Dandy Walker syndrome
•Download as PPTX, PDF•
48 likes•23,359 views

The Dandy-Walker complex is a rare congenital brain malformation characterized by cystic dilation of the 4th ventricle and partial or complete absence of the cerebellar vermis. It ranges from mega cisterna magna to Dandy-Walker variant to Dandy-Walker malformation based on severity. Associated anomalies are common. The cause is unknown but likely involves abnormal development of the hindbrain. Treatment involves managing hydrocephalus, often with shunt procedures. Prognosis depends on severity and associated anomalies, with higher mortality and developmental delays in more severe forms.

Recommended
More Related Content
What's hot
What's hot (20)
Similar to Dandy Walker syndrome
Similar to Dandy Walker syndrome (20)
More from suresh Bishokarma
More from suresh Bishokarma (20)
Recently uploaded
Recently uploaded (20)
Dandy Walker syndrome
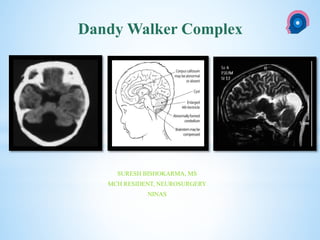
- 1. cka SURESH BISHOKARMA, MS MCH RESIDENT, NEUROSURGERY NINAS Dandy Walker Complex
- 2. The Dandy-Walker complex is a rare congenital intracranial malformation that comprises a spectrum of abnormalities of the posterior fossa which are classified as 1. Dandy-Walker malformation (cystic dilatation of the 4th ventricle, complete or partial agenesis of the cerebellar vermis and an enlarged posterior fossa) 2. Dandy-Walker variant (cystic posterior fossa mass with variable hypoplasia of the cerebellar vermis and no enlargement of the posterior fossa) 3. Mega cisterna magna (enlarged cisterna magna with normal cerebellar vermis) Dandy-Walker complex
- 3. It is a continuum of posterior fossa cystic abnormalities with varying degrees of vermian agenesis. Mega cisterna magna Dandy-Walker variant Dandy-Walker malformation
- 4. • DWM and DWV cases show so many similarities that a clear-cut distinction is difficult. • There was no significant difference in the spectrum of associated anomalies and postnatal prognosis between DW and DWV cases
- 5. • Specific size criteria to denote a normal-sized posterior fossa and vermian hypoplasia are not established in the literature. • DWV: The cerebellar hemispheres may be small but morphologically normal
- 6. • The severity of the diagnosis is based on the size of the posterior fossa, the presence of cystic dilatation of the fourth ventricle, and the degree of vermian hypoplasia.
- 7. • First described in 1914 by W Dandy and K Blackfan and was designated as Dandy-Walker syndrome in 1954 by C Benda History
- 8. • The precise aetiology is unknown. The reported incidence varies between one per 2500 births to one per 100,000 births. Environmental factors including viral infections, alcohol and diabetes have also been suggested to play a role in the genesis of Dandy-Walker malformation but the evidence is uncertain Epidemiology
- 9. • The cerebellum is formed by 2 distinct germinal matrices; 1 periventricular and 1 along the rhombic lip, which gives rise to the cerebellar hemispheres. • The cerebellar vermis develops as a thickening of the midline primordium of the rhomboencephalon during the 5th gestational week. By 16 weeks, the vermis fold and begins to cover the roof of the fourth ventricle. By 19 weeks of gestation the cranial/caudal length of the vermis is equal to that of the cerebellar hemisphere. Embryology
- 10. • The pathophysiological mechanism underlying the Dandy–Walker complex is not clearly elucidated. Initially, it was proposed that congenital obstruction of the foramina of Luschka and Magendie resulted in cystic dilatation of the fourth ventricle and the resulting malformed posterior fossa. In later studies investigators have suggested that it is a manifestation of abnormal development of the rhomboencephalon, with incomplete formation of the vermis, or due to a defect within the tela choroidea, which leads to cystic dilation of the fourth ventricle. Given its comparable appearance to DWM, it is likely that DWV develops along the same embryological pathway. One is embryonic arrest of the rhombencephalon, with failure of cerebellum fusion in the midline between weeks 7 and 10 of gestation. This leads to persistence and interposes itself between the hypoplastic vermis and the choroid plexus. Furthermore, the roof of the fourth ventricle expands upward through an agenetic corpus callosum. • Chromosomal abnormalities were observed in this study and included defects on chromosomes 9, 11, 13, and 8. Deletions on chromosome 8; a long-arm deletion of chromosome 3 was observed in a patient with DWV and associated craniofacial anomalies; and partial trisomy 3 and monosomy 11 (a partial imbalance of chromosomes 6 and 11) have also been described. The gene locus for DWM is 3q24. • Trisomy-18, tri- ploidy and trisomy-13. pathophysiology
