome formation and promote their
disaggregation to monosomes so that only one ribosome is
attached to each strand of mRNA.
• Binding of aminoglycoside to 30S-50S juncture causes
distortion of mRNA codon recognition resulting in
misreading of the code.
• Wrong amino acids are entered in the peptide chain and
peptides of abnormal lengths are produced
6.
7. How cidal?
• The cidal action is due to secondary changes in the
bacterial cell membrane.
• This probably results from incorporation of the defective
proteins into the cell membrane.
• After exposure to aminoglycosides, bacteria become
more permeable to ions, amino acids and even proteins
leak out followed by cell death.
9. MECHANISM OF RESISTANCE
Resistance to aminoglycosides is acquired by one of the following
mechanisms:
(a) Acquisition of cell membrane bound inactivating enzymes which
phosphorylate/ adenylate or acetylate the antibiotic.
The conjugated aminoglycosides do not bind to the target ribosomes.
• This is the most important mechanism of development of resistance
to aminoglycosides.
• These enzymes are acquired mainly by conjugation and transfer of
plasmids.
• Susceptibility of different aminoglycosides to these enzymes
differs.
10. (b) Mutation decreasing the affinity of ribosomal proteins that
normally bind the aminoglycoside.
• 50% of streptomycin resistance strain of E.coli is due to this
ribosomal mutation.
• 5% of Pseudomonas aerginosa exhibit similar kind of
streptomycin resistance.
(c) Decreased efficiency of the aminoglycoside transporting
mechanism:
• Either the pores in the outer coat become less permeable or
• The active transport is interfered
11. Absorption:
• These are highly polar basic compounds and are poorly
absorbed from G.I tract. (<1%).
• Long term oral and rectal administration of aminoglycoside
can lead to accumulation to toxic level in patient with renal
impairment.
• All aminoglycoside are absorbed rapidly from intramuscular
injection site reaching peak concentration within 30-90min.
12. Distribution
• Due to polar nature these don’t penetrate into most of the cells,
eye, CNS.
• These do not bind to plasma albumin, except streptomycin.
• Apparent volume of distribution is only 25% of lean body mass.
• Concentration of aminoglycoside in tissue and secretion are low,
but high concentration is found only in renal cortex, endolymph,
perilymph of inner ear.
• This high concentration is most likely cause of ototoxicity and
nephrotoxicity.
• Inflammation increases the penetration into peritoneal and
pericardial spaces
13. • Streptomycin and tobramycin can lead to hearing loss in
children born to those women who receives these drugs
during pregnancy.
Excretion
• Aminoglycoside are excreted almost entirely by glomerular
filtration, a high urinary concentration is achieved i.e. 50-
200µg/ml.
• A large fraction of the parentrally administered dose is excreted
unchanged in the urine within 24 hrs , of which most is excreted
within 12 hrs.
• Half life is about 2-3 hrs in patient with normal renal function.
14. DOSING REGIMENS:
• It have low safety margin,
• Daily dose of aminoglycosides must be precisely calculated
accordingly to body weight and level of renal function.
• For an average adult with normal renal function (CLcr >70
ml/min), the usual doses are:
• Gentamicin/tobramycin/sisomicin/netilmicin - 3–5 mg/kg/day
• Streptomycin/ kanamycin/amikacin 7.5–15 mg/kg/day
15. SHARED TOXICITIES
The aminoglycosides produce toxic effects which are common to all
members, but the relative propensity differ.
1. Ototoxicity: This is the most important and related to dose and
duration of treatment.
• The vestibular or the cochlear part may be primarily affected by a
particular aminoglycoside.
• These drugs are concentrated in the labyrinthine fluid and are
slowly removed from it when the plasma concentration falls.
• Ototoxicity is greater when plasma concentration of the drug is
persistently high and above a threshold value.
• Ototoxicity can happen when it is instilled in patients with
perforated eardrum, so it is contraindicated in them.
16. Cochlear damage:
It starts from the base and spreads to the apex; hearing loss affects
the high frequency sound first, then the lower frequencies are
affected.
• Initially, the cochlear toxicity is asymptomatic and can be detected
only by audiometry then Tinnitus appears, followed by progressive
hearing loss.
• No regeneration of the sensory cells occurs.
• Deafness is permanent.
Vestibular damage:
• Headache appears first , followed by nausea, vomiting, dizziness,
nystagmus, vertigo and ataxia.
• Most symptoms subside in two weeks except ataxia which may
persist for 1–2 years.
KAN (Kanamycin, Amikacin, Neomycin) mainly damage
cochlea rest vestibular damage
17. 2. Nephrotoxicity:
• Aminoglycosides attain high concentration in the renal cortex
(proximal tubules) and toxicity is related to the total amount of the
drug received by the patient.
• More common in the elderly and in those with preexisting kidney
disease.
• It manifests as tubular damage resulting in loss of urinary
concentrating power, low g.f.r, nitrogen retention, albuminuria and
casts.
• Renal damage caused by aminoglycosides is totally reversible.
• It has been postulated that aminoglycosides interfere with the
production of PGs in the kidney which is causally related to the
reduced g.f.r
Verapamil and Ca++ can
Reduce nephrotoxic potential But
Also reduce antibacterial effect
18. 3. Neuromuscular blockade:
• Aminoglycosides reduce ACh release from the motor nerve endings.
• They interfere with mobilization of centrally located synaptic
vesicles to fuse with the terminal membrane.
• Decrease the sensitivity of the muscle endplates to ACh.
• The neuromuscular block produced by aminoglycosides can be
partially antagonized by i.v. injection of a calcium salt.