- 11. • Developmental Status • Poor developmental outcome in association with posterior fossa malformations is reported in 55–100% of patients. • It is estimated that moderate-to-severe developmental delay is observed in approximately one-third of patients with DWM, and • of those 11–16% have a diagnosis of severe delay and require significant assistance in their daily functioning. • Hydrocephalus is common prenatally or during the neonatal period, although this is a complication rather than part of the disease. Most cases are diagnosed during infancy. • Older patients might be asymptomatic, with normal or near-normal neurological examinations. They usually pre- sent with neurological manifestations such as developmental delay, spasticity, poor head control and seizures.12 Some children present with symptoms suggestive of increased intracranial pressure and posterior fossa tumour, like nystagmus, cranial nerve palsy or truncal ataxia. Clinical presentation
- 12. INTRACRANIALANOMALIES: 1. Brainstem dysplasia 2. Agenesis of corpus callosum 3. Holoprosencephaly 4. Occipital encephaloceles Two thirds of patients have associated central nervous system abnormalities. Association EXTRACRANIAL ANOMALIES 1. The incidence of extracranial anomalies was 54% in DWV, compared with the 12–86% reported in patients with DWM 2. Genitourinary: polycystic kidneys 3. Musculoskeletal systems: polydactyly 4. Gastrointestinal: 5. Ocular abnormalities The severity of Dandy Walker syndrome depends on the presence of associated anomalies. DWV has been associated with Menkes syndrome (kinky-hair disease), Coffin–Siris syndrome, and Ehlers–Danlos syndrome, as well as neurocutaneous melanosis
- 13. Retrocerebellar arachnoid cyst underlying brain is normal. The cerebellar hemispheres are not separated by a cystic mass, rather displaced en-bloc. Diagnosis The diagnosis is challenging because of a lack of specific symptomatology. Unless the syndrome is detected prenatally, by ultrasound or magnetic resonance imaging or increased head circumference (prenatally or postnatally) Definitive criteria have not been firmly established. The prenatal differentiation between Dandy-Walker variant and mega-cisterna magna should be made with caution, especially in the early second trimester because the relatively large fourth ventricle and the incompletely formed inferior cerebellar vermis may give a false impression of vermian defect and a follow-up scan at 18 weeks or later should be done. Cisterna magna: Depth greater than 10 mm. DWM: thin communication is found between the fourth ventricle and the cisterna magna
- 14. • The treatment of Dandy Walker syndrome consists of dealing with hydrocephalus by various approaches, although this is still controversial. • Membrane excision was initially proposed by Dandy for the treatment of DWM. • The results using this form of therapy have been poor initially, with a high failure rate. mortality rate of 10% and a failure rate of 70%. • Few still advocate this treatment by way of cyst wall excision in children aged over 3 years.* • Endoscopic third ventriculostomy may be considered an acceptable alternative, especially in older children, with the aim to reduce the shunt- related problems. • Endoscopic methods of transaqueductal placement of a single-catheter cyst- ventriculoperitoneal shunt has also been noted to be with good results. Treatment * Udvarhelyi and Epstein
- 15. • The prognosis depends largely on the associated anomalies. • The mortality rate ranges from 27% to 50%, and hearing and/or visual problems are associated with poor intellectual development. Prognosis
- 16. • Recurrence risk in subsequent pregnancies of 1-5% is suggested. Genetic counselling
- 17. Thank you NATIONAL INSTITUTE OF NEUROLOGICAL AND ALLIED SCIENCES, BANSBARI, KATHMANDU DANDY-WALKER COMPLEX NATIONAL INSTITUTE OF NEUROLOGICAL AND ALLIED SCIENCES, BANSBARI, KATHMANDU
Editor's Notes
- Developmental anomalies of the posterior fossa