• More with Neomycin and Streptomycin
Dangerous in
Myasthenia gravis
Direct administration of Aminoglycosides into pleural and peritoneal
cavities
If patient received curare like muscle relaxant during surgical procedure
20. Gentamicin:
• Obtained from Micromonospora purpurea in 1964.
• Aminoglycoside of first choice because of lower cost and reliable
activity against all but most resistant gram negative aerobes
• It is active mainly against aerobic gram negative bacilli, including E.
coli, Klebsiella pneumoniae, Enterobacter, H.influenzae, Proteus,
Serratia and Pseudomonas aeruginosa.
• Many strains of Brucella, Campylobacter, Citrobacter, Fransisella
and Yersinia are also sensitive.
• It has low therapeutic index, so its use is restricted to serious gram-
negative bacillary infections.
21. 1. Gentamicin is very valuable for preventing and treating
respiratory infections in critically ill patients.
2. Pseudomonas, Proteus or Klebsiella infections: burns, urinary
tract infection, pneumonia, lung abscesses, osteomyelitis, middle
ear infection, septicaemia, etc., caused mostly by the above
bacteria and are an important area of use of gentamicin.
3. Meningitis caused by gram negative bacilli.
4. Subacute bacterial endocarditis (SABE): Gentamicin (1 mg/kg 8
hourly i.m.) is generally combined with
penicillin/ampicillin/vancomycin
22. Tobramycin:
• Obtained from S. tenebrarius in the 1970s.
• The antibacterial and pharmacokinetic properties, as well as
dosage are almost identical to gentamicin, but it is 2–4 times more
active against Pseudomonas and Proteus.
• Used only as an alternative to gentamicin, Serious infections caused
by Pseudomonas and Proteus
• Ototoxicity and nephrotoxicity is probably less than gentamicin.
• Dose: 3–5 mg/kg day in 1–3 doses
23. Amikacin:
It is a semisynthetic derivative of kanamycin.
It resembles in pharmacokinetics, dose and toxicity to Kanamycin
• Broadest spectrum of activity
• Because of its resistance to many of aminoglycosides – inactivating
enzymes , has a role for treatment of serious nosocomial gram
negative bacillary infection.
• Serratia, Proteus, Pseudomonas, Klebsiella, enterobacte and E.coli
• Less active than gentamicin against Enterococci
• Active against Mycobacteria, but used only for multidrug
resistant infection
• Dose is 15mg/kg/day as a single dose
• Cochlear > vestibular
24. Streptomycin:
• Oldest aminoglycoside antibiotic obtained from Streptomyces griseus.
Used extensively in the past, but is now restricted to treatment of
tuberculosis.
• The antimicrobial spectrum of streptomycin is relatively narrow. About
1/5 patients given streptomycin 1 g BD i.m. experience vestibular
disturbances. Auditory disturbances are less common.
• Streptomycin has the lowest nephrotoxicity among aminoglycosides.
Uses:
1. Tuberculosis
2. Subacute bacterial endocarditis (SABE)
3. Plague
4. Tularemia
• Deep IM
• Dose 15 to 25 mg/kg
• Vestibular > cochlear , irreversible
25. Neomycin:
• Obtained from S. fradiae,
• It is a wide-spectrum aminoglycoside, active against most gram
negative bacilli and some gram-positive cocci.
• Pseudomonas and Strep. pyogenes are not sensitive.
• Spectrum of activity against E.coli, Enterobacter, Klebsiella, Proteus
• Neomycin is highly toxic to the internal ear (mainly auditory) and to
kidney.
• It is, therefore, not used systemically.
Oral neomycin has damaging effect on intestinal villi-
Malabsorption syndrome.
Damages colonic flora- deficiency of vit. K
Superinfection
26. Uses:
1. Most common use is topical, ointment, eye and ear drops
2. Orally for:
(a) Preparation of bowel before surgery: 3 doses of 1.0 g along
with metronidazole 0.5 g on day before surgery) may reduce
postoperative infections.
(b) Hepatic coma or or Hepatic Encephalopathy
3. Neomycin with Polymyxin-B solution is used as an irrigant in
urinary bladder to prevent bacteriuria associated with use of
indwelling catheter
27. Paramomycin:
• Chemically related to neomycin.
• It is active against many protozoan parasites, including
E. histolytica, Giardia lamblia, Trichomonas vaginalis,
Cryptosporidium and Leishmania, in addition to many bacteria
sensitive to neomycin
• It can be used as an alternative to neomycin for hepatic
encephalopathy.
• Parenterally, it is being used for visceral leishmaniasis, topical use
for cutaneous leishmaniasis
28. Kanamycin:
• Obtained from S. kanamyceticus (in 1957), it was the second
systemically used aminoglycoside to be developed after
streptomycin.
• It is more toxic, both to the cochlea and to kidney.
• Hearing loss, which is irreversible, is more common than vestibular
disturbance.
• It is similar to streptomycin in all respects including efficacy against
M. tuberculosis and lack of activity on Pseudomonas.
• It is occasionally used as a second line drug in resistant tuberculosis.
Dose: 0.5 gm i.m. BD (15 mg/kg/day);
29. Precautions in using aminoglycosides
Do not mix aminoglycosides with any other drug in the same syringe.
Avoid use of other ototoxic drugs like loop diuretics with aminoglycosides.
Avoid use of other nephrotoxic drugs like amphotericin B, cephalothin and
cisplatin with aminoglycosides.
Avoid use of drugs having muscle relaxant action along with
aminoglycosides.
Use cautiously in the elderly, in renal damage and in combination with
skeletal muscle relaxants.
Contraindicated in pregnancy because of the risk of deafness in the child.
Determination of plasma levels of aminoglycosides may be needed in severe
infections and in patients with renal dysfunction.